

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Axillary staging in breast cancer is an important prognostic factor, and the standard evaluation for axillary lymph nodes would require full dissection.(1,2) However, axillary lymph node dissection (ALND) causes various sequelae, including numbness, pain, impaired arm movement, and lymphedema.(3,4) Although sentinel lymph node biopsy (SLNB) could be an alternative procedure for evaluating axillary lymph nodes in breast cancer, particularly for early breast cancer or clinically node-negative breast cancer,(5,6) it also presents with a possibility of such morbidities, albeit with a lower incidence rate. Therefore, several clinical trials on the omission of axillary staging in early breast cancer have been conducted.(7,8)
The pathologic assessment of axillary lymph nodes is usually performed with fine needle aspiration cytology (FNAC) or core needle biopsy (CNB).(9-11) Although the false-negative rate of FNAC for axillary lymph nodes in breast cancer is reported to be relatively high at 10%–31%,(12-14) FNAC is more frequently used than CNB for axillary evaluation due to its lower incidence of procedural complications. However, FNAC cannot replace the surgical assessment of axillary lymph nodes. Moreover, CNB for evaluating axillary lymph nodes has shown high accuracy and low false-negative rates.(10,11,15)
The aim of this study is to compare the accuracy and false-negative rates between FNAC and CNB for evaluating axillary lymph nodes in patients with breast cancer who did and did not receive neoadjuvant chemotherapy.
Go to : 
METHODS
Between 2011 and 2016, 159 patients with cN1 breast cancer underwent surgery and additional treatments at the Kyungpook National University Hospital. Among them, 74 patients who underwent a pathologic evaluation for suspicious axillary lymph nodes before surgery were included in this study. This pathologic evaluation was performed using FNAC or CNB. We excluded 24 cases which showed conversion to radiologic complete response (rCR) after neoadjuvant chemotherapy. Furthermore, the FNAC and CNB groups were compared based on various clinicopathologic factors in this study.
Clinical records and pathologic results were all reviewed and analyzed retrospectively. Moreover, the clinicopathologic variables included patient age at breast cancer diagnosis, body mass index, clinical and pathologic tumor size, clinical lymph node status, neoadjuvant or adjuvant treatment performance, and oncologic outcomes. If the patients received neoadjuvant chemotherapy (NAC) before surgery, the rCR for breast lesions and axillary lymph nodes was also evaluated using mammography, ultrasonography, breast magnetic resonance imaging (MRI), and chest/abdominal computed tomography (CT).
The breast cancers were classified into four different molecular subtypes based on their immunohistochemistry (IHC) biomarkers: estrogen receptor, progesterone receptor (PR), HER2 gene status, and the Ki67 index. The Ki67 proliferation index was considered high when >15% of tumor cells showed nuclear immunoreactivity. The histopathological examination of the four biomarkers was performed in accordance with the criteria in the ASCO/CAP (American Society of Clinical Oncology/College of American Pathologists) 2016 guidelines.
The FNAC procedures were performed under ultrasonography guidance; each lesion was aspirated with a 21-gauge needle using the to-and-fro method. Each aspirated material was smeared on the glass slides and was immediately fixed in 95% alcohol. All FNAC slides were prepared for Papanicolaou staining in accordance with the standard method. Moreover, the CNB procedures were performed under ultrasonography guidance using 18-gauge cutting needle biopsy instruments (StericutⓇ, TSK Laboratory, Hirayanagi-Cho, Japan). At least two core samples including cortical tissue were obtained from suspicious axillary lymph nodes. The CNB samples were immediately fixed with 10% neutral buffered formalin and then paraffin-embedded. The CNB specimens were prepared and stained with hematoxylin and eosin. Moreover, the diagnosis of FNAC and CNB was confirmed by a cytopathologist with comparable experience.
All procedures in this study that involved human participants were performed in accordance with the ethical standards of the institutional review board of Kyungpook National Hospital, and the experimental protocol was also approved by them (KNUCH 2015-05-205). Furthermore, all the experiments were performed in accordance with the relevant guidelines and regulations.
1. Surgical methods
All patients underwent SLNB or ALND depending on the condition of the axillary lymph nodes. To identify the sentinel lymph node radiolabeled colloid, blue dye, or a combination of these methods was used. A gamma probe identified radioactivity in the lymph nodes in the axilla, and the surgeons visually identified the blue-stained lymphatic nodes. Moreover, the axilla was meticulously examined and any palpable or visually abnormal lymph nodes were resected and submitted for frozen biopsy. Conventional ALND included the removal of level I and II axillary lymph nodes.
2. Statistical analysis
To assess the impact of the CNB procedure for suspicious axillary lymph nodes, the sensitivity, specificity, positive and negative predictive values, false-positive and false-negative rates, and accuracy rates of FNAC and CNB were calculated and compared. The detection rates of suspicious axillary lymph nodes in ultrasound, chest CT, and breast MRI were also evaluated.
All statistical analyses were performed using SPSS ver. 25.0 (SPSS, Chicago, IL, USA). Categorical variables were analyzed using the chi-squared test through univariate analysis. A P-value < 0.05 was considered as statistically significant.
Go to :
RESULTS
No statistically significant differences were observed between the patients who received FNAC (n = 27) and CNB (n = 23) with regard to the mean age and body mass index, type of breast, and axillary surgery, mean clinical and pathologic tumor size, and molecular biomarkers. During the mean follow-up period of 55.2 months (47.3 ± 16.8 in FNAC vs. 58.2 ± 78.4 in CNB), five cases of locoregional recurrence (2 in FNAC vs. 3 in CNB, P = 0.518), two cases of distant metastasis (0 in FNAC vs. 2 in CNB, P = 0.123), and one case of death in the FNAC group were observed. Moreover, after the procedure, only one case of hematoma was detected in the CNB group (P = 0.941; Table 1).
Table 1
Clinicopathologic Factors of Patients with Breast Cancer Who Were Evaluated for Suspicious Axillary Lymph Nodes Using Fine Needle Aspiration Cytology and Core Needle Biopsy
![]()
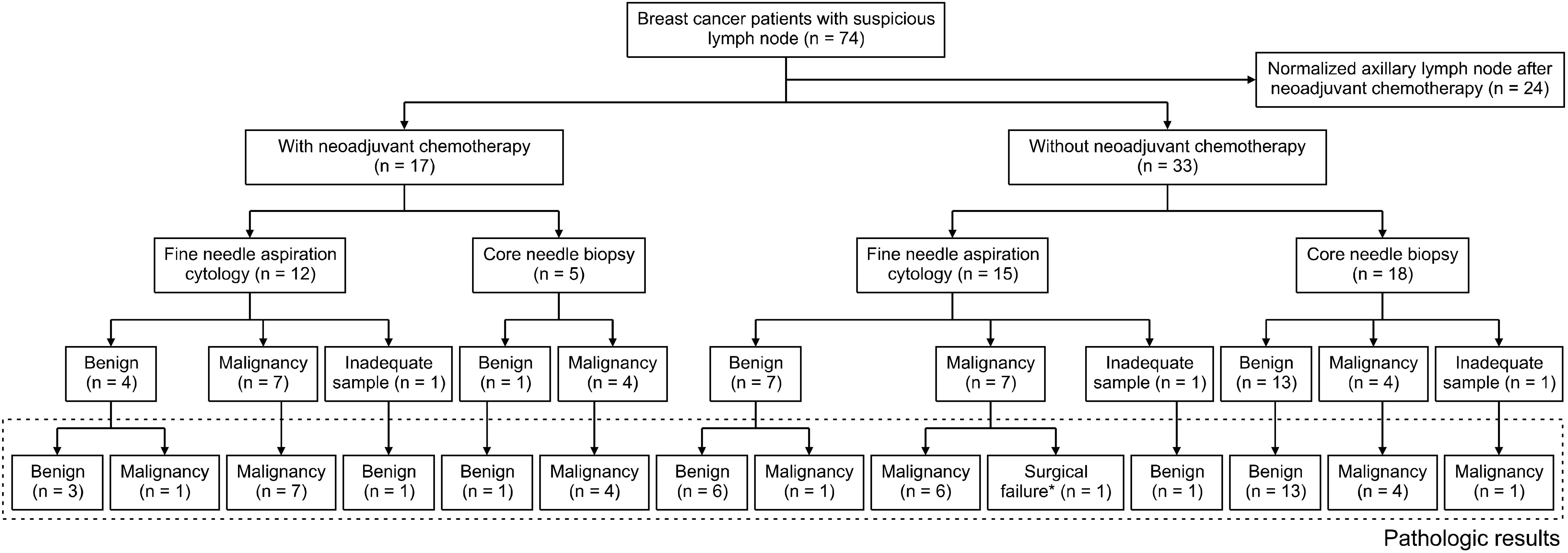
In 17 patients who underwent neoadjuvant chemotherapy (NAC), the FNAC and CNB procedures were performed in 12 and 5 cases, respectively. Moreover, in 33 patients who did not receive NAC, the FNAC, and CNB procedures were performed in 15 and 18 cases, respectively, to evaluate the suspected metastasis to axillary lymph nodes, respectively. Four cases of technical failure were observed, including procedural failure and surgical failure. Two cases in FNAC showed cell counts that were too small to assess the metastasis of breast cancer, and one case in CNB showed only fibrofatty tissue in cores. In one case of surgical failure, ALND had to be performed due to the undetectable malignancy in the lymph nodes or sentinel lymph nodes. Therefore, the accurate pathologic findings of the malignancy-proven lymph nodes could not be recognized (Fig. 1).
Regardless of performing NAC, CNB for the evaluation of metastatic axillary lymph node showed better results than FNAC in terms of sensitivity, specificity, negative predictive value, false-negative rates, and accuracy. In the FNAC group, the false-negative rate was higher in patients with breast cancer who received NAC before lymph node evaluation (Table 2).
Table 2
Statistical Quality Criteria of Fine-Needle Aspiration Cytology and Core Needle Biopsy for Evaluation of Suspicious Axillary Lymph Node*
![]()
Among the imaging modalities, including axillary ultrasound, chest CT, and breast MRI, the axillary ultrasound showed superior detection rates compared to chest CT and breast MRI in both non-malignant and malignant lymph node groups (Table 3).
Table 3
Detection Rate in Ultrasound, Chest CT, and Breast MRI of Suspicious Axillary Lymph Nodes Based on Pathologic Results*
![]()
Go to :
DISCUSSION
Over the past decades, the cases of breast cancer requiring surgical treatment have declined. In breast cancer surgery, the development of radiotherapy as an adjuvant treatment has enabled breast conservation, and it has been reported that nipple-sparing mastectomy is not inferior to conventional mastectomy.(16-20)
Even the need for axillary surgery has declined. The concept of SLNB, which is still considered a revolutionary surgical concept, could be applied for axillary staging instead of ALND, which has been reported to greatly reduce postoperative morbidities, such as postoperative seroma, numbness, axillary pain, limitation of arm movement, and lymphedema.(3-5) In 2014 and 2018, the EORTC (European Organisation for Research and Treatment of Cancer) has reported that axillary radiotherapy is not inferior to ALND in the treatment of metastatic axillary lymph nodes in breast cancer (AMAROS study), even after undergoing NAC.(21,22) During the similar period, the US Alliance Group had reported the possibility of the use of SLNB for selected patients who received NAC based on the results of a 10-year long-term follow-up indicating that SLNB was not inferior to ALND in patients with less than three metastatic axillary lymph nodes after NAC.(23,24)
Recently, the EIO (European Institute of Oncology) had initiated the SOUND (Sentinel node vs. Observation after axillary Ultra-souND) trial which was designed to compare SLNB with only surveillance with axillary ultrasound in node-negative early breast cancer.(7) Moreover, the most important evidence that supports the omission of axillary staging is that removing the axillary lymph nodes does not seem to have a direct impact on the actual overall survival. However, to skip axillary surgery, an alternative procedure should be used for axillary staging to predict the prognosis of breast cancer. Although axillary ultrasound may be sufficient to replace SLNB, even if the result of the SOUND trial has not been officially reported yet, an alternative method of tissue confirmation is necessary to omit surgical evaluation in advanced breast cancer and NAC-treated breast cancer cases.
Generally, the pathologic assessment for axillary lymph nodes is performed with FNAC or CNB.(9-11) Because FNAC is easier and less invasive, it is more frequently performed than CNB. However, because its false-negative rate can be as high as 58%, surgical evaluation is necessary.(12) Conversely, the false-negative rate of CNB is much lower at 0%–14%. The ultrasound-guided CNB in particular shows better results compared to ultrasound-guided FNA in evaluating axillary lymph nodes in breast cancer after NAC. (12,15,25-27)
Metastasis to axillary lymph nodes is easily detected using various imaging modalities. The accuracy of ultrasound in detecting axillary lymph node metastasis in breast cancer is reportedly 67%–96%, and the results further improve greatly if the breast cancer was previously treated with NAC.(28,29) The sensitivity and specificity of breast MRI for evaluating axillary lymph nodes in breast cancer are reportedly 33.3%–97.0% and 14.0%–98.5%, respectively. (29-32) In the present study, although the suspicious axillary lymph node was the most frequently detected with ultrasound imaging, the false-positive rate was also the highest with ultrasound imaging. Therefore, pathologic confirmation is necessary to evaluate metastasis to axillary lymph nodes in breast cancer. Improved results in the identification of metastatic axillary lymph node may provide the evidence supporting the omission of axillary surgical staging.
Moreover, because the lesions showing locoregional recurrence or distant metastasis may not be biologically equivalent to primary tumor, tissue biopsy is necessary for not only an accurate diagnosis of the lesion but also the assessment of biologic features. When the recurrence is only detected in axillary lymph nodes because only the existence of malignant cells can be detected with FNAC, CNB is necessary to provide biologic information in order to develop a treatment strategy.
Although several studies have reported a significantly higher occurrence of post-procedural complications, such as hematoma or bruising, in CNB compared to FNA, (10,26,33-35) most complications can be managed with only conservative treatment. In a recent study, only one case presented with hematoma after CNB, and this complication was resolved spontaneously within a week.
Although this retrospective study did not have a large population of breast cancer patients and did not involve any randomization of procedures, we believe that the efficacy of CNB in the assessment of axillary lymph nodes has been sufficiently evaluated.
Go to :
CONCLUSION
Overall, CNB is more effective than FNAC in evaluating axillary lymph nodes in breast cancer and can be performed without major complications. Because the tissue biopsy can provide information on not only the diagnosis of lesion but also its biologic features, ultrasound-guided CNB for axillary lymph nodes can be useful in examining lymph nodes with metastasis recurrence as well in cases wherein SLNB has to be omitted.
Go to :
 XML Download
XML Download