

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia, and its prevalence is increasing every year.1)2) AF causes stroke, congestive heart failure, and sudden cardiac death.3) The mortality and morbidity of AF, including increasing the frequency of hospitalization, place large socioeconomic burdens on society.4) Many risk factors for AF have been reported, such as aging, male sex, hypertension, obesity, sleep apnea; however one of the most important preventable risk factors is alcohol consumption.5)
Previous observational studies have shown that alcohol consumption affects the incidence of AF through different mechanisms depending on drinking behavior.6) Generally, previous observational studies used multivariate models adjusted for confounders to evaluate the association between alcohol consumption and AF.7) However, it is difficult to conclude causality from the results of observational studies because numerous factors, including individual characteristics such as socioeconomic status, lifestyle, and demographics, affect the pattern of drinking.8) For instance, it is impossible to correct for all confounders and to rule out reverse causation in observational studies.9)
One of the methods for evaluating causality between exposure and outcome is the instrumental variable (IV) method. When a variable is causally associated with the exposure, the outcome is affected only by the exposure; the variable is not associated with any confounders between the exposure and outcome, and the variable can be used as an IV substituting for the exposure.10) If some genetic polymorphisms are used as IVs which satisfy the assumptions, the method of analysis is called the Mendelian randomization (MR) method. As genetic polymorphisms cannot be affected by other factors, the analysis is performed under the assumption of random allocation according to genetic variants, and the results are relatively free from confounding and reverse causation.11)
Alcohol is metabolized through several stages after ingestion. The major pathway involves 2 enzymes: alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH). First, ethanol is dehydrogenated to acetaldehyde by ADH. Thereafter, acetaldehyde is metabolized to acetate by ALDH.12) A functional single nucleotide polymorphism in the ALDH2 rs671 gene results in the reduced function of ALDH and the accumulation of aldehyde after alcohol ingestion.13) The accumulated aldehyde cannot be removed from the body, and a syndrome called “Oriental flushing” occurs, consisting of a series of symptoms including facial flushing and nausea. These unpleasant symptoms prevent people who have the syndrome from drinking alcohol.14) Consequently, ALDH2 polymorphism may be the most potent IV as the genetic predisposition for alcohol consumption.15)
Previous studies have used genetic variants to evaluate the relationship between alcohol and AF. In Japan, a case-control study in hospitalized patients showed an association between genetic polymorphism and AF.5) However, the dataset used in the study was not available for alcohol consumption, the effect size of alcohol on AF could not be estimated. Meanwhile, three genome-wide association studies that performed two-sample MR reported conflicting results. As all studies did not use the ALDH2 gene as an IV, their results may not be applicable for the East Asian population.16)17)18) In the present study, we performed the MR analysis using ALDH2 rs671 to examine the causal association between alcohol and AF in Korea.
METHODS
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital (IRB No. I-2008-05-056). Informed consent was obtained from all participants when they were enrolled in baseline examination.
Subjects
The study participants were from the Dong-gu Study, which included residents of the Dong District, Gwangju, Korea. The cohort included 9,260 participants, and the baseline survey was conducted from May 2007 to July 2010.19) From the cohort, 296 participants were excluded because of missing values in ALDH2 rs671 genotypes, physical activity, alcohol drinking frequency, amount of alcohol consumption at one time, smoking history, height, weight, hypertension, diabetes, educational status, and AF. Finally, 8,964 subjects were included in this study.
Covariates
Information on age, physical activity, alcohol consumption in standard glasses per day, smoking history, body mass index (BMI), hypertension, diabetes, education status, history of coronary heart disease (CHD), high density lipoprotein (HDL), low density lipoprotein (LDL), triglyceride (TG) and AF were obtained from the Dong-gu Study dataset. We defined physical activity as walking at least five times a week and for >30 minutes at a time. Alcohol consumption was estimated using the number of days of drinking alcohol per week and the number of standard glasses of alcohol consumed per drinking day. In addition, alcohol consumption was categorized into 4 categories; never drinker, former drinker, light to moderate drinker (<2 drinks/day in men, <1 drinks/day in women), and heavy drinker (≥2 drinks/day in men, ≥1 drinks/day in women).20) The converted amount by beverage type was included in the question on the amount of alcohol consumption, preventing the participants from measuring their consumption differently for different beverage types. Smoking status was classified as never, former, or current. Participants who had smoked <5 packs in their lifetime were defined as never smokers. For the rest of the participants, the question “Do you smoke currently?” was used to distinguish between current smokers and former smokers. BMI was calculated using the measured height and weight, and the participants were categorized into the underweight, normal, overweight, and obesity groups according to the World Health Organization cutoff criteria.21) Participants who were diagnosed or had a medication with hypertension or had a measured blood pressure of ≥140/90 mmHg were defined as having hypertension. Participants who were diagnosed or had a medication with diabetes or had a measured serum glucose level of ≥126 mg/dL were defined as having diabetes. Education status was divided into groups based on an education duration of >9 years.
Genotyping
Following the manufacturer’s protocol, DNA was extracted with QIAamp DNA Blood Mini Kit (QIAGEN, Valencia, CA, USA) from peripheral blood. As previously described,22) rs671 was genotyped by high-resolution melting (HRM) analysis using a Rotor-Gene 6000 (Corbett Research, Sydney, Australia). The polymerase chain reaction (PCR) primers (forward, 5′-TTGGTGGCTACAAGATGTCG-3′; reverse, 5′-CAGGTCCCACACTCACAGTTT-3′) produced a 97-bp amplicon. The reaction mixture was used for HRM and consisted of 200 nM PCR primer, 1 µM SYTO 9 fluorescent dye (Invitrogen, Carlsbad, CA, USA), 0.5 U F-Star Taq polymerase (BioFACT, Daejeon, Korea), and 40 ng genomic DNA in 10-µL reaction volumes. PCR was started at 95°C for 5 minutes, followed by 40 cycles of 95°C for 5 seconds and 58°C for 30 seconds.
Outcome measures
The participants underwent 12-lead electrocardiography using HP-PageWriter 200 M1771A (Hewlett Packard, Andover, MA, USA) at baseline survey. The recorded electrocardiograms were preliminary analyzed using the Philips 12-lead algorithm and potential cases of AF were identified by 2 cardiologists. In addition, participants who had been treated for AF before the baseline survey were classified as patients with AF.
Statistical analyses
Because alcohol consumption has significant differences between men and women,23) sex stratification was implemented in all analyses. Since the frequency of the AA genotype was low, the GA and AA genotypes were combined. The characteristics of participants according to ALDH2 genotypes were presented as the mean ± SD or number (%), compared using independent t-test or χ2 test was conducted. Age adjusted prevalence of AF according to categorized alcohol consumption was presented using logistic regression. Simple logistic regression and multivariate logistic regression analyses were performed as observational analyses to identify the effect of alcohol consumption on AF. To assess the impact of ‘sick quitter,’ meaning that disease may alter health behavior, observational analyses were conducted in population without former drinkers as sensitivity analysis. In addition, to investigate the effect of heavy drinking on AF, sensitivity analysis was performed in which alcohol consumption were treated as categorical variable. To show the association between ALDH2 polymorphism and AF, univariate and multivariate logistic regression analyses were conducted. Multivariate logistic regression models were adjusted for age, physical activity, smoking status, BMI category, hypertension, diabetes, and education status. In addition, in a sensitivity analysis to assess the pleiotropic effect between ALDH2 genotypes and AF, we adjusted for the potential confounders or mediators such as CHD history, HDL, LDL, and log transformed TG. These variables were reported in the Phenoscanner as an ALDH2 related phenotypes which is the database holding publicly available results from large-scale genome-wide association studies.24)25) A 2-stage MR analysis was performed to evaluate the association between the genetically predicted daily alcohol consumption and AF in men because the difference in the amount of alcohol consumption between men and women was not significant according to ALDH2 genotypes. In the first stage, to obtain genetically predicted log transformed alcohol consumption, linear regression analyses of alcohol consumption on the ALDH2 genotypes were performed. Because alcohol consumption had a left-deviated distribution, the amount of alcohol consumption was used in the model, which was modified by adding the minimum amount of alcohol consumption and log transformation. In the second stage, the association between the back-transformed predicted amount of alcohol consumption and AF was estimated using a univariate and multivariate logistic regression model that included age, physical activity, smoking history, BMI, hypertension, diabetes, and education status. The same MR analyses were conducted as sensitivity analyses in participants excluding former drinkers. All analyses were performed using R (version 4.0.2; The R Foundation, Vienna, Austria).
RESULTS
The characteristics of participants according to genotypes are presented in Table 1. The GG genotype group drank more alcohol and was younger than the GA/AA group in both sexes. Hypertension and diabetes were more prevalent in GG genotype group than GA/AA genotype group in men. There were more smokers in GG genotype group than GA/AA genotype group in women.
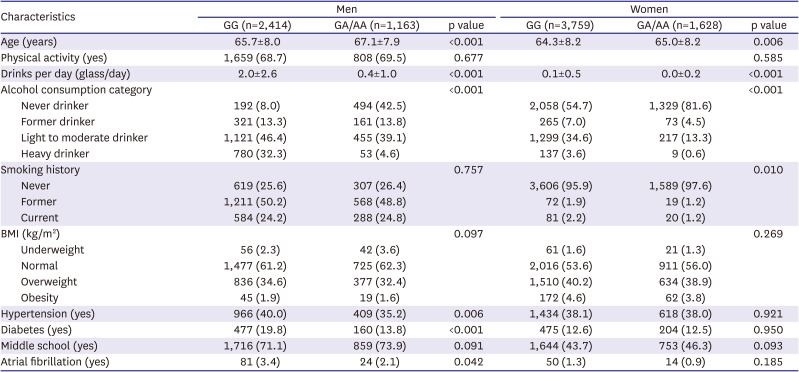
Table 1
Baseline characteristics of the study population according to ALDH2 rs671 genotypes
All values are presented as the mean ± SD or number (%). Independent t-test and χ2 tests were conducted for continuous and categorical variables, respectively.
Alcohol consumption was categorized into 4 groups: never drinker, former drinker, light to moderate drinker (<2 drinks/day in men, <1 drink/day in women), and heavy drinker (≥2 drinks/day in men, ≥1 drink/day in women).
BMI was categorized into 4 groups: underweight (less than 18.5), normal (18.5–24.9), overweight (25.0–29.9), and obesity (30.0 or more).
ALDH2 = aldehyde dehydrogenase 2; BMI = body mass index.
![]()
Figure 1 showed the age-adjusted prevalence of AF according to never drinker, former drinker, light to moderate drinker, and heavy drinker. The highest proportion of prevalent AF was observed in the former drinkers in both sexes. However, significant difference of age-adjusted prevalence of AF among alcohol consumption was shown only in women. There was no prevalent case of AF in women heavy drinkers.
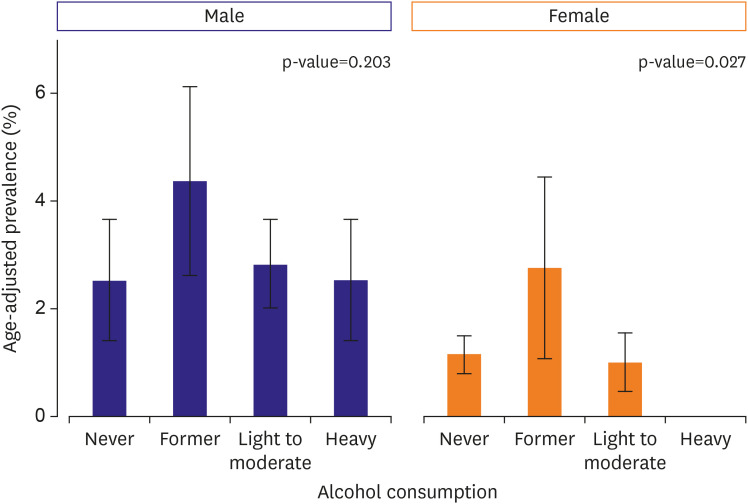
Table 2 presents the association between the amount of alcohol consumption and AF in the observational analysis using logistic regression models. In a simple logistic regression, age, current smoking status and hypertension were associated with AF in men. Age, hypertension, and educational status were associated with AF in women. In adjusted model, no significant association was observed between the amount of alcohol consumption and AF in men (adjusted odds ratio [OR], 0.99; 95% confidence interval [CI], 0.90–1.08) and in women (adjusted OR, 0.38; 95% CI, 0.03–1.19). A sensitivity analysis excluding former drinkers yielded similar result (Supplementary Table 1). The association between categorized alcohol consumption and AF was presented in Supplementary Table 2. In men, alcohol consumption was not associated with AF. In women, former drinkers were associated with an increased risk of prevalent AF compared to never drinkers, while light to moderate drinker was not.
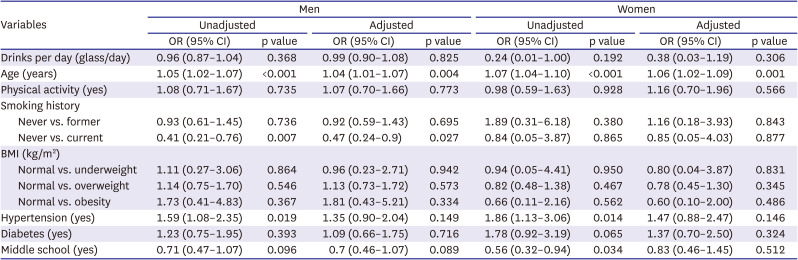
Table 2
Association between alcohol consumption (drinks per day) and atrial fibrillation in the observational analysis
Multivariate logistic regression models were adjusted for age, physical activity, smoking status, BMI category, hypertension, diabetes, and education status.
BMI = body mass index; CI = confidence interval; OR = odds ratio.
![]()
Table 3 presents the associations between ALDH2 polymorphism and AF. In men, the GG genotype had a higher risk of AF (adjusted OR, 1.69; 95% CI, 1.08–2.74). In women, the association between ALDH2 genotypes and AF was not significant (adjusted OR, 1.55; 95% CI, 0.88–2.93). After further adjustment of CHD history, HDL, LDL and log transformed TG, ALDH2 genotype was associated with AF (adjusted OR, 1.71; 95% CI, 1.08–2.79) in men (Supplementary Table 3).
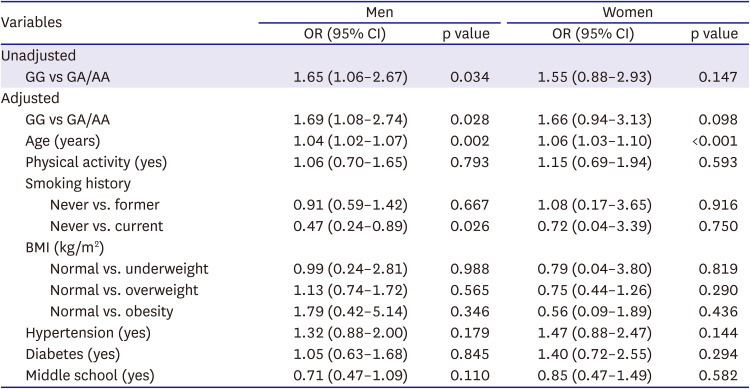
Table 3
Association between atrial fibrillation and rs671 polymorphisms by sex
Multivariate logistic regression models were adjusted for age, physical activity, smoking status, BMI category, hypertension, diabetes, and education status.
BMI = body mass index; CI = confidence interval; OR = odds ratio.
![]()
The results of MR analyses are shown in Table 4. The MR analysis was conducted in men, because there was a significant association between ALDH2 polymorphism and AF only in men. Although the observational analyses did not show significant relationships, there was a positive relationship between predicted alcohol consumption and AF in univariate (OR, 3.00 [95% CI, 1.13–8.68]) and multivariate model (OR, 3.17 [95% CI, 1.18–9.24]). However, in a sensitivity analysis except former drinkers, this association was attenuated and remained significant in both univariate (OR, 2.05 [95% CI, 1.05–4.28]) and multivariate model (OR, 2.12 [95% CI, 1.08–4.44]). The F statistics and adjusted R2 of MR model were 864.6 and 19.5% in total subjects and 1,212 and 28.1% in subjects except former drinkers.
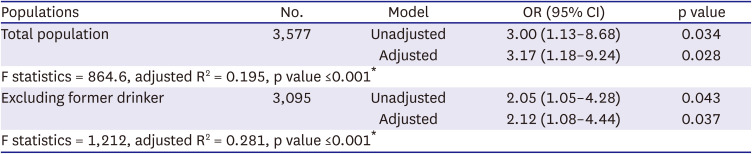
Table 4
Association between genetically predicted alcohol consumption (glass/day) and atrial fibrillation in men
Log-transformed alcohol consumption in men was estimated and inversely transformed according to whether the ALDH2 rs671 genotype was GG or GA/AA.
All models were adjusted for age, physical activity, smoking status, body mass index category, hypertension, diabetes, and education status.
ALDH2 = aldehyde dehydrogenase 2; CI = confidence interval; OR = odds ratio.
*F statistics, adjusted R-squared, and p value of regression model which predicted log-transformed alcohol consumption using ALDH2 genotype GG or GA/AA.
![]()
DISCUSSION
We conducted an MR analysis to identify the causal association between alcohol consumption and AF. The relationship between alcohol consumption and AF seemed to be insignificant in the observational analysis. The MR analysis with genetically predicted alcohol consumption showed a causal association in men.
Previous studies identifying the link between alcohol consumption and AF using genetic factors presented conflicting results. In a Japanese study in 200 hospital inpatients, there was a significant difference in the distribution of ALDH2 and ADH1B genotypes between patients with AF and patients with other diseases. Patients with AF have a lower frequency of the dysfunctional ALDH2 allele and a higher frequency of the dysfunctional ADH1B allele, suggesting that higher alcohol consumption may be associated with AF. Unlike ALDH2 variants, dysfunction of ADH1B slows the metabolism of alcohol to aldehyde, leading to increased alcohol consumption.5) In addition, three previous MR studies examined the causal relationship between the amount of alcohol consumption and AF, which was unaffected by confounders. All studies were two-sample MR studies, and most of the study participants were of European ancestry. In the two-sample MR study performed by Jiang et al.,16) genetically predicted alcohol consumption was not associated with AF. However, in the study by Larsson et al.,17) genetically predicted alcohol consumption was positively associated with AF, and in the study by Lu et al.,18) a positive relationship was found between genetically predicted heavy drinking (>35 units/week in women and >50 units/week in men) and AF.
In our study, a significant relationship between alcohol consumption and AF was observed only in the MR analysis in men. This discrepancy in results between the observational analysis and MR analysis may be caused by unknown confounding factors in the relationship between alcohol consumption and AF. In women, both the observational and genetic analyses did not present a significant relationship between alcohol consumption and AF. The sex differences in the distribution of alcohol consumption among rs671 genotypes led to the sex difference in the MR analysis results. In women, the amount of alcohol consumption was relatively lower than that in men because alcohol consumption is socially proscribed for women. Therefore, in women, physiologic discomfort due to ALDH dysfunction may not play a large role in determining the amount of alcohol consumption.26)
In an MR analysis, several assumptions need to be satisfied for a variable to be used as a genetic instrument. First, the genetic variant is associated with the factor (relevance assumption). Second, there is no unknown confounder between genetic variants and outcome (independence assumption). Third, the genetic variants affect the outcome only through risk factors (exclusion restriction). If the relevance assumption is not met, a ‘weak instrument problem’ occurs, such as weak statistical power and increased bias due to pleiotropic effects. The relevance assumption is tested by checking whether the F statistic exceeds 10. The F value of the regression model for the alcohol consumption of the ALDH2 genotype in this study is 864.6, so there is probably no violation of the relevance assumption. Independence assumption and exclusion restriction assumptions can be evaluated in “Negative control” populations which are rarely exposed to risk factors. These assumptions can be satisfied if IV is not associated with the outcome in these populations.11) In the present study, alcohol consumption of women was close to zero, and there was no significant association between ALDH2 polymorphism and AF in women. In addition, ALDH2 was associated with AF after further adjustment for potential confounders or mediators which are the phenotypes known to be associated with the ALDH2 rs671 genotype. Thus, the ALDH2 polymorphism may be suitable IV on alcohol consumption in the present study. Furthermore, previous study reported ALDH2 variants are the credible genetic IV for MR studies of alcohol consumption.27)
Some limitations could be considered in this study. First, alcohol consumption may have not been accurately measured. In this study, the average daily alcohol consumption was calculated using the questionnaire responses of participants about the monthly drinking frequency and the amount of alcohol consumed at one time, and this value was used for all analyses. In the same context, former drinkers were treated as nondrinkers regardless of the amount of alcohol they had consumed in the past. To assess the bias in evaluating the relationship between alcohol consumption and AF due to the problem in the categorization of former drinkers, a sensitivity analysis was conducted including only current and never drinkers, in whom the effects of alcohol consumption could be clearly determined. Third, undiagnosed paroxysmal AF may have been missed and the prevalence may have been underestimated in the total participants. Clinically, AF can be classified into three categories: paroxysmal, persistent, and permanent. This classification depends on whether the AF is terminated spontaneously and how long the AF is sustained. The management and prognosis of AF can differ according to the classification.28)29) To include patients with paroxysmal AF in our study, we included patients who had been diagnosed with AF, or were being treated for AF. Fourth, the MR results may be ethnic specific because ALDH2 polymorphism exists only in East-Asian.30)
In conclusion, genetically predicted alcohol consumption based on the rs671 polymorphism is associated with AF. This result suggests that the association between AF and alcohol consumption may be causal.
 XML Download
XML Download