

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lumbar interbody fusion is used to treat many diseases of the lumbar spine, such as spinal stenosis, spondylolisthesis, and spinal deformation.1 Among the various fusion methods, posterior approaches are most commonly used, including conventional posterior lumbar interbody fusion (PLIF)234 and transforaminal lumbar interbody fusion (TLIF), first introduced by Harms et al.5
Unlike conventional PLIF, TLIF can achieve decompression and interbody arthrodesis by preserving the opposite facet and lamina in a unilateral approach, while reducing the amount of soft-tissue injury as well as the extent of thecal-sac retraction.678 Nevertheless, both muscle atrophy due to the extensive skin incisions and perivertebral muscle detachment are common postoperative problems.6910 Recently, minimally invasive techniques using a tubular retractor have been shown to preserve much of the lumbar musculature while splitting the muscle to greatly reduce intraoperative bleeding.111213 Among the advantages are a reduction in pain immediately after surgery, a faster recovery, and a shorter hospital stay and thus a faster return to daily life.14151617
Many studies have reported that minimally invasive TLIF (MI-TLIF) provides satisfactory treatment comparable to other fusion methods,12181920 with outcomes similar to those obtained with the conventional fusion method in terms of interbody fusion, complications, and clinical results. However, in MI-TLIF annulectomy and disc resection are performed on only 1 side and only a single cage is inserted, such that the area of disc space preparation may be smaller than in a conventional bilateral PLIF. Furthermore, since the laminar resection is unilateral, much less autogenous local bone can be harvested and an allograft is thus additionally required. These issues have raised concern as to whether, over the long term, the fusion rate is lower than that achieved with conventional PLIF. Nonetheless, an advantage of MI-TLIF is that it minimizes the impact on the connection between the index level and the adjacent segment by preserving the surrounding structures and the interconnecting soft tissues, especially on the contralateral side. Accordingly, compared to conventional open interbody fusion, MI-TLIF should be less likely to cause adjacent segment degeneration (ASD). However, long-term follow-up studies are lacking as most reports have a maximum follow-up of 5 years.
Here we report the clinical and radiological results obtained in a 10-year follow-up of patients with degenerative lumbar disease treated by MI-TLIF.
METHODS
Study design and patient selection
A retrospective review was conducted of patients who, between September 2005 and August 2010, underwent MI-TLIF followed by percutaneous pedicle screw fixation (PPSF) at a single institution. Adult (≥ 18 years of age) patients with a radiological and clinical follow-up of at least 10 years after MI-TLIF for spinal stenosis, spondylolisthesis, degenerative disc disease, or other degenerative lumbar diseases involving L3 to S1 were included in the study. Patients with a previous history of infection, trauma, tumor, or previous surgery on the operated or adjacent segment, diseases and drugs that affect bone metabolism, or incomplete follow-up data were excluded. Among the 107 consecutive patients who underwent MI-TLIF, 86 patients were followed for 1 year or more, 65 patients for 3 years or more, 42 patients for 5 years or more, and 30 patients for 10 years or more. The follow-up rates are 80.4%, 60.7%, 39.3%, and 28.0%, respectively, showing a gradually decreasing pattern as time goes by. In this study, 30 patients (28.0%) who had been followed-up for at least 10 years were included.
Surgical procedures
The patients were administered general anesthesia and placed in a prone position. A 22-mm longitudinal incision was then made with a disc space trajectory on the symptomatic side and a dilater was inserted continuously under fluoroscopic guidance, followed by the insertion of a tubular retractor system (METRx; Medtronic Sofamor Danek, Memphis, TN, USA). Only the facet joint on the symptomatic side was removed, using a high-speed burr with an L-shaped osteotome. After removal of the thickened yellow ligament to decompress the dural sac and nerve roots, the end plate was prepared and the patient’s local bone, collected during surgery, was implanted into the disc space. Additional allogenous bone was used as needed. The cage (either Capstone [Medtronic Sofamor Danek, Minneapolis, MN, USA], or OIC [Stryker Spine, Allendale, NJ, USA]) was filled solely with autogenous bone chips and then sealed with demineralized bone matrix (DBM, Orthoblast II; Isotis Orthobiologics, Irvine, CA, USA). The prepared cage was then placed on the more symptomatic side. Contralateral nerve decompression, when required, was performed by changing the angle of the tubular retractor and using unilateral laminotomy and bilateral decompression methods. After decompression and fusion were completed, the tubular retractor was removed and PPSF was performed. A detailed description of the procedure was provided in a previous paper.21
Measurement of radiological outcomes
Radiological parameters were evaluated based on the preoperative and 1-, 5-, and 10-year postoperative follow-up examinations. All parameters were measured using picture archiving and communication system (PACS) software and PACS workstations. Disc height and foraminal height were measured on a plain lateral radiograph together with segmental lordosis of the operated segment and lumbar lordosis.
Interbody fusion rates were assessed with the modified Bridwell interbody fusion grading system using both plain radiograph and computed tomography imaging (grade 1: fused with bony bridging, presence of trabecular remodeling; grade 2: not fully bony bridged, remodeling but without radiolucency above or below the cage; grade 3: radiolucency present at the top or bottom of the cage and screw; grade 4: fusion absent, with false motion). In this study, Bridwell grades 1 and 2 were defined as fused and Bridwell grades 3 and 4 as non-fused. Interobserver agreement of the modified Bridwell grade was assessed by 2 independent spinal surgeons. The kappa value was 0.78, indicating substantial agreement according to the Landis and Koch criteria.22
Disc degeneration of the adjacent segments was evaluated preoperatively using magnetic resonance (MR) imaging according to Pfirrmann’s classification.23 Preoperative stenosis of the spinal canal was evaluated using T2-weighted sagittal MR images according to Imagama’s classification.24
Radiological adjacent segment degeneration (R-ASDeg) was evaluated on plain X-rays, with separate assessments of the proximal and distal segments.25 R-ASDeg positivity was diagnosed based on comparisons with the preoperative radiographs and defined as a reduction in disc height by ≥ 3 mm on a neutral lateral radiograph, an increase in vertebral slip of ≥ 3 mm as seen on a neutral lateral radiograph, and an increase in the posterior opening angle of ≥ 5° as seen on a flexion lateral radiograph.
Measurement of clinical outcomes
The demographic information collected in this study included age, sex, body mass index, smoking status, osteoporosis, and disease history. Data on the patients’ surgical parameters, including the preoperative diagnosis, operation time, intraoperative blood loss, number of operated levels, operated level, and hospitalization period, were obtained from the medical records.
Clinical outcomes were assessed using the visual analog scale (VAS) for back pain and leg pain and the Oswestry disability index (ODI). All clinical variables were measured preoperatively and at 1, 5, and 10 years postoperatively. Perioperative complications, such as wound infection, postoperative neuralgia, and dural tear, were recorded, as well as the occurrence of pseudarthrosis, implant breakage, screw loosening, and cage subsidence as late complications. Reoperated adjacent segment disease (O-ASD) described those cases in which additional surgery was required to treat pain or neurological symptoms resulting from ASD.
Clinical results, including the VAS score for back pain and leg pain and the ODI, were compared between patients who underwent 1-level and 2-level surgery. The differences in clinical outcomes of young (< 60 years) vs. older (≥ 60 years) MI-TLIF-treated patients was also determined.
Statistical analysis
Clinical and radiological outcomes were analyzed using Student’s t-test and the Mann-Whitney test for continuous variables, and a χ2 test or Fisher’s exact test for categorical variables. Differences in the clinical and radiological outcomes over time as described by the continuous variables were analyzed using a repeat measures analysis of variance. A generalized estimation equation was used to compare the radiological and clinical outcomes between groups based on the presence or absence of R-ASDeg. The survival rates of R-ASDeg and O-ASD were analyzed according to follow-up period and fusion length using the Kaplan-Meier method. The survival rates of R-ASDeg and O-ASD were analyzed according to follow-up period and fusion length using the Kaplan-Meier method. The statistical analyses were conducted using SPSS software (IBM SPSS statistics for Windows, Version 25.0; IBM, Armonk, NY, USA). A P value < 0.050 was considered to indicate statistical significance.
RESULTS
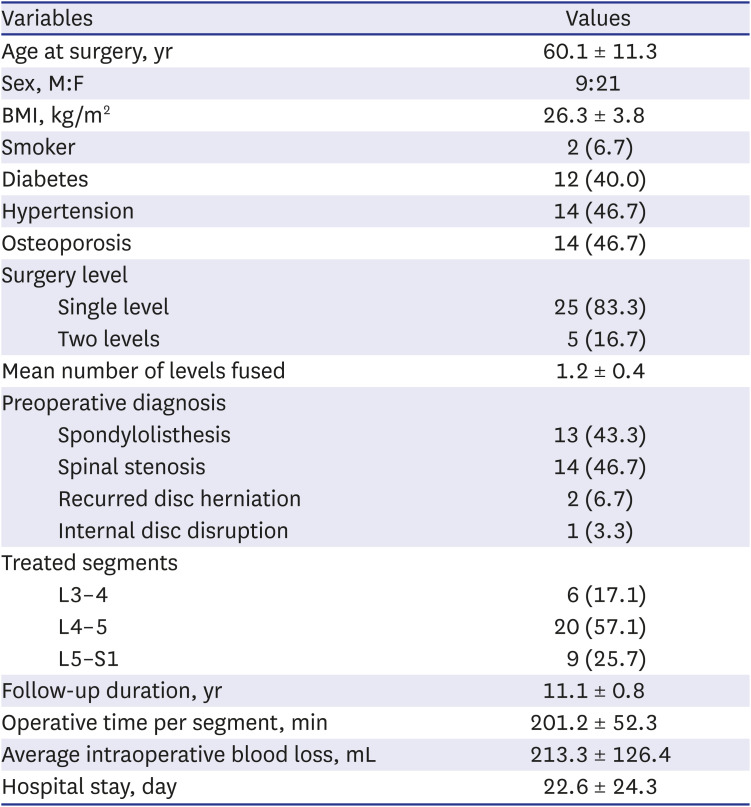
Thirty patients underwent MI-TLIF and were followed-up for at least 10 years. The mean duration of follow-up was 11.1 years (range, 10.0–12.7 years). The mean age at surgery was 60.1 ± 11.3 years (range, 40–80 years). The number of fused levels was 1 segment in 25 patients (83.3%), and 2 segments in 5 patients (16.7%). L4–5 was the most frequently operated level, followed by L5–S1 and L3–4. The main pathological indications for surgery were spinal stenosis (n = 14, 46.7%), spondylolisthesis (n = 13, 43.3%), recurrent disc herniation (n = 2, 6.7%), and internal disc disruption (n = 1, 3.3%). The baseline characteristics of the patients are listed in Table 1.
Table 1
Patient demographic and operative data
Radiological outcomes
A significant increase in foraminal height compared to the preoperative value was determined 1 year postoperatively and was maintained at the 10-year follow-up (P < 0.001). Slight increases in mean disc height, segmental lordosis, and lumbar lordosis were measured 1 year, 5 years, and 10 years postoperatively, but the difference compared to the initial value was not significant (Table 2).
Table 2
Radiologic outcomes

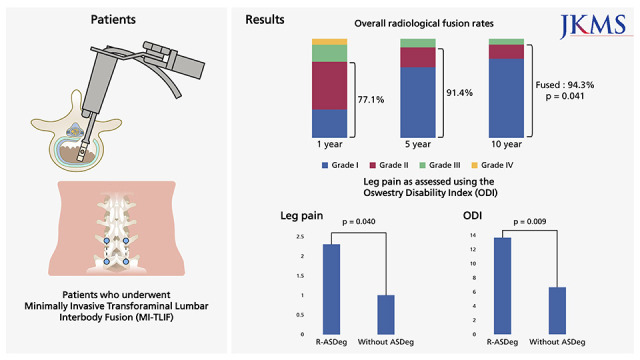
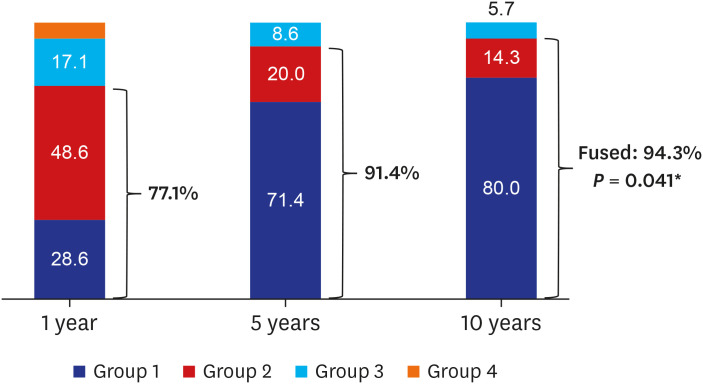
Interbody fusion was evaluated using a modified Bridwell grade and differed significantly between the 1-year and the 5-year follow-up (P < 0.001) and between the 1-year and 10-year follow-up (P < 0.001), but not between the 5-year and 10-year follow-up. The ratio of Bridwell grades 1 and 2 (fused) increased gradually, from 27 segments (77.1%) at 1 year to 32 segments (91.4%) at 5 years, and 33 segments (94.3%) at 10 years postoperatively. The difference in the fusion rate 1 and 10 years postoperatively was significant (P = 0.041) (Fig. 1). Among our patients, 2 had pseudarthrosis, which persisted until the last follow-up but remained asymptomatic and was managed conservatively.
Fig. 1
The overall radiological fusion rates, as defined by Bridwell grade 1 or 2, at the 1-, 5-, and 10-year follow-up examinations.
*P < 0.05.
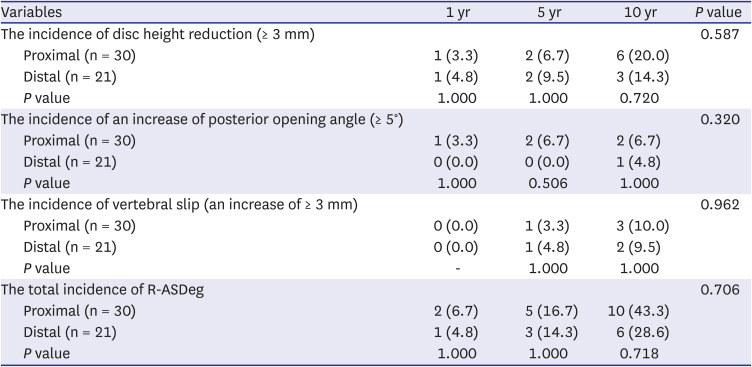
R-ASDeg occurred more frequently in the proximal than in the distal adjacent segment, but the difference was not significant. A reduction in disc height of > 3 mm, as determined at the 10-year follow-up, more often involved the proximal (6/30, 20.0%) than the distal (3/21, 14.3%) adjacent segment. The incidence of an increase of the posterior opening angle at the adjacent segment of > 5° did not significantly differ between the proximal (2/30, 6.7%) and distal (1/21, 4.8%) adjacent segments at 10 years, nor did the incidence of an increase in vertebral slip of > 3 mm (proximal adjacent segment: 3/30, 10.0%; distal adjacent segment: 2/21, 9.5%). The incidence of any of these R-ASDeg signs (disc height reduction, increased posterior opening angle, and increased vertebral slip) at the 1-year, 5-year, and 10-year follow-up was 6.7%, 16.7%, and 43.3% at the proximal adjacent segment, and 4.8%, 14.3%, and 28.6% at the distal adjacent segment, respectively. Despite a tendency of a greater frequency in the proximal than in the distal segment, the difference was not significant. A gradual increase in R-ASDeg involving either the proximal or the distal adjacent segment was determined, with rates of 10.0%, 26.7%, and 50.0% 1, 5, and 10 years postoperatively, but the differences between the corresponding values of the proximal and distal adjacent segments were not significant (Table 3).
Table 3
The R-ASDeg incidence at the proximal and distal adjacent levels
In the analysis of patients classified according to the presence or absence of R-ASDeg, in the former the VAS score for leg pain was significantly higher at the 10-year follow-up (P = 0.040), while the ODI was significantly higher both at 5 years (P = 0.002) and 10 years (P = 0.009) (Fig. 2). The 2 groups did not significantly differ with respect to back pain and other variables (Table 4).
Fig. 2
Leg pain as assessed using the ODI. The difference in leg pain between patients with and without R-ASDeg was statistically significant.
ODI = Oswestry disability index, R-ASDeg = radiological adjacent segment degeneration.
*P < 0.05; **P < 0.01.
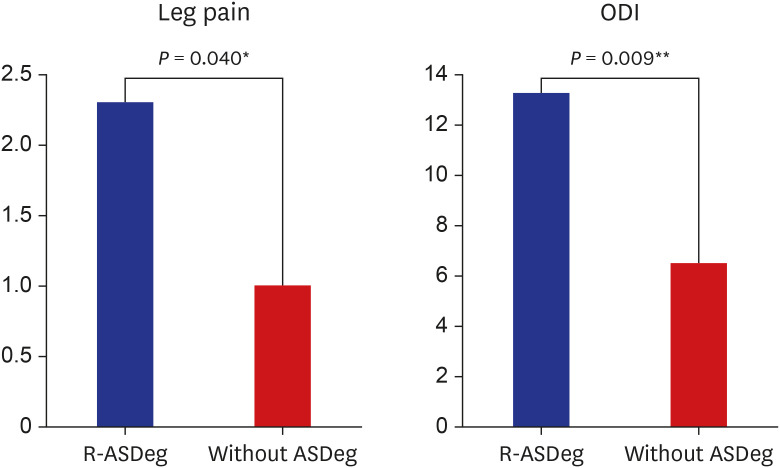
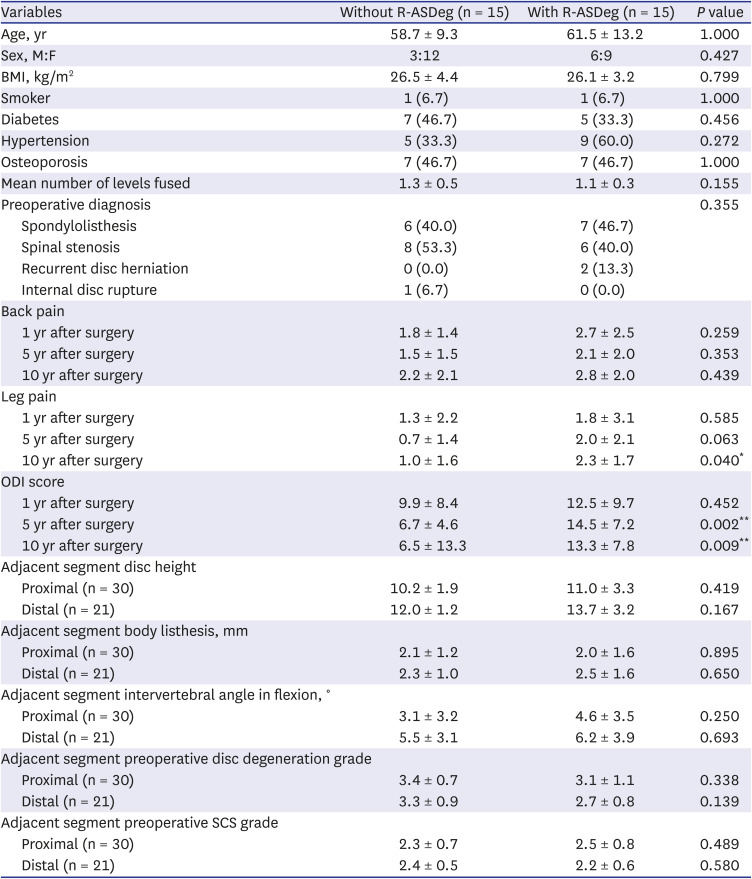
Table 4
Comparison of patients with and without R-ASDeg at 10 years after primary surgery
Clinical outcomes
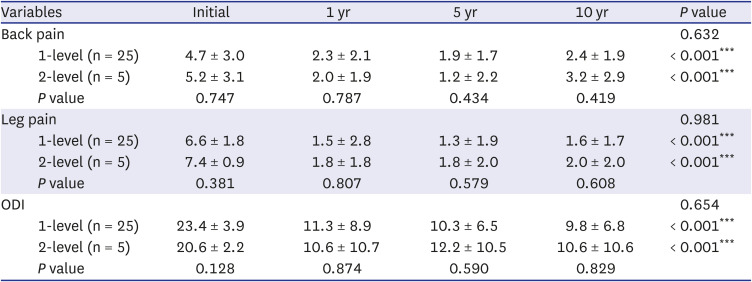
All clinical parameters improved significantly after surgery and the improvements were maintained over the 10-year follow-up period. Both the VAS score for back and leg pain and the ODI improved significantly at the 1-year, 5-year, and 10-year follow-up examinations compared to their preoperative values, without a significant difference over time (Fig. 3). The clinical scores were further analyzed by dividing patients into those with 1-level vs. 2-level surgery. The VAS score and ODI improved in each group but the changes over time were similar in the 2 groups (Table 5). MI-TLIF was as effective in patients with a 2-level pathology as in those with a 1-level pathology. There was also no difference in the clinical scores between older and young patients based on a cut-off of 60 years of age (Supplementary Table 1).
Fig. 3
The visual analog scale and ODI for LBP and leg RP as measured 1, 5, and 10 years postoperatively.
LBP = low back pain, RP = radiating pain, ODI = Oswestry disability index.
**P < 0.01; ***P < 0.001.
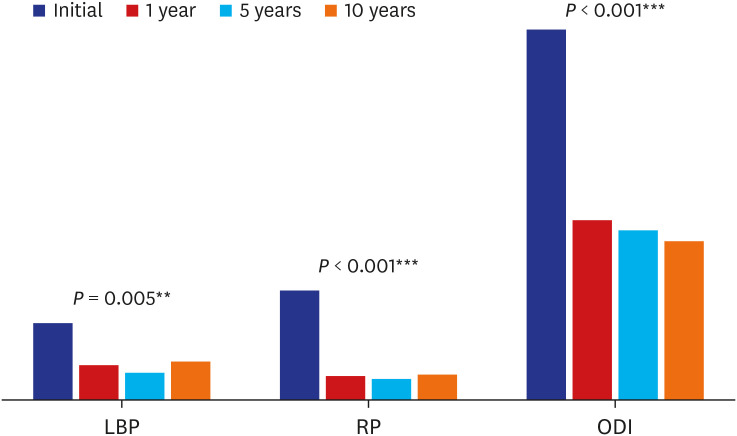
Table 5
Single vs. 2-level fusion clinical outcomes
No deaths or serious complications occurred. One patient developed a surgical site infection soon after surgery but it was successfully treated by superficial incision and drainage and resolved by 2 weeks after MI-TLIF. Two patients complained of postoperative neuralgia at the first outpatient visit, but both responded well to pregabaline. Late complications consisted of mild cage subsidence of < 25% of the disc height in 9 patients (30.0%); however, the subsidence did not cause neurological symptoms and secondary surgery was not required. As interbody fusion progressed, the subsidence ceased in all patients. A screw halo around the screw, visible on the plain anteroposterior radiograph and computed tomography images, occurred in 2 patients (6.7%), but as the union progressed the halo filled with bone and, at the last follow-up, solid interbody union was observed.
Incidence of secondary surgery
Seven of the 30 patients required reoperation, as determined at the last follow-up. The mean time from the first operation to reoperation was 7.7 years (range, 3.5–12.2). Among these patients, O-ASD involved the proximal adjacent segments in 3 patients, the distal adjacent segments in 3 patients, and both the proximal and the distal adjacent segments in 1 patient.
The pathology leading to O-ASD was spinal stenosis in 5 patients, degenerative listhesis in 1 patient, and intervertebral disc herniation in 1 patient. Reoperation consisted of open PLIF, with spinal fusion extended to adjacent segments in the 6 patients with spinal stenosis or degenerative listhesis. Microdiscectomy was performed in the patients with disc herniation. In all 7 O-ASD patients, both the neurological symptoms and pain improved after the second surgery.
Survival analysis
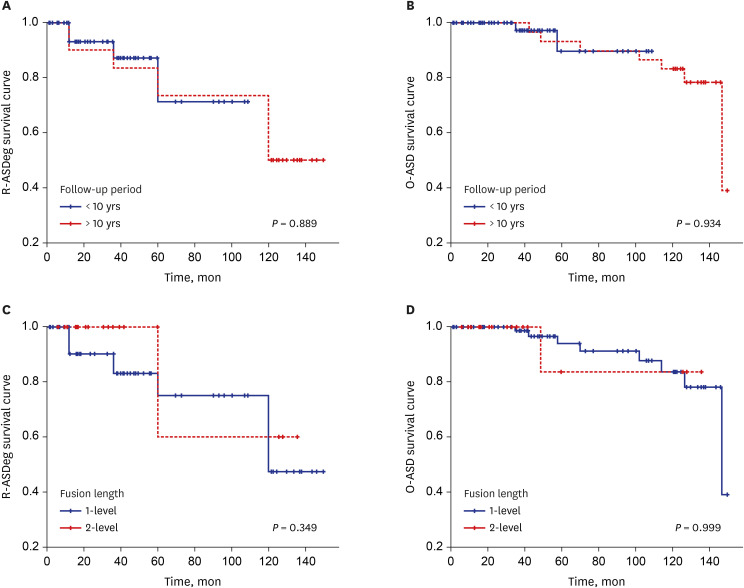
Survival analysis was performed by dividing the patients into two groups, those with less than 10 years of follow-up and those with more than 10 years of follow-up. No significant difference was observed in the R-ASDeg and O-ASD survival curves between the two groups (R-ASDeg, P = 0.889; O-ASD, P = 0.946). No significant difference was observed in the R-ASDeg and O-ASD survival curves between the two groups even when survival analysis was performed for patients who underwent 1-level fusion surgery and those who underwent 2-level fusion surgery (R-ASDeg, P = 0.349; O-ASD, P = 0.999) (Fig. 4).
DISCUSSION
As life expectancy in many countries continues to increase, due to advances in medical technology, the demand for effective spinal surgery is also likely to increase. Previously, most studies examined perioperative complications, but the focus of recent research has shifted to a consideration of the long-term results, especially long-term clinical outcomes and the inevitable occurrence of ASD following fusion surgery. The goal of minimally invasive techniques is to preserve the paraspinal muscles and soft tissues and thus maintain spinal stability between the index and adjacent segments. For this reason, MI-TLIF has been widely adopted and its results are comparable to those achieved with conventional PLIF or open TLIF. However, most of the studied patients have been followed-up for < 5 years.
In our long-term study, while the union rate 1 year after MI-TLIF was relatively low (77%), it increased to 91% at 5 years and 94% at 10 years, thus ultimately resulting in a high rate of union (Fig. 5). A limitation of MI-TLIF compared to conventional open PLIF is that the volume of local bone available as a graft is limited, because the procedure includes only a hemilaminectomy, performed through a tubular retractor. Although an allo-chip bone graft and DBM are used to compensate for this deficit, there is concern that it will lead to a low rate of union. Bone morphogenic protein (BMP) was not used in any of our patients. Nonetheless, our study was able to demonstrate the reliability of MI-TLIF as a fusion method as well as successful spinal fusion even without BMP, with results comparable to those reported in previous studies. For example, in a study that included MI-TLIF patients with a minimum 5-year follow-up, the overall fusion rate was 97.7%, with complete fusion and interbody bony bridging achieved in 84.1%.26 In another study of MI-TLIF in which patients were followed-up for 5 years,27 solid fusion was achieved in 72% of the patients by the second postoperative year and in 74% by the fifth postoperative year. Bin Abd Razak et al.28 performed 1-level MI-TLIF in patients with spondylolisthesis and reported grade 1 fusion 6 months, 2 years, and 5 years postoperatively in 39.3%, 92.9%, and 96.4%, respectively. However, in their study, in 15 patients the bone graft included additional autogenous bone from the posterior iliac crest, and in 41 patients a larger amount of DBM was used than in our study.
Fig. 5
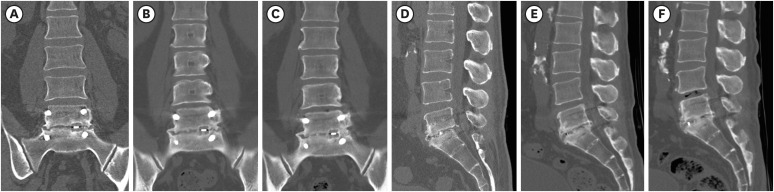
Chronological CT images of the spine. (A-C) CT after MI-TLIF of segment L5–S1. The coronal images were taken 1, 5, and 10 years after surgery. Over time, bony bridging around the cage resulted in the formation of a solid union. (D-F) CT sagittal images of segment L5–S1 taken 1, 5, and 10 years after MI-TLIF. Progressive bony bridging is seen along the cage together with callus formation in the anterior and posterior disc spaces, confirming solid union. However, 10 years postoperatively, a vacuum sign indicates disc degeneration of the proximal adjacent segment.
CT = computed tomography, MI-TLIF = minimally invasive transforaminal lumbar interbody fusion.
Several studies have described ASD after lumbar fusion surgery, but the incidence varied depending on the definition of ASD. The reported incidence of R-ASDeg is 31–82.6%293031 whereas the incidence of O-ASD is much lower, 4.9–24%.3233 The incidence of ASD also varies because it depends on the duration of follow-up. In our study, at the 10-year follow-up exam the incidence of R-ASDeg was 50% and that of O-ASD 23%. When these results are compared with those of previous studies of open PLIF, in which the patients were followed-up for at least 10 years, the incidence of R-ASDeg was lower in our study. Okuda et al.25 reported that R-ASDeg developed in 75% and O-ASD in 15% of patients with degenerative spondylolisthesis who underwent open PLIF and were followed-up for > 10 years. In a similar study, Nakashima et al.34 reported R-ASDeg in 68% and O-ASD in 9.9%. The lower incidence of O-ASD than in our study may have been due to differences in the eligibility criteria for reoperation. Further prospective studies are needed to determine whether the 2 surgical methods result in different rates of ASD.
The R-ASDeg observed in our study tended to involve the proximal adjacent segments more often than the distal adjacent segments, as also described by other investigators. In Bydon et al.,35 disc degeneration and reoperation in patients with ASD who underwent L4–5 discectomy were seen more often in the proximal than in the distal adjacent segments. Another study reported that 24 patients who underwent L4–5 fusion surgery required reoperation due to ASD of the proximal adjacent segment, L3–4, compared to 3 patients reoperated for ASD of the distal adjacent segment.36 Among our patients, L4–5 was the most frequently operated site. The distal adjacent segment, L5–S1, is supported by the tightly connected lumbosacral ligaments, which limits abnormal movement, and by the sacrum and pelvis, which increase biomechanical stability.43738
However, the implications of R-ASDeg are controversial, with at least 2 studies failing to find an association of R-ASDeg with clinical symptoms.2139 While the incidence of R-ASDeg and O-ASD differ significantly, our patients with R-ASDeg suffered statistically worse leg pain, as evaluated using the VAS and ODI. This result suggests that R-ASDeg is related to the deterioration of clinical symptoms and is a pre-stage to O-ASD progression.
Several studies have reported long-term clinical results after MI-TLIF. In the series of Bin Abd Razak et al.,28 the improvements in the VAS for back and leg pain and in the ODI, 6 months after surgery, were maintained for up to 5 years; similar results were obtained with the Short-Form 36 health survey and Neurogenic Symptoms Score. In the study of Rouben et al.,40 improvements in the ODI and in the VAS of back pain, determined 3 months postoperatively, were maintained at 49 months, regardless of the preoperative diagnosis. In our study, the clinical outcomes after MI-TLIF were maintained for a longer period of time than in previous studies; in our patients the improvements in back pain and leg pain in the first postoperative year were maintained 10 years after surgery. In other MI-TLIF studies the follow-up time was limited to 5 years, whereas our study shows that MI-TLIF continues to provide good clinical results even 10 years after the procedure.
The analyses of our MI-TLIF patients, classified according to the fusion level length, preoperative diagnosis, and age showed that, similar to other studies, these subgroups did not differ in terms of the postoperative improvements in back pain and leg pain on VAS and ODI, either after surgery or at the 10-year follow-up. Although a previous study in which patients were assessed using the VAS and ODI reported greater improvement in those with multi-level than with 1-level fusion, the preoperative VAS and ODI were higher in the 1-level group whereas the postoperative values were similar to those of the latter; thus, the trend over time was in agreement with our findings.40 In another study, patients treated with 1-level MI-TLIF were classified into isthmic spondylolisthesis and degenerative spondylolisthesis subgroups based on the preoperative diagnosis. Outcomes were evaluated using the VAS and ODI as well as patient satisfaction and return to work rates, but none of the differences between the subgroups were significant.26 These results together with those of other studies demonstrate the good long-term clinical outcomes that can be achieved with MI-TLIF, regardless of the preoperative diagnosis, patient age, or the need for 2-stage fusion.
Failure to follow-up in long-term follow-up studies can lead to misinterpretation and biased conclusions. The possibility that follow-up rates will not be the same between patients with good and bad clinical outcomes is always a difficult question to answer and a common limitation of human studies. Interestingly, in a recent study comparing the clinical outcomes of patients with and without postoperative follow-up for lumbar degenerative disease, there were no significant differences between groups.41 In this study, to minimize this limitation, the survival rate was analyzed by dividing the group with less than 10 years of follow-up and the group with more than 10 years of follow-up using the Kaplan-Meier method. When survival analysis was conducted using R-ASDeg and O-ASD as events, there was no significant difference in the survival rate between groups according to follow-up period. Therefore, although the follow-up rate of this study is not high, it is expected to provide meaningful results and will be a valuable reference for future randomized prospective studies.
A strength of our study was that it was performed at a single center and all of the operations were performed by a single senior spine surgeon (Jae Chul Lee). These features increased the reliability of the study, by reducing the number of variables. Another advantage of our study was a follow-up of > 10 years after MI-TLIF. However there were also limitations that should be addressed. These included the retrospective design, which may have resulted in observer bias, a lack of standardization of the data, and a lower quality than prospective studies, as well as the relatively small population. This resulted in a lack of statistical power in some of the analyses. Despite these weaknesses, our study is the only 1 thus far to present 10-year follow-up data for MI-TLIF. Studies of patients followed prospectively for at least 10 years will provide further insights into the clinical advantages of MI-TLIF.
In conclusion, in patients with lumbar spine disease treated by MI-TLIF, the improved clinical and radiological outcomes obtained postoperatively were maintained for up to 10 years and the fusion rates at the end of follow-up were high. However, during the first 10 postoperative years, 50% of patients developed R-ASDeg, which was also characterized by worse leg pain as assessed using the VAS and ODI tools.
 XML Download
XML Download