

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Blood pressure (BP) measurement (BPM) is an essential part of medical examination, and undisputedly, the accuracy of BPM devices is crucial.1) The technique of BPM remained mostly unchanged during the last decades. Despite technical progress in automated cuff-based BPM devices, BPM is still based on a cuff and sphygmomanometer’s principles described by Riva Rocci and Korotkoff.2)
There is no doubt that cuff-based BPM has several problems, including the requirement for specific devices and limitations for 24-hour BP monitoring, including patients’ discomfort, which influence BP acutely.2)3) Therefore, extensive efforts have been made to develop cuffless BPM devices using pulse-transit-time or photoplethysmographic (PPG) signals. The advance of information and communication technology and the widespread mobile smartphone devices and smartwatches have brought new BPM possibilities using PPG signals. In April 2020, the BPM application (App) based on PPG signals available for the Samsung Galaxy Watch 2 (GW2) was the first one ever to be approved as a medical device by a government (Korean Ministry of Drug and Food Safety).4)5) A second device sold as a clinically validated BPM device is the Aktiia bracelet promising 24/7 BP monitoring. As a result, physicians are likely to be confronted with this new technology. Therefore, it will be of paramount importance for clinicians how the data patients retrieved by PPG devices should inform our clinical decision-making while keeping a patient-centered approach and yet evidence-based medicine.
Go to : 
VALIDATED PPG APPS AND DEVICES?
A prerequisite of BPM is the accuracy of the measuring device. According to current hypertension guidelines, clinicians and patients should only use BPM devices validated according to standardized protocols.3) However, even standard cuff-based BPM devices have often not been validated correctly, as reported by STRIDE BP, an international initiative for accurate BPM.1) As example in a recent study in Australia non-validated home BPM devices dominated the online marketplace resulting in roughly 18% of upper arm cuff devices (51 out of 278), 8% of wrist cuff devices (13 out of 162) and 0% of wristband wearable devices (0 out of 532) proven accurate according to international validation standards.6)
Therefore, examining the PPG Apps and devices available to date, none currently comply with the above-mentioned validation requirements. Additionally, there are presently no cuffless PPG devices officially recommended by STRIDE BP for home BPM, which is essential for hypertension diagnosis and management. Nonetheless, recent studies have shown improved accuracy by using ubiquitous or linear polynomial equations.7)8) For example, a proof-of-concept study applying an iPhone camera sensor for BPM showed bias and precision errors of −4.0 and 11.4 mmHg for systolic blood pressure and −9.4 and 9.7 mmHg for diastolic blood pressure.9) Furthermore, a smartphone-based BPM algorithm using transdermal optical imaging technology in normotensive adults falls within 5±8 mmHg of reference measurements, which fulfills a critical accuracy threshold bias and standard deviation (SD) according to the Association for the Advancement of Medical Instrumentation (AAMI) validation standard.10) The Samsung GW2 is reported by the manufacturer and the Korean Ministry of Drug and Food Safety to meet performance standards for automatic cuff-based electronic BPM devices with an average difference of less than ±5 mmHg and a maximum SD of 8 mmHg. However, there is a lack of detailed information peer-reviewed or published regarding the study population, methods, and spread of the BP data, including the measurement process during the study.4) The new Aktiia bracelet is sold as an easy 24/7 BP monitoring device which consists of a bracelet with an optical measurement unit. It can be connected to a smartphone App using Bluetooth to retrieve the BPM values. The bracelet device comes with an upper arm cuff-based automated BP device to perform a calibration measurement on the contralateral arm. In a comparative study using an adapted ISO81060-2:2013 protocol including 86 participants, the device showed promising results resulting in mean (and SD) differences between the bracelet and the reference of 0.46±7.75 mmHg for systolic and 0.39±6.86 mmHg for diastolic BP values. Both validation criteria of the ISO81060-2:2013 protocol have been fulfilled, with the caveat that the ISO81060-2 protocol was established for non-invasive sphygmomanometers and not for cuffless PPG BPM. Furthermore, there have been several protocol deviations within the study—including underrepresentation of systolic blood pressure >140 mmHg, which are of special interest in terms of diagnosis and treatment of arterial hypertension.11)12)
However, numerous Apps did not pass clinical validation. The most prominent example being the Instant BP Smartphone App, one of the top 50 best-selling iPhone Apps in 2014/2015. After an independent study, it had to be withdrawn from the market, showing a considerable overestimation of low BP values and underestimation of high BP values compared to standard BPM.13) This pattern was repeatedly seen in studies comparing PPG Apps to standard BPM. Therefore, it is crucial to know about the BP distribution and the graphical presentation in a validation study.13)14)15)
Go to :
ARE PRESENT VALIDATION PROTOCOLS ADEQUATE FOR PPG DEVICES?
Over the last decades, several academic societies and industry standards have used various validation protocols until the proposal for a universal standard for the validation of BPM devices was finally adopted by the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO) in 2019.16) This is a highly standardized and reproducible validation protocol based on decades of experience in validating cuff-based BPM devices.16) In brief, at least 85 participants were tested under static conditions, comparing same arm, sequential measurements of a test device to the reference method using a mercury sphygmomanometer and auscultation by 2 observers. It starts with 2 initial measurements (reference and test) and 7 alternating validation measurements starting with the reference BP (Figure 1). Participants with BP difference above 12 mmHg systolic or 8 mmHg diastolic between any 2 reference BPs need to be excluded, resulting in very stable BP condition during the time needed for measurements. Next, results were analyzed according to specific validation criteria.16) However, for PPG Apps or alternative continuous cuff-less devices,16) there is no generally accepted validation protocol to date. This is highlighted in the consensus document by the AAMI/ESH/ISO, and task groups have been established to explore the methodology of such protocols.16)17) The Institute of Electrical and Electronics Engineers (IEEE) published a standard in 2014 (IEEE1708-2014), but this was criticized for having the major limitation that the reference measurement method was not described detailed enough to ensure standardization—usually a key feature of validation protocols.18)19) Additionally, there is an ISO 81060-3 standard for the clinical investigation of continuous non-invasive automated BPM devices under development. Still, as long as it is not completed and fully implemented, new devices will come up with different adaptions of validation protocols like the Aktiia device.11)
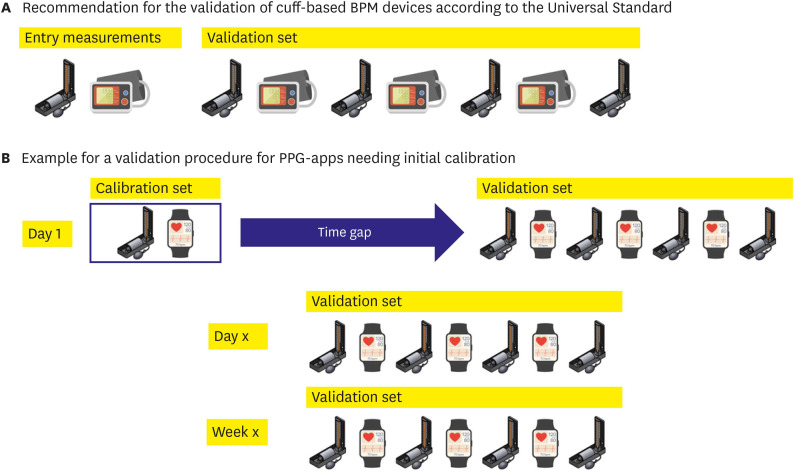 | Figure 1Measurement sequences for the validation of BPM devices. (A) Measurement sequence according to the Universal AAMI/ESH/ISO Standard for the validation16) of cuff-based BP measurement devices, started by entry measurements with the reference method and the test device, directly followed by the validation measurement set. (B) The proposal for a validation procedure for PPG Apps needs an initial calibration to the reference method. After a first calibration set, validations are set at different time points covering one calibration’s recommended time frame.Source of illustrations: Shutterstock.com (Zern Liew; marina_ua; Victor Metelskiy).
AAMI/ESH/ISO = Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization; App = application; BP = blood pressure; BPM = blood pressure measurement; PPG = photoplethysmographic.
|
From a clinical point of view, there are 2 major types of PPG Apps. One type is Apps which measure BP directly, e.g., the Instant BP Smartphone App. In these cases, a validation protocol like the 2019 AAMI/ESH/ISO Standard may be suitable for validation as 2 independent measurements are compared. But the other type is Apps which need calibration to a cuff-based BPM before use, like the Samsung GW2 or the Aktiia bracelet. Afterward, BP values are estimated based on this calibration. This may lead to bias and raise critical questions about the methodology of traditional validation protocols. When the first App measurement is calibrated to the first reference measurement, the validation measurement set is directly following this calibration. Then, how can we extrapolate that this App can truly monitor dynamic changes in BP? It would be sufficient for passing the validation if the App covers a small range of BP changes around the calibration measurement. For the Samsung GW2 and the Aktiia bracelet, recalibration is recommended every 4 weeks, but how can we rely on BP values over 4 weeks after the initial validation study covering 20 minutes after calibration? At least the study team had to use several time points when investigating the device’s accuracy.11)
Given these limitations, a unique validation protocol has to be tailored, covering the first set of validation measurements and repeated measurements allowing for BP changes after different periods of time. The last set of measurements then would be mandatory before recalibration is recommended by the manufacturer. An example of such a protocol in comparison to a traditional validation protocol is given in the Figure 1.
Additionally, before applying a new technology, different patient groups that represent the general population have to be studied, e.g., subjects with large visit-to-visit BP variability or taking different drugs influencing vascular tone to challenge the new techniques in a clinical context. Moreover, there is a need for validation in special populations like the elderly, patients with cardiovascular disease, children, adolescents, or pregnancy.
Go to :
PITFALLS FOR DAILY CLINICAL PRACTICE USE
There are several questions regarding the implementation into clinical practice. Correct BPM is not an easy task. BPM should be done according to standard operating procedures recommended by professional societies, including resting time, sitting position, quiet surroundings, validation and regular recalibration of devices.3) For PPG Apps needing calibration, accurate calibration will be mandatory for the accuracy. Errors during the calibration process may translate into deviations afterward. So, who will execute this calibration? Patients at home with their own devices, as we know that the majority of BP monitors on the market are not clinically validated? Or doctors in a clinical setting which might not be feasible for the younger population, current main users of PPG Apps?1) Given the enormous importance of accurate calibration, this question is essential.
The next question is how to interpret the large amount of BP values collected by the patients. The devices allow BPM at 7 days per week and even over 24 hours or collect BPM according to device-specific timings for some devices. We can assume that people will track their BP on a 24/7 basis (as the PPG App is included in a smartwatch that they wear) and bring their results into the clinics. This might be an enormous advantage, e.g., for symptom-BP correlation in case of dizziness or evaluation of nighttime BP or BP fluctuation. But actually, there is a need for studies comparing these values to our traditional cut-off BP values for home-based BPMs, which usually follow a specific protocol of a given number of BPMs in the morning and evening hours.3)20) Therefore, we will need more experience and comparative studies in the areas intended for their use, e.g., in comparison to traditional home and ambulatory BP monitoring. As an example to illustrate this challenge, the Somnotouch Non-invasive BP Measurement device is a cuff-less beat-to-beat BPM device developed explicitly for ambulatory BP monitoring. The device uses changes in the pulse-transit-time after an initial cuff-based calibration to estimate changes in BP. It has passed a validation study according to the European Society of Hypertension International Protocol revision 2010 for the validation of BP monitoring devices.21) Still, it leads to significantly higher mean systolic and diastolic BP values when compared to standard cuff-based devices over 24 hours.22)23) Reasons for that phenomenon remain unclear and include a systematic error in the algorithm, possible deviations due to a larger number of BPM, more values during physical activity by the cuffless device, and an inability to reflect pronounced BP changes, postural changes, changes in vascular tone, or hemodynamics over time.22) The technique used was not PPG, but the example illustrates that a positive validation study under laboratory conditions doesn’t predict necessarily that BP values obtained by the device are interchangeable with traditional BP measurements in the designated area of use—which is 24 hour BP measurement for the Somnotouch device. From this example we can learn, that there has to be a thorough evaluation of PPG measurements under different physiological conditions, too.
However, BPM by PPG Apps opens a new field of dynamic BP evaluation in a real-life setting. Although BP values in ‘resting condition’ are still the most critical factors determining prognosis, BP variability has been proven in many studies to be an independent and robust indicator of cardiovascular events.24) Nevertheless, conventional BPM, including ambulatory BP monitoring, mainly focused on the static BP values at resting status. PPG App-based BPM will report BP changes in daily living and during physical/emotional stress, thus opening new chapters of BP research regarding dynamic BP evaluation, e.g., response to intrinsic and extrinsic environmental factors like stress at work or seasonal climate changes. Current PPG Apps cannot measure BP in actual dynamic conditions but require a resting status for 60 seconds to get valid signals. In the user manual of the Aktiaa bracelet, e.g., the manufacturer of the device states that the BPM is done during periods of rest. However, the rapid progress of PPG technology will result in beat-to-beat signal processing.
Last but not least, one additional and important advantage has to be addressed. This technology may have the additional benefit of increasing BP awareness in the young. Currently, target customers for BPM Apps are the younger rather than the elderly. Although hypertension prevalence is low in those in the 3rd to 4th decade of life, they showed a low rate of awareness in hypertension.25)26) With a PPG App in their smartwatch, people need to measure BP using standard devices only every 4 weeks for re-calibration. For the remainder of the time, the smartwatch will track and report BP values automatically.
In conclusion, the possibilities of PPG Apps for BPM are vast and fascinating and can hopefully be integrated into clinical and research practice soon. It will open up new screening methods and monitoring possibilities in different environments. There is the possibility that BPM will be widely and readily available to people, especially for tracking over extended periods. Nonetheless, there is still no validated BPM App that is recommended by professional societies to date. Critical questions remain in PPG Apps that need calibration to a standard BPM. This includes developing specific validation protocols, execution, and publication of validation studies adhering to these protocols, and evaluation of the devices in different patient groups.
Go to :
 XML Download
XML Download