

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A mixture of 3:1 chloromethylisothiazolinone (CMIT) and methylisothiazolinone (MIT) under the brand name Kathon CG has been extensively used in water-based industrial products and cosmetic applications as a preservative.1 Currently, various types of products are registered for its incorporation, including adhesives, coatings, fuels, metalworking fluids, resin emulsions, paints, and various other specialty industrial products. It is also applied as a microbicide in pulp/paper mills, cooling water systems, oil field operations, industrial process water, and air washer systems. It is also used as a disinfectant in household and individual hygiene products such as shampoo, hair rinse, disposable hand disinfectants, cosmetics, and more.23
A total of 41 household humidifier disinfectant (HD) products were reported to have been marketed in South Korea from 1994 through 2011. The use of HD was then banned because a number of HD users developed fatal health effects, including lung injury.4 In particular, people who used HD products containing polyhexamethylene guanidine phosphate (CAS No. 89697-78-9, PHMG), oligo(2-(2-ethoxy) ethoxyethyl guanidinium (CAS No. 374572-91-5, PGH), or a mixture of CMIT/MIT have complained of various respiratory health problems, including lung injury. The use of these HD products has been clinically confirmed to cause lung disease with widespread lung fibrosis, termed elsewhere as humidifier disinfectant-associated lung injury (HDLI).56 Most of the patients complained of cough and dyspnea, but some progressed rapidly and developed symptoms akin to severe acute respiratory distress syndrome. From 2013 to date, the HDLI Investigation and Decision Committee (HDLIIDC) has been in operation to evaluate registered patients who were presumed to have developed lung injuries due to HD clinically associated with HD use.
This study aims to discuss major issues in assessing inhalation exposure to a mixture of CMIT/MIT contained in HD products, estimating their deposition into the lower part of the respiratory tract, and evaluating the risk of HDLI, including interstitial lung disease (ILD).
Go to : 
METHODS
This study was based on a literature review, focusing on literatures dealing with the inhalation risk of HD containing a mixture of CMIT and MIT. Government documentation, research reports, and manuscripts related to the aims of this study were summarized and reviewed. The major contents include the physicochemical properties of CMIT and MIT contained in HDs, sampling and analytical methods to quantify airborne CMIT and MIT, inhalation animal tests to examine the toxicity of CMIT/MIT, and clinical cases related to inhalation exposure to CMIT and MIT. Since an insufficient body of papers reporting inhalation exposure risk and accordingly respiratory health effects has been published in peer-reviewed outlets, government documentation and official but not peer-reviewed research reports were also included.
Go to :
RESULTS AND DISCUSSION
The emergence of HDs containing a mixture of CMIT/MIT
The basic physicochemical properties of CMIT and MIT, including CAS No., chemical formula, molecular weight (g/mole), density (g/cm2), level of water solubility, and usage have been published elsewhere.789 A total of 11 HD products containing a 3:1 mixture of CMIT and MIT had been marketed by the end of 2011 when a number of HDLI patients were reported and the sale of HD was banned. SKYBIO FG, a 1.5% solution of a 3:1 blend of CMIT and MIT, was reported to be diluted in order to manufacture these HDs. Magnesium nitrate (20–25%), magnesium chloride (0.2–1.0%), and water (70–75%) were also included in the HD products (Table 1).47 Park et al.7 estimated the concentration of CMIT and MIT dissolved in HD products to be approximately 112.5–225 ppm for CMIT and 7.5–22.5 ppm for MIT. SKYBIO FG appears to be similar to the product commercially manufactured and sold under the name of Kathon CG.1 Companies promoted their HD products to incite consumers to purchase them. Several phrases such as “for your baby,” “fresh air,” and “refreshing air” that lack a scientific basis were widely used in their advertisements.410 The concentration of CMIT and MIT and the market volume and sales period by type of HD have been reported in detail elsewhere, although there is no data on HD products manufactured prior to 2004.47 Data on the number of people who used HD products containing CMIT and MIT has not been published.

Table 1
Ingredient compositions of a humidifier disinfectant brand (SKYBIO FG) containing a mixture of CMIT and MIT
| Name of ingredient | CAS No. | Proportion, %a |
|---|---|---|
| CMIT | 26172-55-4 | 1.0–2.0 |
| MIT | 2682-20-4 | 0.2–0.6 |
| Magnesium nitrate | 10377-60-3 | 21–25 |
| Magnesium chloride | 7886-30-3 | 0.5 |
| Water | N/A | 72–77 |
CMIT = chloromethylisothiazolinone, MIT = methylisothiazolinone, N/A = not available.
aConcentration of ingredient: 1% = 10,000 ppm.
![]()
Health risks associated with the use of HDs containing a mixture of CMIT/MIT
With their strong corrosive properties, CMIT/MIT can also be fatal through skin contact or inhalation (H330, H331), depending on the size of the dose exposed or inhaled. The most frequently reported health effect is skin disease such as skin irritation and allergic skin diseases,10 observed mainly among cosmetics users. Due to these health risks and toxicities, many countries, including South Korea, have banned CMIT, MIT, or a mixture of the two for leave-on cosmetics and restricted them in rinse-off cosmetics.11 Among the 453 victims registered as of 2017, HD products containing only PHMG were the most frequently used among HDLI patients (n = 234, 52%), followed by PGH (n = 27, 6%) and a mixture of CMIT and MIT (n = 26, 6%).12 This study summarized HDLI statistics associated with the type of HDs containing CMIT and MIT (Table 2). The government has provided financial support to HDLI patients as advance relief and has exercised the right to indemnity relief funds from the industry manufacturing HDs. No lung injuries like ILD and HDLI have been reported to be caused by CMIT and/or MIT contained in products other than HD.

Table 2
Summary of HDLI cases associated with the use of HD a mixture of CMIT and MIT12
HD = humidifier disinfectant, HDLI = humidifier disinfectant-associated lung injury, PHMG = polyhexamethylene guanidine phosphate, PHMG-H = polyhexamethylene guanidine hydrochloride, PGH = oligo (2-(2-ethoxy) ethoxyethyl guanidinium, CMIT = chloromethylisothiazolinone, MIT = methylisothiazolinone.
![]()
Airborne CMIT and MIT
Type of airborne CMIT and MIT
According to the material safety and data sheets (MSDS) provided by the HD manufacturers, the mixture of CMIT and MIT are likely entrapped with magnesium salts in the HDs, preventing them from evaporating quickly (Table 1). When HD is used in a residential environment such as a small room, most of the CMIT and MIT dissolved in the humidifier is dispersed into the air and remains for a certain time in the small room, where the ventilation is low or lacking, especially during winter or sleep. This study assumed that there are two types of CMIT and MIT when they are dispersed into air and deposited in the respiratory tract: a gaseous substance and particles mixed with magnesium salts.
Firstly, in consideration of the semi-volatile nature of CMIT/MIT (vapor pressure CMIT; 2.39 Pa, MIT 0.41 Pa at 25°C),213 it is common for them to evaporate into the air. Both the respiratory tract and skin, including on the face, are consecutively exposed to airborne CMIT and MIT as long as it is being sprayed in the air through a household humidifier, which is conventionally placed within a couple of meters of users within a room. Airborne contact dermatitis reported to be caused by the emission of CMIT or MIT from paint or industrial products has become more prevalent in recent years.14151617 Inhalation of CMIT or MIT may also cause asthmatic reactions.151617 These studies indicated that CMIT and MIT contained in industrial or household products can be dispersed into the air in a gaseous or aerosols state through evaporation or dispersion during usage and can be inhaled into the respiratory tract.
Secondly, CMIT/MIT entrapped with other salt compounds in HD can be dispersed into the air as particles mixed with magnesium nitrate. The mass median aerodynamic diameter of airborne aerosol dispersed from the use of HD products containing a mixture of CMIT and MIT was measured to be lower than 2 μm.18 Arguably, these tiny particles of CMIT/MIT can reach the alveoli, as hinted at in studies that have illustrated how substances in tap water are condensed and turn into white dust in the air, causing pneumonia.19 It is required to assess inhalation exposure considering a range of factors, such as the characteristics of this mixture of chemicals, humidifier users’ behaviors, and indoor environments with insufficient ventilation.
Techniques to collect and quantify airborne CMIT and MIT
As far as we reviewed, no study has reported on airborne CMIT and MIT in the indoor and residential environment based on detailed descriptions about sampling and analytical techniques. Park et al.20 reported that airborne CMIT/MIT sampled using two serial impingers containing deionized water (DI) in room-scale chamber studies were respectively 35.5% and 77.9% of the theoretical level (μg/m3). The recovery rates (mean ± standard deviation, %) of the amount at 1.00 and 10.0 μg/L injected into DI in an impinger were 35.5 ± 8.8% and 77.9 ± 22.2% for CMIT and MIT (n = 6), respectively. The recovery rate of airborne CMIT and MIT analyzed by liquid chromatography-mass spectrometry in this study was reported to be low and inconsistent, indicating larger discrepancies between that was measured by impinger sampling and that was calculated without considering any decay processes. To date, no sampling or analytical method has been verified to quantify airborne CMIT and MIT. Park et al.7 estimated the inhalation exposure levels of combined CMIT and MIT among the HDLI patients to be in the range from 0.3 to 8.1 μg/m3. The characteristics of CMIT and MIT with their high water solubility, reactive properties, and vapor pressure make it very difficult to collect and quantify them.20 Proper sampling media for collecting airborne isothiazolinones such as CMIT and MIT, solvents for extraction from sampling media, and analytical techniques should all be studied. Daftary and Deterding (2011)19 suggested that the existing risk assessments for cosmetic and industrial products that contain MI should be evaluated considering the accurate quantification of airborne CMIT and MIT levels.
Threshold limit values for CMIT and MIT
No airborne threshold level for CMIT and/or MIT has been set for residential environment exposure. The US Environmental Protection Agency (EPA) recommended an airborne no observable effect level (NOEL) of 0.34 µg/L.2 This value was estimated around 1994 based on the results of inhalation animal testing. In addition, safety factors that depend on the reliability of the data used for extrapolation, ranging from 10 to 1,000, are not considered in this criterion. Furthermore, this criterion for workers cannot be applied to residential exposure for all groups of people, including biologically susceptible groups such as children, pregnant women, the elderly, and patients.
Deposition of CMIT/MIT in the lower part of the respiratory tract based on clinical results
It could be assumed that it would be hard for CMIT and MIT to reach the lower part of the respiratory tract because they are water-soluble chemicals, and then are generally intercepted in the upper part of the respiratory system. This assumption can be broadly applied to non-reactive gaseous chemicals, but cannot be directly applied to CMIT and MIT with their corrosive properties and coexisting with other salts. CMIT/MIT does not exist alone in HD products, but is mixed with a significant amount of magnesium nitrate (25%) added as a stabilizer. The properties of CMIT/MIT alone cannot determine their airborne occurrence and respiratory absorption.21 Many clinical studies and case reports have demonstrated that CMIT and MIT reach the lower respiratory and cause health effects including HDLI and asthma.2021
Key results from three studies that examined clinical features from HDLI pediatric patients who responded to use only HD containing CMIT and MIT are summarized (Table 3).222324 Lee et al.72223 reported that two sisters and one HDLI patient who used only an HD brand containing a mixture of CMIT and MIT showed the typical rapid progression of respiratory difficulty, starting from a mild cough or tachypnea, similar to HDLI caused by exposure to PHMG or PGH. This study showed an assumption that airborne CMIT/MIT dispersed from HD could reach the alveoli part and cause lung injury. PHMG and PGH with their high solubility were contained in other HD products and were found to reach the lower respiratory tract and cause lung injury.7 PHMG is also a polycationic agent and shows structural similarity with the agents that caused the Ardystil syndrome that appeared first in Spain (mainly in a factory named Ardystil). This syndrome shares common clinical and pathologic features, especially the bronchiolocentric distribution of the interstitial lung lesions, because they were caused by the inhalation of agents of a similar nature, namely, polycationic compounds.25 In addition, there have been many water-soluble chemicals that have been known to cause health effects in the lower respiratory tract, such as asthma, chronic obstructive pulmonary disease, ILD, and lung cancer. They include ozone, nitrogen oxide, phosgene, sulfur oxide, pesticides, aldehydes, and therapeutic drugs.262728
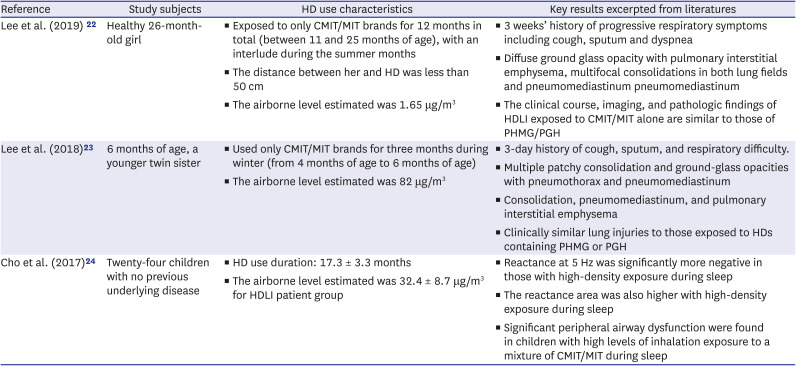
Table 3
Key results on clinical features for HDLI patients who responded to use only humidifier disinfectants containing CMIT/MIT
| Reference | Study subjects | HD use characteristics | Key results excerpted from literatures |
|---|---|---|---|
| Lee et al. (2019)22 | Healthy 26-month-old girl | ▪ Exposed to only CMIT/MIT brands for 12 months in total (between 11 and 25 months of age), with an interlude during the summer months | ▪ 3 weeks’ history of progressive respiratory symptoms including cough, sputum and dyspnea |
| ▪ The distance between her and HD was less than 50 cm | ▪ Diffuse ground glass opacity with pulmonary interstitial emphysema, multifocal consolidations in both lung fields and pneumomediastinum pneumomediastinum | ||
| ▪ The airborne level estimated was 1.65 μg/m3 | ▪ The clinical course, imaging, and pathologic findings of HDLI exposed to CMIT/MIT alone are similar to those of PHMG/PGH | ||
| Lee et al. (2018)23 | 6 months of age, a younger twin sister | ▪ Used only CMIT/MIT brands for three months during winter (from 4 months of age to 6 months of age) | ▪ 3-day history of cough, sputum, and respiratory difficulty. |
| ▪ The airborne level estimated was 82 μg/m3 | ▪ Multiple patchy consolidation and ground-glass opacities with pneumothorax and pneumomediastinum | ||
| ▪ Consolidation, pneumomediastinum, and pulmonary interstitial emphysema | |||
| ▪ Clinically similar lung injuries to those exposed to HDs containing PHMG or PGH | |||
| Cho et al. (2017)24 | Twenty-four children with no previous underlying disease | ▪ HD use duration: 17.3 ± 3.3 months | ▪ Reactance at 5 Hz was significantly more negative in those with high-density exposure during sleep |
| ▪ The airborne level estimated was 32.4 ± 8.7 μg/m3 for HDLI patient group | ▪ The reactance area was also higher with high-density exposure during sleep | ||
| ▪ Significant peripheral airway dysfunction were found in children with high levels of inhalation exposure to a mixture of CMIT/MIT during sleep |
CMIT = 5-chloro-2methylisothiazol-3(2H)-one, MIT = 2-Methylisothiazol-3(2H)-one, HDLI = humidifier disinfectant-associated lung injury, PHMG = polyhexamethylene guanidine, PGH = oligo-(2-)ethoxyethyl guanidine chloride.
![]()
Only one case of asthma due to inhalation exposure to CMIT or MIT has previously been reported. A chemical plant operator aged 53 who worked for five months in a CMIT/MIT manufacturing plant was reported to have developed asthma.29 His job was to fill containers with CMIT/MIT. He developed nasal irritation, cough, wheeze, and chest tightness starting 4–6 hours into his shift and persisting into the evening, with sleep disturbance at night. Out of a total of 20 workers, two others also reported to develop symptoms of asthma after beginning employment.29 Airborne levels of CMIT and MIT monitored in the manufacturing ranged from 0.01 to 0.3 mg/m3, but no description of the sampling and analytical methods applied was provided. These levels are within the range (0.66–118 µg/m3) reported by Park et al. (2020),7 who estimated airborne levels based on the amount of HD used (mL), room size (m3), and assumed ventilation level.
The possibility of chemicals, including CMIT and MIT, reaching and being deposited in part of the respiratory tract cannot be generalized by only the level of water solubility. In addition, the presence and levels of mixed or co-existing substances, their reactivity and airborne levels may affect not only the type of respiratory health problems, but also the part of the respiratory tract that chemicals reach and in which they are deposited. Many aerosols are deposited in the respiratory tract depending on the size, density, shape, charge, and surface properties of the particles, and also on the breathing pattern of the individual.30
Inhalation animal testing for examining toxicity of a mixture of CMIT/MIT
A total of four series of inhalation tests on rats were conducted in South Korea and found that CMIT and MIT did not cause interstitial lung disease.313233 The level of particles measured by the filter method ranged in this study from 1.8 mg m−3 for a day to 50.0 mg m−3 for a day. The US EPA reported that the toxicity of CMIT/MIT led to upper respiratory sinusitis in a 13-week inhalation animal experiment, but systemic toxicity could not be observed due to the strong corrosive nature of this substance.34 The actual airborne level of CMIT and MIT formed during animal testing is unknown. Song et al.35 reported that intra-tracheal installation of Kathon containing a mixture of CMIT and MIT induced fibrotic lung injury following direct lung exposure in a mouse animal model, demonstrating that a mixture of CMIT and MIT causes lung fibrosis in the alveoli part of the respiratory tract if it reaches it. In terms of strict causality during the criminal proceedings, the court gave precedence to inhalation animal testing results that did not find lung injury toxicity over the multiple human HDLI victims who used HD products.
There are inevitable limitations and uncertainties in extrapolating the health effects on humans from animal test results, which is why human cases are prioritized in the risk assessment of chemicals and establishment of regulatory standards by the European Union and International Agency for Research on Cancer. Animal test results are never required as a condition or used as evidence proving or disproving a chemical’s health effects on humans. It seems very hard to develop an inhalation animal testing environment causing lung injury within 90 days without the death animal tested since a mixture of CMIT and MIT is very corrosive and likely volatile. This study recommends that an airborne mixture of CMIT and MIT, not an HD product, be administered to an animal to examine whether these materials can cause interstitial lung injuries.
Epidemiological study for inhalation health risk by HD containing a mixture of CMIT and MIT
Kim et al.36 reported on the odds ratio (OR) of asthma and interstitial pneumonitis incidence between after and before the use of HDs containing a mixture of CMIT and MIT (Table 4). Using data from the National Health Insurance Corporation on 4,206 reported HD victims (of whom 303 applicants for damage were recognized as exclusive CMIT/MIT product users), this epidemiological study compared and analyzed the incidence of asthma and ILD one year, three years, and five years before and after the start of use of the product. Since the initial hospitalization of exclusive CMIT/MIT users due to asthma, the incidence rate surged by 5.1 times, 5.6 times, and 8.7 times between one year, three years, and five years after using, respectively (P <0.05). The odds ratio (OR) for ILD included “1” in the 95% confidence interval, but was 4.1 times higher than the OR before HD use (P <0.05). The court also dismissed these results, requiring case-control epidemiological studies including the risks of ILD developed from a control group that has not used HD. Childhood ILD is a heterogeneous group of rare chronic respiratory disorders in children. The incidence of childhood ILD was reported as 3.6 cases per million in the United Kingdom and Ireland in 2002,37 similar to a German study which estimated an incidence of 0.13 cases per million children less than 17 years of age in 2009.38 It is almost impossible to examine the ILD risk from CMIT and MIT by epidemiological study since ILD, especially childhood ILD has been regarded as rare. Nonetheless, the court demanded the determination of the difference in ILD risk between populations who used HD and who did not use HD.
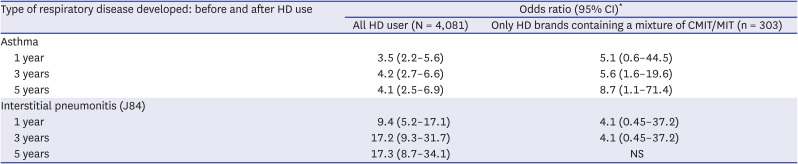
Table 4
Odds ratios of asthma and interstitial pneumonitis incidence between without and with HD brands containing a mixture of CMIT/MIT use in all HD users and CMIT/MIT only users36
HD = humidifier disinfectant, CI = confidence interval, CMIT/MIT = 5-chloro-2methylisothiazol-3(2H)-one/2-methylisothiazol-3(2H)-one, NS = not significant.
*P < 0.05.
![]()
Individual causality of lung injury with the use of HD containing a mixture of CMIT and MIT
An analysis of individual causality can be useful rather than general epidemiological study when examining the risk of a rare disease like ILD. Park et al.39 analyzed individual causality of lung injury with the use of HD containing CMIT and MIT, examining the likelihood of HDLI due to other factors, including occupational exposure, genetic factors, etc. A total of eight out of eleven HDLI patients were children under six years old. Three of them were diagnosed with lung damage based on tissue pathology, and two had product containers left over from use. The authors concluded that CMIT/MIT-containing HDs irrefutably caused at least five HDLI cases. Children are unlikely to experience ILD, which is often caused by smoking or occupational disease. Beyond following exposure to HDs, lung damage is a disease that children can only very rarely develop. The court blamed the causative factor on individuals, such as genetic factors, not CMIT/MIT, without any sound evidence for this determination. There have been few studies to evaluate respiratory health risks associated with exposure to CMIT and MIT. This study reviewed the scientifically sufficient evidence supporting the assertion that HDs containing CMIT/MIT cause lung injuries, including asthma, contrary to the criminal court’s judgement in terms of the strict causality required in criminal proceedings. The results can be used to better examine the association of inhalation exposure to CMIT and MIT with respiratory health effects.
Go to :
CONCLUSION
A number of humidifiers containing chemical disinfectants such as a mixture of CMIT and MIT were widely used only in South Korea, posing unreasonable inhalation exposure and accordingly causing respiratory health problems. A number of HDLI cases with clinical evidence should be prioritized in risk assessment of HD containing CMIT and MIT, even though there might be insufficient evidence in all related areas, including inhalation exposure assessment studies, animal testing, and epidemiological studies.
Go to :
 XML Download
XML Download