

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sexual health has major implications for quality of life in adults.1) Although its impact on personal well-being is well accepted, it continues to be underrated and under addressed in clinical cardiology practice.2)
As an increasing number of children with congenital heart disease survives childhood and life expectancy of adult patients with congenital heart disease (ACHD) generally increases,3) the focus of medical attention is shifting towards factors with impact on quality of life. As such, sexual health becomes increasingly important in this specific patient cohort. Previous studies have reported a prevalence of erectile dysfunction (ED) between 10 and 28%4)5)6) in ACHD. Given the young average ACHD age, the prevalence of ED in ACHD appears considerable compared to generally much older groups included in non-congenital analyses reporting an ED prevalence between 13–71%.7)
In the general population, causes for ED are multifactorial involving organic, psychological and social factors.7) Considering the specific characteristics of ACHD, influencing variables may differ, however, from non-ACHD. These include cardiac and extracardiac morbidities, endothelial dysfunction, exercise limitation as well as perceived or actual risk of malignant cardiac arrhythmias during exertion.6)8)9)
Congenital heart disease is a chronic illness that requires regular follow-up visits ideally in centers of specialized care.10)11) Theoretically, this should offer the opportunity of building a trusting patient-physician relationship enabling physicians to address more sensitive topics such as ED. However, data on non-ACHD suggests, that ED is often under addressed by health professionals.2)12)
In our analysis, we aimed to quantify the magnitude of ED in ACHD. We compared ACHD with ED to patients without ED based on questionnaire responses. We focused specifically on the frequency of sexual activity, satisfaction with sexual life and the role of patient-physician communication.
METHODS
Ethical statement
NRCHD specific data-protection concept is registered with the Berlin Official for Data Protection and Freedom of Information (Nr. 531.390). General approval of the Ethical Review Board of the Charité – Universitätsmedizin Berlin is given for all research conducted within the scope of the NRCHD. It was conducted in accordance with the Declaration of Helsinki in the current revised version by the General Assembly 2013.
Methods
The dataset of the German National Register for Congenital Heart Defects (NRCHD) has been described in detail previously.13) In a subgroup of patients, electronic contact information is available, and patients have consented to being contacted for questionnaire type studies. Based on this dataset, male patients over the age of 18 years were invited per electronic mail to participate in the online survey about sexual health. The medical information provided was cross-referenced for complexity of disease. Patient received individualized URL-links for survey participation based on complexity of the underlying heart defect as coded in the Register. A flowchart stratifying overall male patients older than 18 years, those with mailing contacts available and those that responded by age and complexity of disease is provided in Supplementary Figure 1. The complete questionnaire with the number of answers given is displayed in Supplementary Table 1.
In addition to demographic and disease specific information, the questionnaire included the previously validated and clinically well-implemented International Index of Erectile Function (IIEF) Score to identify male individuals with ED.14) This score evaluates erectile function, orgasmic function, intercourse satisfaction and overall satisfaction. A cutoff value of 22 points, indicating a more than mild ED was chosen to distinguish between ED and of non-ED individuals.15) Distinguishing questions between ED and non-ED patients are marked with shading in Supplementary Table 1. Severity of the underlying congenital heart disease was graded as mild, moderate or highly complex according to the 32nd Bethesda conference classification.16) Among the analyzed patients, a total of 7 patients underwent heart transplantation but have been included in the analysis because of former congenital heart disease.
Statistical analysis
Standard methods of descriptive statistics were used. Categorical variables are summarized as percentages. Comparisons between groups were performed using χ2 test and Fisher's exact test. Results of χ2 test are given throughout. The prevalence of ED in the underlying population enrolled in the National Register was estimated by adjusting for the distribution of disease complexity and age compared to the surveyed group. Parameters potentially associated with ED were evaluated on univariable logistic regression analysis. Candidate variables with significant association to ED on univariable analysis as well as parameters associated with ED according to current literature were subsequently included into multivariable stepwise logistic regression analyses using threshold of p value of 0.20. All analyses were explorative, and results of the analyses are summarized as odds ratio (OR) with their 95% confidence intervals and p values. The p values below 0.05 were regarded as statistically significant. Statistical analyses were performed using MedCalc 10.1.2.0 (MedCalc Software, Mariakerke, Belgium).
RESULTS
More than 50,000 patients of any age with the diagnosis of a congenital heart disease are registered in the NRCHD database (of those, 10,738 men ≥18 years). The 2,234 male patients ≥18 years, that had previously agreed to be contacted by electronic mail for surveys, were contacted to participate (for details on the cohorts see Supplementary Figure 1). In total, 371 male ACHD (corresponding to a return rate of 16.6%) responded to the invitation. According to the IIEF Score 160 participants (43.1%) were suffering from more than mild ED. To exclude a selection bias, we additionally calculated the estimated prevalence of ED in the underlying male ACHD population. After adjustment for complexity of disease and age, the estimated prevalence in all men ≥18 years registered in the Register was 36.4%, and in those with mailing contacts available, it was 40.5%.
Baseline characteristics for included ACHD participants overall and stratified into ED and non-ED patients are displayed in Table 1. Patients with ED had similar complexity of underlying ACHD compared to non-ED patients (p=0.29 for simple versus moderate to highly complex congenital heart disease). Underlying congenital heart disease diagnoses are provided in Supplementary Table 2. The participants with ED were older (p<0.05, cutoff age 40 years) and more often reporting of being single (p<0.001). The ACHD with ED reported more often to be anxious about performing sexual activity due to underlying heart defect (p<0.05). Concerning cardiac characteristics, participants with ED were more frequently suffering from heart failure (p<0.05) and were treated with antiarrhythmic drugs (p<0.05). Comorbidities, such as diabetes (p<0.05), cancer (p<0.05) or psychiatric disorders (p<0.05) were more often found in subjects with ED. Also, these participants were more frequently on antidepressant medication (p<0.05).
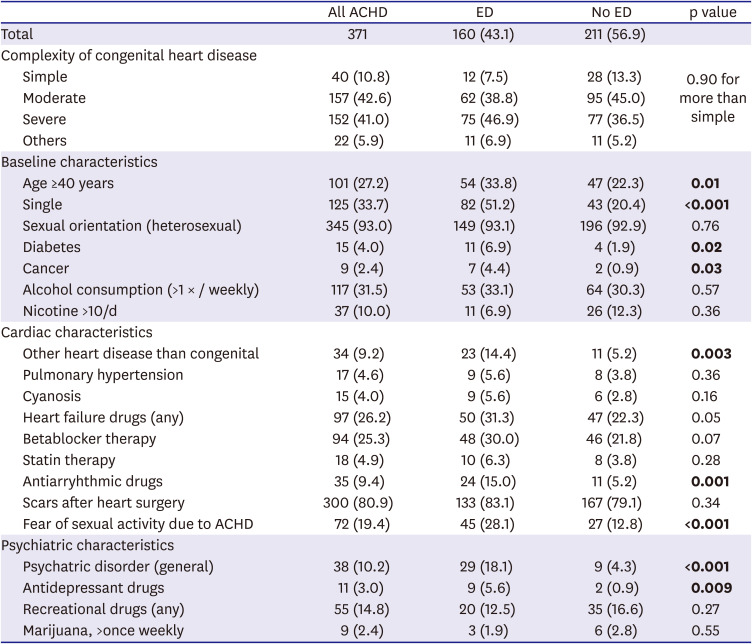
Table 1
Overview over the baseline characteristics of all ACHD that responded to the questionnaire
Patient characteristics are divided into 2 groups for patients with ED and without. Values are presented as number (%). Parameters with significant values are bold.
ACHD = adult congenital heart disease; ED = erectile dysfunction.
![]()
Participants with ED were less frequently sexually active in comparison to participants without ED (p<0.05) (Table 2). Engagement with sex-workers was not exclusive for either analysed cohort of men (p=0.53). Concerning the number of sexual partners, participants without ED tended to be more frequently sexually active with more than one partner (p=0.05). Table 2 additionally describes the use of medicinal aids and drugs for ED and its role in patient-physician communication between the groups. The most commonly used drug type were phosphodiesterase 5 inhibitors (PDE-5 inhibitors) in 68.8% of patients with treated ED. Participants with ED sought medical advice for sexual function more often than participants without ED (p<0.05). Overall, 6.7% of patients (of those 88% with ED) actively approached their treating physician about this issue (p<0.05 with ED compared to non-ED). In contrast, 29.6% of patients (of those 58.2% with ED) would appreciate an active approach by their health care provider to discuss sexual life (p<0.05 with ED compared to non-ED).
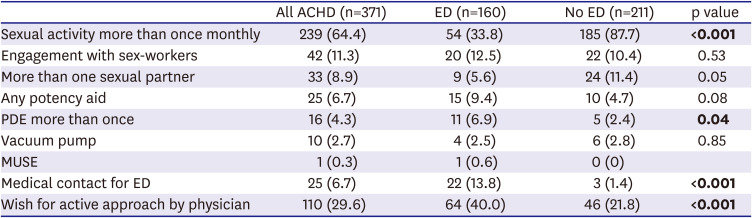
Table 2
Overview over specifics of sexual activity, the role of sexual activity in patient-physician communication and use of medicinal aids and drugs for ED
Male ACHD with ED are compared to patients without ED. Values are presented as number (%). Parameters with significant values are bold.
ACHD = adult congenital heart disease; ED = erectile dysfunction; PDE = phosphodiesterase; MUSE = Medicated Urethral System for Erection.
![]()
On univariable logistic analysis, we identified age ≥40 years, moderate to high complexity of congenital heart disease, but not Fontan circulation only, anxiety to undergo sexual activity due to congenital heart disease, diabetes, being single, diagnosis of heart failure or use of diuretics, use of antiarrhythmic drugs, psychiatric disorder and use of antidepressant drugs as significant predictors for ED (Table 3). On multivariable analysis, age ≥40 years, being single, diagnosis of a psychiatric disorder and anxiety to be sexually active due to ACHD were found to be independent predictors for ED in ACHD (Table 4). Regarding the independent risk factors for ED, anxiety to be sexually active because of ACHD appears to be the only modifiable risk factor. In order to investigate if aesthetic aspects are associated with anxiety, we assessed the correlation between these factors. There was no correlation between scar formation after previous surgery and anxiety to undergo sexual activity (p=0.36). In addition, free text comments of the affected participants suggested that fear of arrhythmia and sudden cardiac death rather than aesthetic issues are related to anxiety during sexual activity in the majority of patients. Of the 44 free-text comments, 19 participants (43.2%) reported about fear of arrhythmia when being sexually active.
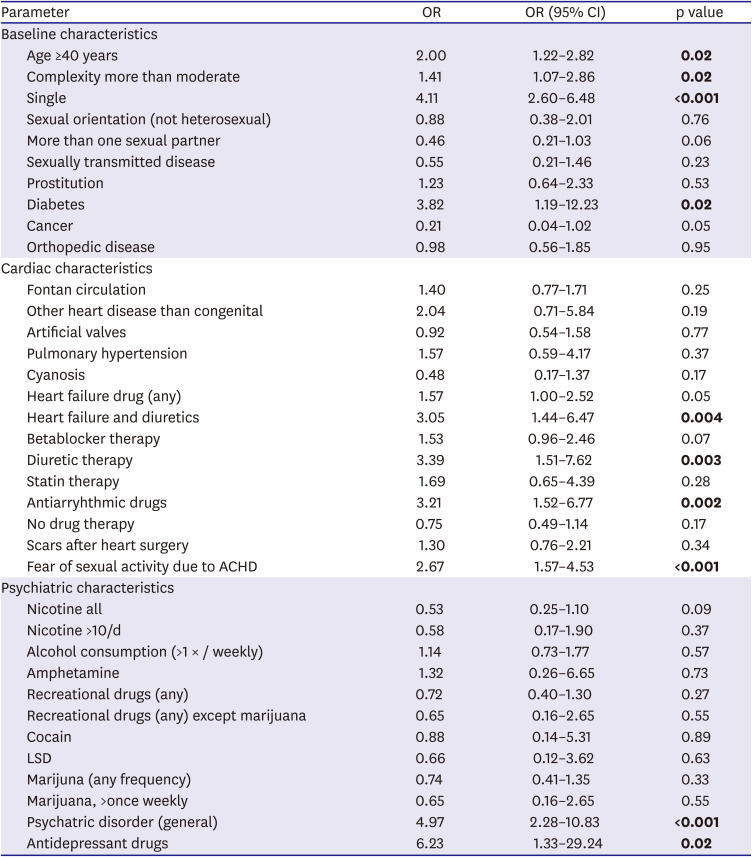
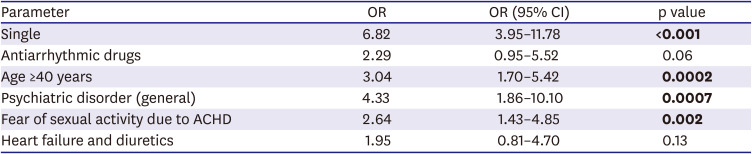
Table 3
Results of the univariable logistic regression analysis for erectile male dysfunction
Parameters with significant values are bold.
ACHD = adult congenital heart disease; CI = confidence interval; LSD = lysergic acid diethylamide; OR = odds ratio.
![]()
Table 4
Significant results of the stepwise multivariable logistic regression analysis for erectile male dysfunction
The following variables were not retained in the model: complexity of congenital heart disease more than moderate, diabetes, antidepressant drugs, nicotine abuse, betablocker therapy only. Parameters with significant values are bold.
ACHD = adult congenital heart disease; CI = confidence interval; OR = odds ratio.
![]()
DISCUSSION
Based on a questionnaire including >300 male ACHD, the current analysis demonstrates that ED is frequent and affects 43% of study respondents and an estimated proportion of 36% of the male individuals included in the German National Register for congenital heart disease. Previously validated and clinically implemented risk scores for ED such as the IIEF14)15) can and should be used in ACHD for risk assessment. As for sensitivity of the subject, the focus should be placed on ACHD at risk, specifically patients older than 40 years, those, who are single and patients with a known psychiatric disorder. A proactive approach to regularly enquire about anxiety to be sexually active and to address ED as a frequent issue in ACHD by healthcare professionals is required and desired by surveyed participants.
In non-ACHD, ED is estimated to occur in 13–71% varying with the age distribution of the study population.7) Generally, age is a major predictor for ED in non-ACHD.17)18) While potentially less prominent in the younger ACHD population with diverse additional risk factors, advancing age also emerged as an independent risk factor for ED in ACHD in our study.
On an organic level, ED is primarily a disease of vascular origin, where specifically endothelial dysfunction plays a role.19) In ACHD, endothelial dysfunction is common and may aggravate the risk of ED in this specific patient cohort.8)20) The influence of vascular dysfunction increases when cardiovascular comorbidities such as arterial hypertension or diabetes are present.19) According to our study, cardiac comorbidities specifically diabetes, diagnosis of heart failure and use of diuretics emerged as predictors for ED on univariable analysis, although not on the multivariable analysis.
In addition to these conventional risk factors for ED, hemodynamic limitations that theoretically increase with complexity of the underlying congenital heart disease may affect sexual life. In patients with more complex congenital heart disease, exercise capacity is depressed.9) Hemodynamic limitations during exertion could therefore play a role. These aspects could not be objectified in our analysis, but diagnosis of moderate to highly complex congenital heart disease was identified as a predictor for ED on univariable analysis, albeit not reaching statistical significance on multivariable analysis. However, complexity of congenital heart defects may have an impact on ED in ACHD especially through its association with co-morbidities, heart failure and arrhythmias.10)11)21)
Beyond organic causes, psychological and sociodemographic factors influence erectile function.7) According to our analysis, being single is associated with ED in ACHD. In non-ACHD, never having been married, being separated or divorced has been described as a predictor for ED.18) Family support is linked to a generally better quality of life potentially lowering psychological distress in ACHD.22) Concerning erectile function, a reassuring environment may reduce psychological distress and thus, be associated with less ED. Alternatively, participants with ED may decide not to involve themselves in relationships in the first place.23) We, thus, cannot exclude the possibility of reverse causation in this setting but the mere association may allow for risk stratification in the clinical setting by obtaining information on patients' partnership status.
Previous diagnosis of a psychiatric disorder has been identified as an independent predictor for ED in our study. This finding is consistent with previous studies, reporting that anxiety and depression are associated with ED in ACHD.4)5) For non-ACHD, psychiatric disorders, particularly depression and anxiety were also associated with ED.24) These psychiatric disorders are relatively frequent in ACHD.25)
Psychologic factors influencing erectile function are not mandatorily linked to manifest psychiatric diseases. Anxiety to be sexually active due to underlying heart defect that was reported by 19% of ACHD, was identified as an independent predictor for ED in our study. Previous studies showed a high rate of anxiety and fear evoked by multiple previous hospitalizations.25) According to patient comments in our analysis, patients' fear was most often grounded on fear of arrhythmia and sudden cardiac death related to sexual activity. This anxiety may partly be justified as a considerable number of patients received antiarrhythmic drugs and the use of antiarrhythmic drugs was associated with ED albeit not reaching statistical significance in our analysis. An interrelation between antiarrhythmic drug usage and sexual function is not well investigated. Dobs et al.26) showed that amiodarone, one of the most frequently used antiarrhythmic drugs, leads to a testicular dysfunction in a prospective case-control analysis. According to their analysis, however, sexual dysfunction in itself is not affected by the intake of amiodarone. Therefore, the particular challenge for health care providers is, to identify those patients in whom the concern is justified versus those in whom psychological distress is the leading cause. If distress is the leading reason, it may be resolved through an empathic conversation with an open patient-physician communication or formal psychological support.
However, unfortunately, communication about sexual function remains a neglected subject in clinical practice.2) According to our analysis, irrespective of underlying ED, almost 30% of patients would favor a proactive approach by physicians concerning this issue. Neglecting ED as a subject in regular clinical contacts may not only influence quality of life but can also have detrimental clinical implications when patients are not sufficiently informed about potential risks and side effects of ED medication that patients may obtain independently. The most commonly used potency aids/medications in the study population were PDE-5 inhibitors, which are also the first line therapy according to current guidelines.27) Generally, data on safety of PDE-5 inhibitors in ACHD without the indication of pulmonary arterial hypertension is scarce.28) Due to the hemodynamic effects of this vasorelaxant drug, intake under regular professional surveillance is preferable depending on severity of congenital heart disease.
There are some limitations to our study. This is a study based on the German NRCHD. Despite the size of the Register, only 10,738 patients were older than 18 years and 2,234 had e-mail contacts available. The 371 male patients (16.6%) responded to the survey, thus limiting the statistical power of analyses. This return rate is, however, within the expected range for this type of online questionnaire study. The informative value of the analysis in clinical practice is improved as there was no preselection of ACHD. For validity of responses, the underlying disease complexity was cross-referenced against the objective medical data available in the Register database by providing different access links by disease severity groups. Due to the sensitivity of the study subject, we refrained from fully unblinding respondents by fully linking them to their medical dataset. The subset of patients with an e-mail contact available was not entirely reflective of the underlying overall Register cohort. Additionally, as for not linking responses to the medical dataset, we cannot exclude the possibility of misinterpretation of the questions by the respondents. For example, Beta-blocker therapy may or may not be assessed as an antiarrhythmic drug therapy. Inclusion of betablocker intake to antiarrhythmic drug treatment potentially, at least in part, may explain the association between antiarrhythmic drug use and ED in our study.
In conclusion, ED is frequent affecting one third to one half of adult patients with congenital heart disease based on a questionnaire-based analysis. Awareness of and attention to sexual health should be integrated into routine care particularly in patients of advanced age, when diagnosis of a psychiatric disorder is known and those, who are not living in a relationship. Given the prevalence of ED and its important potential implications on quality of life, assessment for ED should be standard of care in the ACHD clinic with referral for specialist management when needed. Inquiring about ED should be as routine for ACHD specialists as asking patients about desire to have children, contraception and adequacy of dental hygiene.
 XML Download
XML Download