

 PDF
PDF Citation
Citation Print
Print


서 론
갑상선 유두암은 갑상선암 중에서 가장 흔한 조직학적 분류이며 다른 암종에 비하여 좋은 예후를 보인다.(1) 세계보건기구(World Health Organization, WHO)의 정의에 따르면 갑상선 미세유두암(Papillary thyroid microcarcinoma, PTMC)은 1 cm 이하의 갑상선 유두암으로 특히 뛰어난 예후를 보이는 것으로 알려져 있다.(2-4)
갑상선 유두암의 치료로는 일측엽수술(Lobectomy), 전절제술(Total thyroidectomy) 및 방사성 요오드 치료까지 다양한 방법이 있으며, 최근에는 수술을 하지 않고 지켜보는 적극적 감시(Active surveillance)도 일부 적용되고 있다.(5-8) 2015년 개정된 미국갑상선학회(American Thyroid Association, ATA) 권고안에 따르면 갑상선 미세유두암이 단일엽에만 존재하고 실질 내에 국한되어 있으면서 림프절 전이가 없는 경우 일측엽절제술을 시행할 수 있다.(9,10) 그러나 상기 조건에 해당하지 않는 경우에는 갑상선 전절제를 고려해야 한다. 따라서 수술 전 초음파를 비롯한 영상의학적 검사를 통해 갑상선과 경부 림프절을 세심하게 평가하는 것이 수술 계획을 세우는 데 필수적이라 할 수 있다.
갑상선 초음파(Ultrasound)는 갑상선암으로 진단된 환자에서 갑상선의 병변 또는 상태를 확인하기에 가장 쉽고 빠른 영상검사로, 미국갑상선학회(ATA)나 NCCN 등의 단체에서 발행한 진단 및 치료권고안에도 초음파 검사가 포함된다.(11-13)
저자들은 갑상선 미세유두암에서 종양의 크기, 중심부 또는 측경부 림프절 전이 여부, 갑상선 피막외 침범, 다발성 병변, 양측성 등의 특성을 지표로 하여 초음파를 이용한 병기 설정의 정확도를 조사해보고자 하였다.
Go to : 
방 법
2016년 6월부터 2020년 6월까지 칠곡경북대학교병원에서 갑상선 미세유두암으로 수술을 받은 환자 159명을 대상으로 후향적 연구를 진행하였다. 수술 방법으로는 갑상선 일측엽 절제술 또는 갑상선 전절제술이 시행되었고, 수술 전 초음파 검사 결과에 따라 병변의 동측 또는 양측 중앙 경부림프절 절제술을 같이 시행하였다. 수술 전 초음파 및 미세침흡인생검(Fine needle aspiration cytology, FNAC)으로 측경부의 림프절 전이가 확진된 일부 환자는 측경부 림프절 곽청술을 함께 받았다. 갑상선 유두암이 아닌 다른 진단으로 수술을 한 경우나 수술 후 1 cm 이상인 갑상선 유두암은 연구 대상에서 제외하였다.
연구 대상자의 병력 기록을 바탕으로 나이, 성별, 갑상선의 기저질환, 갑상선암의 위치와 수술방법, 수술 전/후의 진단에 대한 자료를 수집 및 평가하였다. 수술 전 병기설정 초음파 소견과 수술 후 병리학적 소견으로부터 갑상선 미세유두암의 크기, 양측성 및 다발성, 갑상선 전방 또는 후방으로의 피막외 침범, 중앙부 및 측경부 림프절 전이에 대해 비교 분석하였다. 양측성 갑상선 미세유두암은 미세유두암이 양측엽 모두에 각각 존재하는 경우로 정의하였고, 다발성 갑상선 미세유두암은 위치와 무관하게 종양의 개수가 2개 이상인 경우로 정의하였다. 수술 전 초음파 소견과 수술 후 병리학적 소견을 바탕으로 계산된 민감도, 특이도, 양성예측도, 음성예측도, 위양성률, 위음성률을 지표로 하여 갑상선 미세유두암의 병기 설정에 있어 초음파 검사의 정확도를 평가하였다.
Go to :
결 과
총 159명의 갑상선 미세유두암 환자의 평균 연령은 46.4세(SD, ±10.9)였으며, 이들 중 45세 이상인 환자는 86명(54.1%)이었다. 환자들의 성별은 남성 26명(16.4%), 여성 133명(83.6%)으로 여성이 훨씬 많았다. 갑상선암으로 진단되기 전 갑상선의 기저질환으로 하시모토 갑상선염이 있는 환자가 1명(0.6%) 있었고, 그레이브스병을 진단받은 환자는 없었다. 갑상선암은 우측과 좌측이 동일하게 79례(49.7%)로 확인되었고, 상중하로 구분하였을 때는 중부의 병변이 86례(54.7%)로 가장 많았다. 수술적 방법으로는 일측엽 절제술(126례, 79.2%)이 가장 많이 시행되었으며, 그 외 전절제술 30례(18.9%), 갑상선 협부절제술(Isthmectomy) 1례(0.6%) 및 측경부 림프절 곽청술(Modified radical neck dissection, MRND) 2례(1.3%)가 시행되었다(Table 1).
Table 1
Clinical Characteristics of Patients with Papillary Thyroid Microcarcinoma
| Variables | Total (n = 159) | |
|---|---|---|
| Mean age (years, ±SD) | 46.4 ± 10.9 | |
| Age at diagnosis (n, %) | <45 | 73 (45.9) |
| ≥45 | 86 (54.1) | |
| Sex (n, %) | Male | 26 (16.4) |
| Female | 133 (83.6) | |
| Underlying thyroid disease (n, %) | Hashimoto’s thyroiditis | 1 (0.6) |
| Graves’ disease | 0 | |
| Location* (n, %) | Right | 79 (49.7) |
| Left | 79 (49.7) | |
| Isthmus | 1 (0.6) | |
| Superior | 39 (24.5) | |
| Middle | 86 (54.7) | |
| Inferior | 33 (20.8) | |
| Type of surgery (n, %) | Lobectomy | 126 (79.2) |
| Total thyroidectomy | 30 (18.9) | |
| Total thyroidectomy with modified radical neck dissection | 2 (1.3) | |
| Isthmectomy | 1 (0.6) |
![]()
종양의 평균 크기는 수술 전 초음파 상 0.7 cm (SD, ±0.3), 최종 병리조직검사결과 상 0.6 cm (SD, ±0.3)로 비슷하였으며, 양측성 갑상선암은 수술 전 초음파 검사에서 22례(13.8%)로 예상되었으나 수술 후 7례가 추가로 진단되어 총 29례(18.2%)로 최종 확인되었다. 다발성 병소는 수술 전 초음파와 수술 후 조직검사 결과에서 각각 27례(17.0%), 35례(22.0%)로 확인되었으며, 갑상선 피막외 침범은 각각 36례(22.6%), 19례(11.9%)에서 확인되었다. 중앙경부 림프절 전이는 수술 전 초음파에서보다 수술 후 병리결과에서 훨씬 높은 빈도로 확인되었고(11.3% vs 30.2%), 측경부 림프절 전이는 수술 전 초음파에서 5례(3.1%)가 예상되었으나 조직검사 결과 전이가 확인된 2례(1.3%)에서만 측경부 림프절 곽청술을 시행하였다. 전이성 림프절의 개수와 최대 전이병변의 장경은 수술 전 초음파에서 파악이 불가하여 비교하지 못하였다(Table 2).
Table 2
Ultrasonographic and Pathologic Findings of Papillary Thyroid Microcarcinoma
![]()
수술 전 초음파로 갑상선 미세유두암의 특징을 파악할 때, 측경부 림프절 전이를 예측하는 것은 민감도 100.0%, 특이도 98.1%, 위양성율 40.0%, 위음성율 0%, 정확도 98.1%로 다른 인자에 비해 비교적 높은 정확도를 보이는 반면, 중앙경부 림프절 전이를 예측하는 것은 가장 낮은 정확도를 보였다(민감도 14.6%, 특이도 90.1%, 위양성율 6.9%, 위음성율 25.8%, 정확도 67.3%). 전방 및 후방 피막외 침범, 다발성 암 여부에 대해서는 정확도 80% 이상의 높은 예측율이 확인되었다(Table 3).
Table 3
Statistical Parameters between Ultrasonographic and Pathologic Findings of Papillary Thyroid Microcarcinoma
![]()
Go to :
고 찰
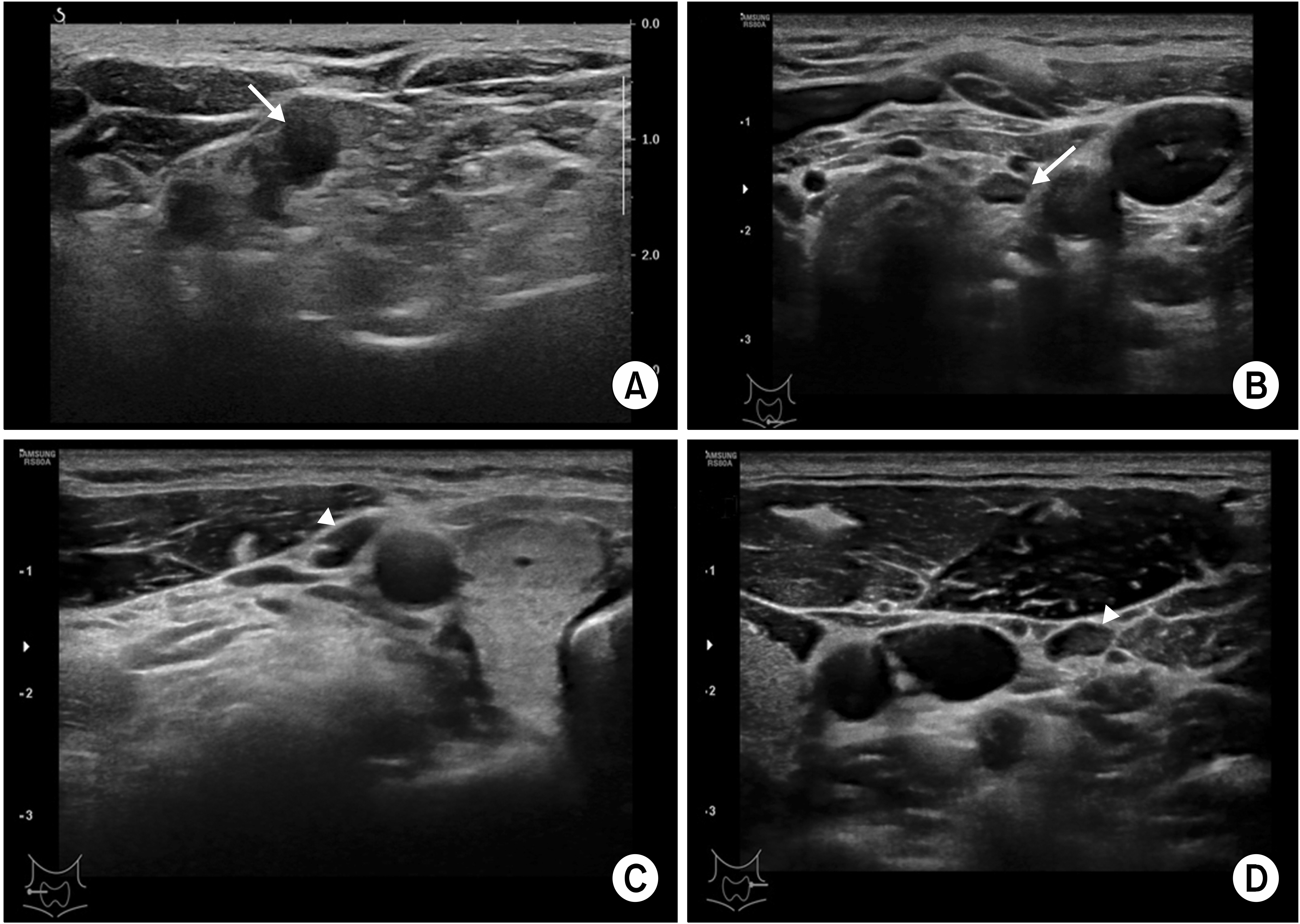
세계보건기구(WHO)의 정의에 따르면 갑상선 미세유두암은 종양의 크기가 1 cm 이하인 갑상선 유두암을 말한다. 크기가 작기 때문에 대부분 갑상선 실질 내에 위치하며, 중앙경부 또는 측경부 림프절 전이를 보이는 경우가 드물어 예후가 뛰어난 것으로 보고된 바 있다.(2-4) 그러나 갑상선 미세유두암이 다발성이거나 피막외 침범이 동반되어 있는 경우(Fig. 1), 중앙경부 또는 측경부 림프절 전이가 의심되는 경우에는 갑상선 전절제술을 고려하여야 한다(Fig. 2).
 | Fig. 1Various ultrasonographic findings of thyroid papillary microcarcinoma (PTMC). Extrathyroidal extension to anterior aspect (arrow head) (A) or to posterior aspect (arrow heads) (B), abutting status to trachea of PTMC can be detected in preoperative ultrasound. Multifocal (D) or bilateral (E) PTMCs can be also identified in ultrasound.
|
크기가 작은 갑상선암은 적극적 감시만으로도 충분하다는 주장도 있지만, 적극적 감시를 시행한 갑상선 암의 7-20%에서 최종적으로 종양의 크기가 증가하는 것으로 보고되고 있어 많은 환자들이 여전히 수술을 우선적으로 고려한다.(2,14) 최근에는 예후가 매우 좋을 것으로 예상되는 환자에 한하여 선별적으로 적극적 감시를 적용한다.(15) 수술적 치료는 크게 갑상선 일측엽 절제술과 갑상선 전절제술로 나뉘는데, 갑상선 전절제술을 받은 환자는 평생 약을 복용해야 하는 불편함을 감수해야할 뿐 아니라 일측엽 절제술에 비하여 갑상선 주변 신경 및 근육손상 등의 합병증 발생 위험이 더 높다. 따라서 갑상선 전절제술을 시행할 환자를 선별하는 것은 매우 중요하며, 이들을 선별함에 있어 수술 전 갑상선 초음파 검사는 많은 정보를 제공한다.
초음파는 다양한 암종의 진단 및 치료에 필수적인 영상기법으로, 갑상선암에서는 특히 갑상선 결절의 크기나 모양, 위치 등을 파악하고 피막외 침범 및 중앙경부/측경부 림프절 전이를 평가하기 위해 시행된다.(16-21) 또한 적극적 감시를 하는 환자에서는 주기적인 초음파 검사를 통하여 종양의 변화를 평가할 수 있다.(15,22-24) 갑상선암에 있어 수술 전 초음파 검사는 병기를 예상하고 수술 계획을 세우는 데 많은 정보를 제공하지만 초음파 소견과 수술 후 병리 결과의 일치 여부는 인자에 따라 차이가 있는 것으로 보고되고 있다.
갑상선 미세유두암을 대상으로 한 본 연구에서 수술 전 초음파 검사결과 중 측경부 림프절 전이는 수술 후 병리결과와 높은 확률로 일치하였으나(정확도 98.1%), 중앙경부 림프절 전이는 정확도 67.3%로 가장 낮았다. 즉, 수술 전 초음파로 측경부 림프절 전이는 보다 정확하게 예측할 수 있으나, 중앙경부 림프절 전이를 예측하는 것은 정확하지 않을 수 있다. 이는 중앙경부 림프절 전이의 크기가 평균 0.3 cm로 작고 쇄골 사이에 주로 위치하여 초음파로 검사 가능한 범위를 벗어나는 등의 제한점 때문이라고 생각된다. 피막외 침범은 전방과 후방에서 비슷한 정확도로 예측할 수 있었는데, 양방향 모두 정확도 85% 이상으로 수술 전 초음파소견과 수술 후 병리소견이 일치하였다.
갑상선은 초음파 진단이 매우 유용하게 적용될 수 있는 장기 중 하나로, 갑상선암이나 갑상선암의 전이성 림프절은 초음파 소견으로 쉽게 구별이 가능하다. 갑상선 결절은 비교적 세로로 길쭉하게 생겼거나(taller than wide shape) 변연부가 불규칙한 저에코성 결절의 소견을 보일 때 암으로 의심한다. 초음파 검사는 병변의 악성 가능성을 포함하여 갑상선암의 피막침범, 기관지 침범 또는 주변 혈관이나 신경과의 유착 여부 등을 어느 정도 예측할 수 있어 수술 전 계획을 세우는데 유용하다. 경부 림프절은 초음파 소견 상 크기가 크고 피막이 두꺼워져 있거나 림프절 문(fatty hilum)의 소실이 있다면 전이가 있을 것으로 예측할 수 있다. 그러나 본 연구에서는 쇄골 중앙부(level VI)에 위치하는 림프절은 가측 림프절에 비해 예측도가 떨어지는 것이 확인되었다.
저자들의 연구에서 갑상선암 진단 전 하시모토 갑상선염을 진단받은 환자가 1명 포함되었는데, 해당 환자의 경우 갑상선암이 진단된 시점에서는 초음파 상 전형적인 하시모토 갑상선염의 소견을 보이고 있지 않아 갑상선암의 진단에 큰 어려움은 없었다.
종합적으로 볼 때 갑상선 초음파 검사는 갑상선 미세유두암의 진단과 치료에 필수적인 도구로서 수술 전 시행하여 전방 또는 후방 피막외 침범, 다발성 또는 양측성 갑상선암의 여부, 측경부 림프절 전이 등의 정보를 비교적 정확하게 예측할 수 있으나, 중앙경부 림프절 전이를 예측하기에는 정확도가 떨어지는 것으로 보인다. 따라서 중앙경부 림프절 전이에 대해서는 초음파 소견을 전적으로 신뢰하기 보다는 수술장에서 육안적으로 전이가 의심되거나 수술 중 동결절편검사를 시행하여 전이가 확인되는 경우에 한하여 추가적인 수술 여부를 결정하는 것이 바람직하겠다.
Go to :
 XML Download
XML Download