

 PDF
PDF Citation
Citation Print
Print



A 57-year-old man was admitted for cardiac sarcoidosis work-up. He had been suffering from dermal sarcoidosis in both his lower legs for 7 years. He denied symptom of chest pain. Transthoracic echocardiography revealed akinesia and a focal aneurysm at the left ventricular (LV) apex (Figure 1A and B, Supplementary Video 1). Coronary angiography and coronary computed tomography revealed dual left anterior descending artery (LAD) type 41); a short LAD from the left main coronary artery (Figure 2B) and a long LAD of anomalous origin from the right coronary sinus with mild compression by right ventricular outflow tract (Figure 2A and B). Cardiac magnetic resonance imaging (CMR) revealed an aneurysmal change and transmural late-gadolinium enhancement (LGE) at the LV apex, and subendocardial LGE of anterior and lateral walls (Figure 3) which were not compatible with typical cardiac sarcoidosis because of aneurysmal change of LV apex and subendocardial involvement.2) On a resting F-18fluorodeoxyglucose positron emission tomography (FDG-PET) scan, there was high uptake at the LV apex, including the lateral and anterior walls (Figure 4), indicative of cardiac sarcoidosis.3) It is assumed that myocardial necrosis due to granulomatous inflammation induced LV apical aneurysm in this patient.4)
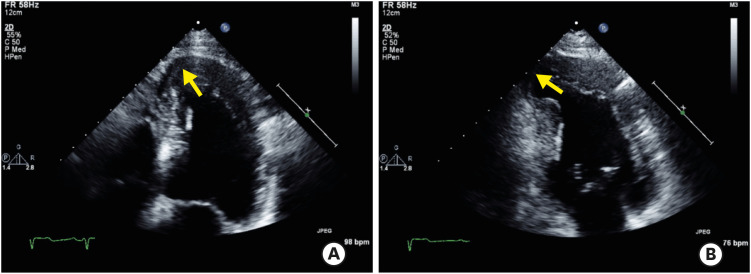
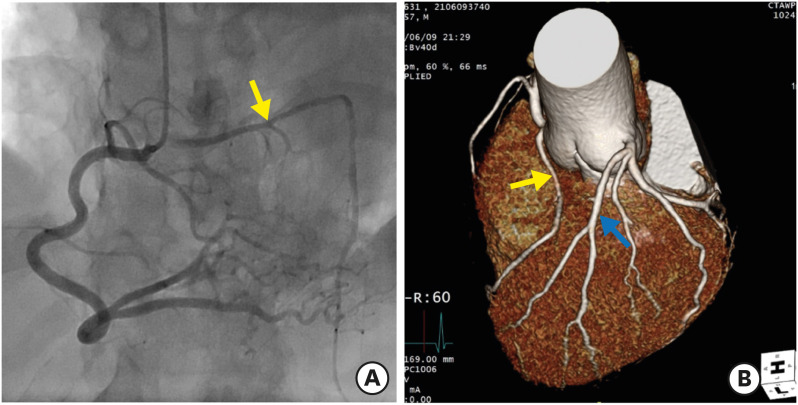
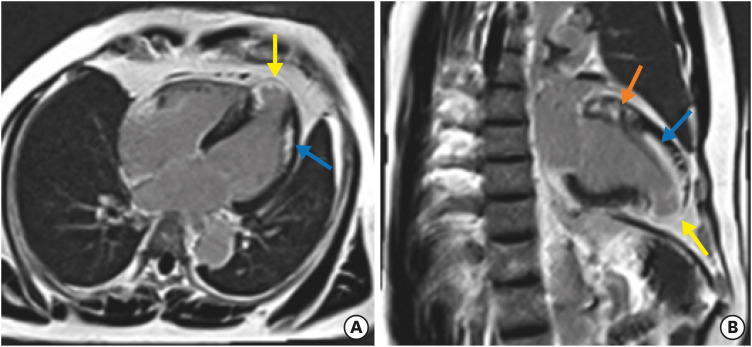
Figure 1
Apical 4-chamber (A) and 2-chamber view (B) revealing akinesia and a focal aneurysm at the left ventricular apex (yellow arrows).
![]()
Figure 2
Coronary angiography (A) and coronary computed tomography (B) revealing dual LAD type 4; the long LAD of anomalous origin from the right coronary sinus with mild compression by right ventricular outflow tract (yellow arrows) and the short LAD from the left main coronary artery (blue arrow).
LAD = left anterior descending artery.
![]()
Figure 3
Horizontal (A) and vertical long axis view (B) of cardiac magnetic resonance imaging revealing wall thinning with aneurysmal change and transmural LGE of the LV apex (yellow arrows), subendocardial LGE of the anterior and lateral walls (blue arrows), and intramural patchy LGE of the LV base (orange arrow).
LGE = late-gadolinium enhancement, LV = left ventricle.
![]()
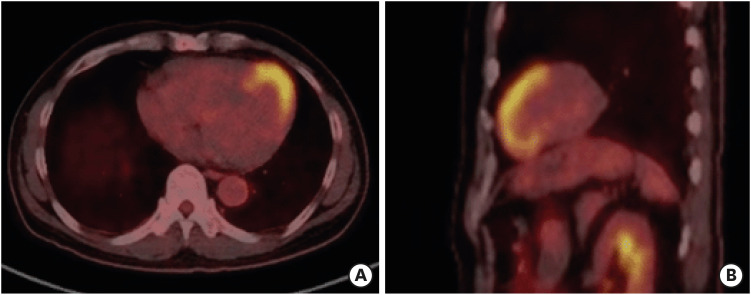
This case reflects the importance of screening for cardiac sarcoidosis in patients with extracardiac sarcoidosis.5) Although the findings of CMR in this case are not typical of cardiac sarcoidosis, in a case with past history of extracardiac sarcoidosis, they should be regarded as diagnostic clues for cardiac sarcoidosis. Such a situation warrants further imaging assessments, such as an FDG-PET scan.3)
The Institutional Review Board (IRB) of Ulsan University Hospital approved this study and the patient's informed consent was waived (IRB number: UUH202108038-HE003).
 XML Download
XML Download