

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mitral regurgitation (MR) is the most frequent valvular heart disease requiring surgical intervention.1)2) Optimal timing of surgical treatment of severe MR is crucial for preventing adverse clinical outcomes. Current guidelines recommend mitral valve (MV) surgery for patients with severe MR and overt symptoms, left ventricular (LV) systolic dysfunction, atrial fibrillation (AF), or pulmonary hypertension.3) Significant dilation of the left atrial (LA) is also a poor prognostic marker and is included as a class IIa indication for surgery, even in asymptomatic patients with severe MR.3) During the early phase of MR, LA compensates for the increase in regurgitant volume by augmenting its reservoir function.4)5) However, LA no longer compensates for chronic volume overload that occurs in advanced phase; consequently, LA adverse remodeling occurs, manifesting as LA dilatation and dysfunction. LA dilatation may be accompanied by cellular hypertrophy and interstitial fibrosis, with increased vulnerability to the development of AF and LA dysfunction.6) Recently published studies have shown decreased LA reservoir function even in the early stage of LA structural changes. Thus, decreased LA reservoir function may indicate the hemodynamic implications of severe MR at an earlier stage than that of overt LA structural changes.7)8) Furthermore, decreased LA function is associated with a poor long-term prognosis in patients with several cardiovascular diseases.9)10) However, the prognostic significance of LA function in patients with severe MR remains unclear. The assessment of LA reservoir function by speckle-tracking echocardiography can provide an objective marker of LA function and may have prognostic implications in patients with severe MR after MV surgery. Therefore, we assessed the LA global longitudinal strain (LAGLS) by speckle-tracking echocardiography and evaluated its prognostic impact in patients with chronic severe MR requiring MV repair surgery.
METHODS
Ethical statement
The study protocol was approved by the Asan Medical Center Institutional Review Board (2019-0553) and performed in accordance with the Declaration of Helsinki. The need for informed consent was waived due to the retrospective nature of the study.
Study population
The study population comprised consecutive patients with chronic severe MR who underwent successful MV repair surgery at Asan Medical Center (Seoul, South Korea) from January 2012 to December 2017. A diagnosis of severe MR required more than 4 of the following criteria: (1) flail leaflet; (2) vena contracta width >0.7 cm; (3) proximal isovelocity surface area (PISA) radius >1.0 cm at an aliasing velocity of about 40 cm/s; (4) regurgitant jet area >50% of the LA; and (5) pulmonary vein systolic flow reversal. If only 2–3 criteria were met, ≥1 qualitative parameter were necessary, especially with an effective regurgitant orifice area ≥0.4 cm2 or regurgitant volume ≥60 mL, using the PISA method. Patients with a baseline LV ejection fraction (LVEF) <50%, AF/flutter rhythm at baseline, significant concomitant aortic valve disease, previous MV surgery, and more than a moderate degree of residual MR after surgery were excluded.
Echocardiographic evaluation
Conventional echocardiographic analysis
Transthoracic echocardiography was performed as routine clinical practice and baseline study was performed within 7 days before MR surgery, using commercially available echocardiographic systems (iE33 and Epiq7, Philips Healthcare, Andover, MA, USA; Vivid 7 and E9, General Electric Healthcare, Waukesha, WI, USA). Digitally stored images were retrospectively analyzed by an experienced cardiologist specialized in valvular heart diseases. MR severity was assessed using the following parameters: valve morphology, jet area, vena contracta width, pulmonary vein flow pattern, and proximal convergence method with a multi-parametric integrative approach.11) LV and LA chamber quantification were performed following the recommendations of the American Society of Echocardiography,12) LA anteroposterior linear diameter was measured at the end-systole along the parasternal long-axis view using M-mode echocardiography. LV and LA volumes were assessed from apical 4- and 2-chamber views using Simpson’s biplane method and indexed by the body surface area. LA maximal and minimal volumes were measured just before MV opening (Volmax) and at MV closure (Volmin), respectively. The LA expansion index was calculated as (Volmax − Volmin/Volmin × 100).13) The diastolic properties of the LV were analyzed by the mitral inflow pattern, including the early mitral inflow velocity (E), deceleration time, and late mitral inflow velocity (A).14) Doppler tissue interrogation of the early diastolic mitral annular relaxation velocity (E′) and late diastolic velocity (A′) were recorded at the septal annulus, and the E/E′ ratio was used to estimate the LV filling pressure.15) The systolic pulmonary artery pressure (SPAP) was assessed by the maximal velocity of the tricuspid regurgitation (TR) jet using the modified Bernoulli equation,16) and right atrial pressure was estimated by the inferior vena cava diameter and its response to inspiration.17) Significant pulmonary hypertension was defined as an estimated SPAP ≥50 mmHg. Right ventricle (RV) systolic function was estimated by the systolic velocity of the lateral annulus of the tricuspid valve, with a velocity <9.5 cm/sec indicating RV systolic dysfunction.12)
Speckle-tracking echocardiographic analysis
Speckle-tracking echocardiography was used to evaluate LA myocardial function. An experienced investigator analyzed the LA strain using off-line software (TomTec Imaging Systems 2D Cardiac Performance Analysis, Germany) and greyscale LA images obtained in both apical 4- and 2-chamber views (frame rate, 60–80 frames/s).18) After importing digitally stored cine echocardiographic images to the software, the LA endocardial border was manually drawn using a point-and-click approach. Then, the software automatically performed endocardial border tracking. If the entire cardiac wall was not covered from the endocardium to the epicardial border, manual adjustments were performed to optimize the tracking. After segmental tracking quality analysis and final manual corrections, longitudinal strain and strain rate curves were generated in all segments, and the average value was calculated for the corresponding time points.19) We used R-R gating in the strain analysis, with the onset of the QRS complex as the reference point. Two peaks representing LA reservoir function (first peak) and LA contractile function (starting at the P wave onset) were obtained. The LAGLS was calculated by averaging the first peak-positive LA strain values observed in all LA segments from apical 4- and 2-axis views.20)
Outcomes and follow-up
Postoperatively, patients regularly visited physicians in the outpatient clinic at 3- to 6-month intervals. Clinical follow-up data, including postoperative clinical events, until the end of December 2019, were obtained by a review of the registry data and medical records. The primary study endpoint was adverse cardiovascular events, defined as the composite of all-cause death, newly developed AF (persisting 5 days after MV repair), and re-hospitalization for cardiovascular causes (nonfatal stroke, MV reoperation, and heart failure). Stroke of any type was defined using clinical documentation, with confirmatory imaging findings. Heart failure was defined according to the Framingham criteria, with the presence of two major, or one major and two minor criteria.21) Dates and causes of death were obtained from medical records for patients with regular clinical follow-up, or from the Korean National Registry of Vital Statistics for patients without regular follow-up.
Statistical analysis
Continuous variables are presented as the mean ± standard deviation or median (interquartile range); categorical variables are presented as numbers and percentages. Group comparisons were evaluated using the chi-square or Fisher exact test for categorical variables, and the Student t-test or Mann-Whitney U test for continuous variables, as appropriate. Cox proportional hazard analysis was used to identify prognostic factors significantly associated with study outcomes, with adjustment for the effects of covariates in a multivariate analysis. Clinically relevant covariates with p<0.1 on univariate analysis were added in the multivariate model. Time-dependent receiver-operating characteristic (ROC) curve analysis was performed, and area under the curve (AUC) was calculated for the prognostic value of baseline LAGLS to predict cardiovascular events. The most accurate cutoff value (i.e., the best compromise between sensitivity and specificity) was obtained using the Kaplan-Meier (KM) estimation method at 5 years after MV surgery. To examine the effect of baseline LAGLS in different subsets of patients, subgroup analyses were conducted according to the echocardiographic variables which were significant in the multivariable model (age, sex, LV end-systolic dimension, LA maximal volume index (LAVimax), and estimated SPAP). Adjusted hazard ratios (HRs) were calculated using the Cox proportional-hazards model. Time-to-event curves were constructed using KM estimates, and group comparisons were performed using the log-rank test. All reported p values are 2-sided, and p<0.05 were considered statistical significance. All statistical analyses were performed using the SPSS version 21.0 (IBM, Chicago, IL, USA) and R software version 3.4.0 (R Foundation, Vienna, Austria).
RESULTS
During the study period, 718 patients with chronic severe MR underwent MV repair surgery in the Asan Medical Center (Seoul, South Korea). Among them, 380 patients were excluded for several reasons including AF/flutter at the baseline (n=253 patients), significant concomitant aortic valve disease (n=53 patients), LVEF <50% (n=32 patients), previous MV surgery (n=16 patients), with moderate or severe residual MR after the surgery (n=6 patients), and concomitant LA reduction or Maze operation (n=12 patients). Finally, 338 patients (mean age, 51.9±12.5 years; 218 male) were analyzed (Supplementary Figure 1). During a median follow-up of 45 months (interquartile range, 26–65 months), there were 30 (8.9%) adverse cardiovascular events, 5 (1.5%) all-cause deaths, 8 (2.4%) newly developed AF, and 26 (7.7%) re-hospitalizations for cardiovascular causes. Patients with and without cardiovascular events had similar clinical and operative characteristics (Table 1). Annuloplasty was performed in 333 (98.5%) patients, and 209 (61.8%) received a leaflet plication. Concomitant procedures, including tricuspid valve annuloplasty, coronary artery bypass graft surgery, and atrial septal defect closure were performed in 45 (13.3%) patients.
Table 1
Comparison of baseline characteristics between patients with and without cardiovascular events
Data are expressed as number (%) or mean ± standard deviation.
ASD = atrial septal defect.
*Renal failure was defined as an estimated glomerular filtration ratio of <30 mL/min/1.73 m2 or dialysis.
![]()
Echocardiographic data before and after mitral valve repair surgery
Baseline echocardiographic data are summarized in Table 2. Most patients showed primary MR (98.8%), including MV prolapse/flail (96.4%) and rheumatic disease (2.4%). The two groups did not significantly differ in LV dimensions, LVEF, diastolic properties of the LV, and degree of MR. Baseline LA anteroposterior dimension and volume index were larger in patients with cardiovascular events than in those without events. In addition, the LAGLS and expansion index were lower in patients with cardiovascular events than in those without events. The estimated RA pressure, SPAP, and presence of RV dysfunction were greater in patients with cardiovascular events than in those without events. Follow-up echocardiographic data obtained in the immediate postoperative period and 1-year postoperatively are shown in the Supplementary Table 1. After MV repair surgery, all patients showed considerable reductions in the LA diameter (baseline, 48.0±6.8 mm; immediately postoperatively, 42.5±6.0 mm; 1-year postoperatively, 39.3±5.8 mm) and LAVimax (baseline, 96.0±44.8 mL/m2; immediately postoperatively, 68.0±34.9 mL/m2; 1-year postoperatively, 49.5±19.5 mL/m2). Although the LAGLS decreased immediately after surgery, it improved at 1-year postoperatively. Patients without cardiovascular events had smaller maximal LA diameter and LAVimax values at baseline, immediately postoperatively, and 1-year after surgery compared to those with events (Figure 1). LAGLS values were significantly lower in patients with cardiovascular events before and after MV repair surgery compared to those in patients without events (Figure 2).
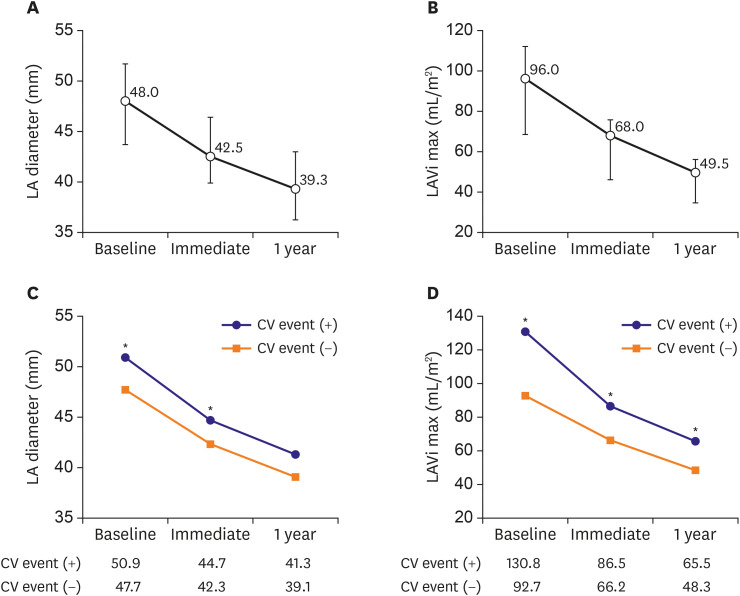
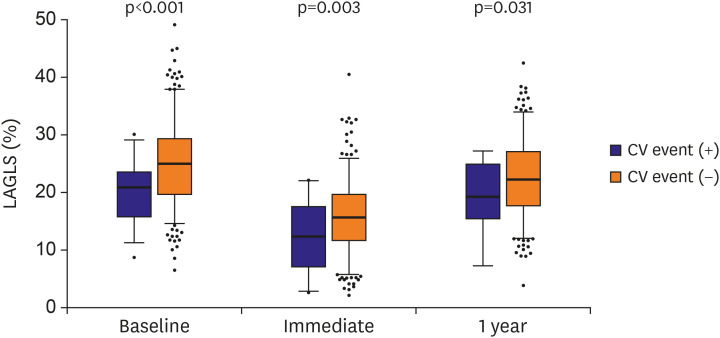
Figure 1
Change in LA size and volume before and after mitral valve repair surgery. LA anteroposterior diameter and LAVimax are shown for all patients (A and B) and for patients with or without CV events (C and D). Data are displayed as the median value, with 25th and 75th percentiles (whiskers).
CV = cardiovascular; LA = left atrial; LAVimax = left atrial maximal volume index.
*p < 0.05.
![]()
Figure 2
Time course of the LA global longitudinal strain before and after mitral valve repair surgery. The LA global longitudinal strain at baseline, immediately after surgery, and 1-year after surgery is shown according to presence of CV events. Box-plot indicates the median value, and the 25th and 75th percentiles; whiskers depict the 2.5th and 97.5th percentiles.
CV = cardiovascular; LA = left atrial.
![]()
Table 2
Comparison of baseline echocardiographic parameters between patients with and without cardiovascular events
Data are expressed as number (%) or mean ± standard deviation.
AR = aortic regurgitation; LA = left atrium; LV = left ventricle; MR = mitral regurgitation; PISA = proximal isovelocity surface area; RA = right atrium; RV = right ventricle; SPAP = systolic pulmonary artery pressure; TR = tricuspid regurgitation.
![]()
Left atrial function and clinical outcomes
On multivariate Cox-proportional hazard analysis with adjustment for age, sex, LV end-systolic dimension, LAVimax, and estimated SPAP, baseline LAGLS was identified as an independent predictor of cardiovascular events (adjusted HR, 0.91; 95% confidential interval [CI], 0.85–0.97; p=0.005) and re-hospitalization for cardiovascular causes (adjusted HR, 0.93; 95% CI, 0.86–1.00; p=0.039) (Table 3). Using the time-dependent ROC curve analysis, the optimal cutoff value of LAGLS for predicting adverse cardiovascular events at 5 years was 23.6% (AUC, 0.736; 95% CI, 0.63–0.84; p<0.001), with a sensitivity and specificity of 83.9% and 56.7%, respectively. The patients were divided into the high LAGLS (≥23.6%) and low LAGLS (<23.6%) groups based on the cutoff value. A comparison of the baseline characteristics between two groups is shown in Supplementary Table 2. Both groups were similar in terms of gender, prevalence of diabetes mellitus and hypertension, and operative characteristics. However, compared to the high LAGLS group, the low LAGLS group was older (54.9±11.6 years vs. 49.1±12.7 years, p<0.001), with increased LV end-systolic diameter and LAVimax, higher estimated SPAP and RA pressure, and higher prevalence of RV dysfunction. However, there were no significant differences in LVEF, MR severity, and concomitant other valvular regurgitation. The high LAGLS group had a significantly lower rate of adverse cardiovascular events (adjusted HR, 0.37; 95% CI, 0.14–0.96; p=0.041) than low LAGLS group (Figure 3 and Supplementary Table 3).
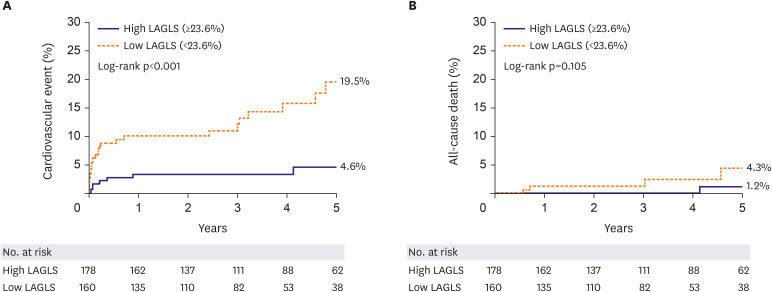
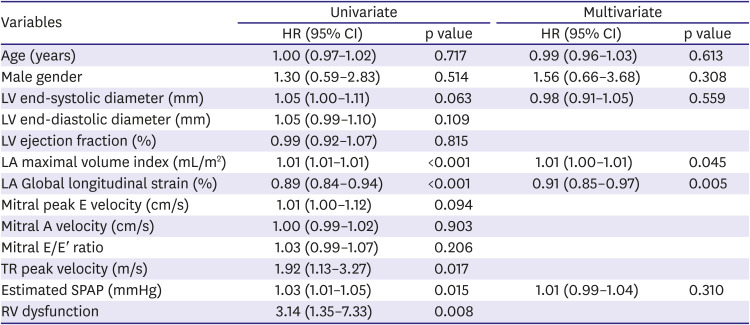
Figure 3
Comparison of outcomes between high and low baseline LAGLS groups. Cumulative incidence curves for cardiovascular events (A) and all-cause death (B) based on the optimal cutoff value of LAGLS (23.6%). High LAGLS: LAGLS ≥ 23.6%.
LAGLS = left atrial global longitudinal strain.
![]()
Table 3
Univariate and multivariable predictors of cardiovascular events after mitral valve repair surgery
CI = confidential interval; HR = hazard ratio; LA = left atrium; LV = left ventricle; RV = right ventricle; SPAP = systolic pulmonary artery pressure; TR = tricuspid regurgitation.
![]()
Subgroup analyses were performed with the adjustment of multiple variables which were identified as significant determinants for the primary outcome in the final multivariable model. Among the subgroup of patients with LAVimax ≥60 mL/m2, high LAGLS was associated with a significantly lower rate of adverse cardiovascular events (adjusted HR, 0.35; 95% CI, 0.14–0.92; p=0.033). Similarly, in patients with LAVimax <60 mL/m2, high LAGLS was associated with a significantly lower rate of adverse cardiovascular events (adjusted HR, 0.05; 95% CI, 0.00–0.69; p=0.026; Figure 4).
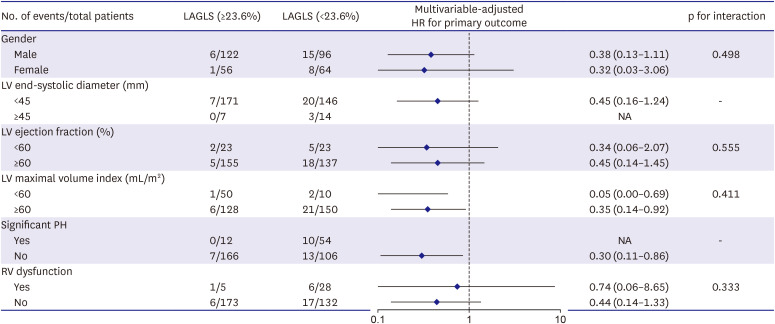
Figure 4
Subgroup analysis for cardiovascular events. HRs, adjusted by variables identified as significant determinants in the final multivariable model, are shown for the high LAGLS group in comparison with the low LAGLS group. HRs lower than 1 indicate a lower risk of cardiovascular events.
CV = cardiovascular; HR = hazard ratio; LA = left atrium; LAGLS = left atrial global longitudinal strain; LV = left ventricle; PH = pulmonary hypertension; RV = right ventricle.
![]()
DISCUSSION
The major finding of our study is that preoperative LAGLS is an independent predictor of postoperative adverse cardiovascular events in patients with chronic severe MR who underwent successful MV repair surgery. There was a significantly higher rate of adverse cardiovascular events in patients with a low preoperative LAGLS (<23.6%) than in those with high preoperative LAGLS (≥23.6%). Additionally, the long-term clinical outcomes were better with high LAGLS regardless of whether the patient had an LAVimax <60 mL/m2.
MV surgery is considered as a definitive treatment for patients with symptomatic severe MR. Current European guidelines recommend MV surgery for patients with overt symptoms, LV dilatation, LV systolic dysfunction, AF, or pulmonary hypertension. Significant LA dilatation (≥60 mL/m2) with a sinus rhythm has also been found to be a predictor of poor clinical outcomes in patients with asymptomatic severe MR and is considered one of the surgical indications.3) Increased LA size or volume is associated with adverse cardiovascular outcomes in both the general population and in patients with various cardiac diseases; thus, it is a powerful predictor of cardiovascular disease.22) However, increased LA volume itself cannot represent LA dysfunction, and normal LA function can be found even with enlarged LA, without an evidence of diastolic dysfunction.23) Recently, several studies have investigated the associations between LA volume, function, and clinical outcomes, and found that LA function reflected LA remodeling better than LA enlargement.24)25) Unlike LA volume, LA strain is an objective marker of LA function,26) and it represents the extent of myocardial fibrosis in the LA.8) The degree of LA fibrosis is a significant predictor of early and late LA reverse remodeling after MV surgery. In particular, LA longitudinal strain can detect subtle LA remodeling in the early stage, before structural changes, myocardial fibrosis, and chamber stiffness occur in the LA. Thus, the assessment of LA reservoir function is a more useful tool than LA volume for identifying patients whose outcomes may be improved with chronic severe MR surgery. Cameli et al.27) reported that decreased LAGLS (<35%) was a poor prognostic marker of adverse clinical events, including AF, stroke/transient ischemic attack, and cardiovascular death, in patients with moderate asymptomatic MR. In addition, Debonnaire et al.28) presented that patients with severe MR and decreased LAGLS (≤24.0%) had worse survival during follow-up, regardless of their symptom status. In our study, we show that low baseline LAGLS (<23.6%) is a poor prognostic marker of postoperative outcomes in chronic severe MR patients underwent MV repair surgery. Thus, the LAGLS may be a good marker for determining the optimal timing of MV surgery. Based on our findings, we propose that considering MV surgical correction before LAGLS decrease would be helpful in achieving good clinical outcomes even in patients without symptoms or a LAVimax <60 mL/m2.
In our study, compared to baseline values, LA dimensions and volume were significantly decreased after successful MR reduction; most of this reduction occurred during the early postoperative period, continuing over the 1-year postoperatively. On the other hand, the LAGLS decreased immediately after surgery, despite a significant decrease in LA volume. One year after MV repair surgery, the LA strain value improved compared to the immediately postoperative value, but did not fully recover and remained lower than the baseline LAGLS value. Decreased LA strain after surgery may be associated with reduced preload and decreased LA expansion due to MR correction; however, the possibility of LA function deterioration due to atriotomy after open surgery and manipulation of the LA cannot be ruled out. Mitral annuloplasty also had the potential to interfere with the basal movement of LA because the rigid complete ring directly fixes and stabilizes the mitral annulus. Patients without cardiovascular events had a smaller reduction in LA volume, but still maintained a high LAGLS after MV repair surgery, while patients with cardiovascular events had lower LA strain values despite a marked reduction in LA volume postoperatively. These findings suggest that low baseline LAGLS may be associated with increased LA stiffness and persistent LA dysfunction after MR repair surgery.
The present study has several limitations. First, there was heterogeneity in the baseline characteristics of the study population. To compensate for potential selection and baseline differences between study groups, covariate adjustment was performed. However, the results may still be biased by confounding variables that were not taken into account. Second, almost half of the screened patients were excluded due to AF. In patients with AF, LA strain was significantly lower than in non-AF patients even with the same MR severity. Therefore, AF patients were excluded to investigate the impact of LA strain affected by chronic volume overload caused by severe MR rather than AF on postoperative clinical outcomes. It is unclear whether the study results can be applied to patients with functional MR. Furthermore, in this present study, preoperatively LVGLS could not be assessed. Therefore, important additional factor, LVGLS, was not comprehensively integrated into this risk model. Third, in this study, we set the primary endpoint as a composite outcome, a cardiovascular event, because the event rate of each individual outcome was small. Cardiovascular events consisted of individual outcomes that were either already included in previous studies of valve disease or occurred frequently in MR patients. Finally, although our findings suggest an additional clinical role of LAGLS assessment in determining the optimal timing for surgery in patients with chronic severe MR, the study was single-center in nature, with a small registry; thus, a clinically directive conclusion is not feasible. The overall findings should be confirmed through a further large-scale clinical investigation.
In patients with chronic severe MR, preoperative LAGLS is an independent predictor of postoperative outcomes after MV repair surgery. Patients with high preoperative LAGLS had better long-term outcomes compared to those with low preoperative LAGLS, regardless of a LAVimax <60 mL/m2. Therefore, the evaluation of preoperative LAGLS can be used to predict postoperative outcomes and determine the optimal timing for MV surgery.
 XML Download
XML Download