

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pulmonary hypertension (PH) is a devastating disease with multifactorial causes. Various etiologies affect pulmonary vascular resistance, and increasing resistance leads to right heart failure. PH is classified into five subtypes in accordance with the hemodynamic features affecting pathophysiology.1) Worldwide, based on the global prevalence, all PH cases affect approximately 70 million people.2)3) Promising therapies are available for pulmonary arterial hypertension (PAH) belonging to group 1 PH and address therapeutic targets by focusing on their cellular and molecular mechanisms. In terms of the pathophysiological characteristics, endothelial cell (EC) dysfunction, fibroblast and smooth muscle cell (SMC) proliferation, pericyte communication and detrimental changes in ECs to mesenchymal cells occur.4) These conditions clinically result in narrowing of the endovascular diameter, inflammation, and thrombosis. The leading determinants of pulmonary vascular remodeling are interactions between cellular instigators such as pulmonary ECs, pulmonary arterial SMCs, various immune cells and molecular recruiting mediators such as cytokines and paracrine products.5)6)7) These pathobiological reactions exacerbate patients’ hemodynamic statuses and cause right heart failure, resulting in multiorgan damage and ultimately death.8)9) A growing body of research suggests that pulmonary vascular inflammation induced by multiple immune cell interactions is crucially linked to the development of progressive vascular remodeling in PAH.
Currently approved conventional treatments for PAH can control symptoms or ameliorate worsening conditions, but are not curative or preventive.10)11) Therefore, many researchers are eager to discover novel treatments from the aforementioned pathological point of view.12) For example, by focusing on inflammatory reactions, which are the main mechanisms of pulmonary vascular remodeling, anti-inflammatory remedies have an anti-remodeling role and modulate vascular tone, preventing vascular fibrosis.13) Macrophages are one of the main actors inducing inflammation-related mediator cascades, and a treatment targeting monocytes, the precursors of these macrophages, and monocyte progenitors might be able to control pulmonary vascular remodeling.14)15) In addition, in these situations, pulmonary ECs and pulmonary arterial SMCs communicate, leading to remodeling of pulmonary vascularature called “plexiform”. Due to dysfunction of ECs and excessive proliferation of SMCs, pulmonary blood vessels are muscularized, resulting in decreased vascular compliance, narrowing of the internal diameter, and increased pulmonary vascular resistance. Through concepts focusing on genetic insights as well as cellular and molecular perspectives, a new therapeutic approach is being explored by pathological investigation. The expression of related genes, transcription components, and epigenetic compounds has been reported.16) Herein, in this review, with the development of various technical studies and improvements in awareness of related paradigms, as a novel treatment field for PAH thus far, regenerative therapies with stem cells and their paracrine effects are summarized, and future prospects are presented.
CELL THERAPY in PULMONARY HYPERTENSION
Stem cell based remedies
Stem cells refer to cells that have not yet differentiated in humans; that is, they possess the potential capability to differentiate into any type of cell. Two main methods for transplanting stem cells have been applied. One method involves transplanting appropriate stem cells directly into a target site in the body, where the essential niche and specific signaling molecules help the stem cells differentiate into the intended cells, thereby exhibiting substantial actions. With the other method, under in vitro circumstances, definitive types of stem cells are isolated, cultivated, and induced to differentiate into cells with substantial actions, and these stem cell-derived mature cells are transplanted into the patient. With these two methods properly combined and applied to the patient, a good therapeutic effect can be achieved.
Stem cells are able to differentiate into vascular cell lineages that can be effective for the regenerative process and treatment of PH.17) One of the mainstream cell-based therapies is mesenchymal stem cells (MSCs), which are derived from mesoderm in the early developmental phase. They can renew themselves and possess the potential capability to differentiate into many cell types. MSCs, which were first found in bone marrow, can be isolated not only from bone marrow but also from adipose tissue, umbilical cord blood, peripheral blood and other tissues.18) Depending on the specific circumstances, MSCs are capable of diverse differentiation into bone, cartilage, nerves, adipose tissue, liver, myocardium, muscle, tendon, ligament, or ECs in both laboratory and in vivo environments.19)20)21) As such, the virtues of MSCs are that they can be collected from various tissues relatively easily and can be differentiated in various manners by their pluripotent factors. Various signals and products from MSCs have therapeutic actions with respect to senescence and advanced diseases.
Although the definition of human MSCs has been newly revised in the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy, separate MSCs from various sources typically express similar cell surface tracers and differentiate by recognized lineage pathways but are distinguished by gene expression, lineage differentiation, and immunological characteristics.22) As an excellent cell source for lung tissue regeneration treatment through differentiation possibilities and accessibility, MSCs have an anti-inflammatory effect along with immunological interactions. However, if applied to the real clinical field, cell-based treatment using MSCs has many hurdles to overcome in many areas.23) For example, MSCs derived from bone marrow have limitations in their ability to proliferate and can show significant differences in cell quality because they are obtained from several different donors. In addition, in ex-vivo environments, cells quickly lose their potential for differentiation and protection, and depending on the donor's condition, bone marrow MSCs obtained from an old or sick donor may be fatally impaired in their viability and function as stem cells.24) Although these challenges exist, recent attempts have been made to find complementary measures and apply them to PAH. Since PAH shows reduced resident MSCs in the lung, administration of differentiated lung MSCs can slow PAH progression.25) Accordingly, researchers studying treatment using stem cells for lung disease have considered that treatment applying other tissues or other stem cell types is limited. Meanwhile, a proposal for pericytes from the lungs as cells with the potential for differentiation has also been suggested. Bordenave et al. demonstrated that pulmonary pericytes, a kind of progenitor cell in residency, more often differentiate into SMCs and induce pulmonary vessels to undergo muscularization under exposure to hypoxic conditions.26)
The next proposed agent for cell-based therapy is induced pluripotent stem cells (iPSCs). iPSCs were spotted in 2006 by 2 Japanese scientists and were created by reversely differentiating somatic cells by transfection with exogenous specific genes.27) In cell-based treatment, human iPSCs are desirable because they possess the potential capability to differentiate into all types of cells in the human body, such as embryonic stem cells (ESCs).28) Ethical difficulties and immune rejections, which are serious problems that can be encountered in other MSCs, are overcome by autologous human iPSCs. The first patient in the world in whom autologous human iPSCs were transplanted was a Japanese patient diagnosed with polypoidal choroidal vasculopathy in 2014.29)
MSCs, iPSCs, human amniotic epithelial cells, and endothelial progenitor cells are stem cell-based treatments, that are applied to associated lung diseases and experimental PH models that can cause right ventricular failure, suggesting the possibility of cure by preventing disease progression and reversibility to the normal state. Their anti-inflammatory and protective properties and ability to recover normally play a decisive role. Herein, we applied cell-based treatment to clinical disease and an experimental PH model.
Stem cell-based remedies in pulmonary hypertension: using mesenchymal stem cells
Through several preclinical experimental studies, remedies with MSCs that have the potential to control immunological inflammation ameliorate diseases such as acute lung damage, chronic obstructive pulmonary disease, pulmonary fibrosis, and asthma.30)31) In a hypoxic model, we performed comparative and systemic analyses of treatment using MSCs in a monocrotaline (MCT) rat model. In this study, MSCs were derived from three sources: bone marrow, adipose tissue, and umbilical cord blood. All of these MSCs demonstrated therapeutic effectiveness and feasibility. Among them, MSCs separated from umbilical cord blood were found to have superior effects in terms of improving right ventricular function, pathological changes, cell engraftment, anti-inflammatory aspects.32) These stem cells regulate the immune/inflammatory response in the MCT model, thereby improving the environment (niche) in which stem cells live and increasing the survival rate of stem cells. Stem cells with an increased survival rate persist for a long time to exert their function, alleviate the inflammatory response, attenuate vascular remodeling in the PH model, and improve hemodynamic function.
Stem cell-based remedies in pulmonary hypertension: using induced pluripotent stem cells
iPSCs, which are dedifferentiated cells from adult somatic cells that genetically reprogram through exogenous transcription factors, have pluripotency, such as ESCs. One study showed therapeutic results by applying iPSCs using a rat MCT model.33) In this MCT-induced PAH model, treatment using iPSCs improved right heart dysfunction, resulting in a decrease in hemodynamic parameters supporting right ventricular systolic pressure. In addition, histologically, such treatment prevented deterioration of the vascular remodeling of the pulmonary arterioles and suppressed the proliferation of the media layer by blocking inflammation. Therefore, iPSC-based treatments present powerful evidence for ameliorating vascular remodeling and repairing damage in PAH and lead to the recovery of vascular endothelial integrity. In a recent study, in familial PAH associated with the bone-morphogenetic-protein-receptor 2 (BMPR2) gene, human iPSC-derived ECs from carriers were applied to identify genetic variations between patients and controls.34) The investigation revealed that carriers human iPSC-derived ECs present a boost in BMPR2 activators and a decrease in BMPR2 inhibitors. These results demonstrated that many ECs are preserved and alive in unaffected carriers. However, although these promising projects have been performed at the preclinical stage, more studies should be conducted to optimize clinical applications in patients in terms of cost-effectiveness and tumorigenic activity.
FREE FROM CELL THERAPY IN PH
Extracellular product-based remedies in pulmonary hypertension: using exosomes
The above description referred to cell-based treatment using stem cells, and the proceeding description refers to extracellular products, not the cell itself. Free-from-cell treatment refers to dealing with materials and products derived from activated cells and the interface of communication between cells. One of the major mechanisms leading to pulmonary vascular remodeling at the molecular level is the inflammatory reaction, which is responsible for dysfunction of the immune system. Dysregulated immune cells recruit many mediators that lead to a cascade detrimental immune responses. The transporters in these processes are extracellular vesicles (EVs).
Exosomes, which are EVs, are smaller than microvesicles and have a diameter of approximately 30–150 nm.35) When a cell is stimulated by diverse factors, the plasma membrane sprouts inward to generate early endosomes. Through endosomal production, multivesicular bodies (MVBs), which have roles as transporters, were induced and maintained to pool intraluminal vesicles. MVBs adapt their constituents according to physiological or morbid changes in cell status. The degradation process is also possible by trafficking lysosomal MVBs themselves, and MVBs also release their accumulated intraluminal vesicles into the extracellular gap. These intraluminal vesicles contain some functional cytosolic requisites, such as messenger RNA (mRNA), microRNA (miRNA), and other transmembrane proteins. Exosomes are these secreted intraluminal vesicles.36)
In the extracellular space, the released vesicles act as messengers between cells. Exceptionally, exosomes play pivotal roles in the remodeling process of pathological vascular diseases and play a central role in therapeutic approaches in the clinical field. An increasing number of studies are being published on therapeutic and prognostic applications of exosomes in vascular diseases including PH. Therefore, we discuss current knowledge about exosome therapy in a general spectrum of PH in this section.
As the physiological cellular mechanism of vascular remodeling proceeds, exosomes act as key players in communication and signaling in the cellular interspace. Exosomes and several other EVs are produced through unusual pathways other than the basic secretory routes identified theoretically thus far.37) To regenerate damaged pulmonary vasculature, the conventional pathways of released secretory proteins that act on such vessels and the context of using unconventional pathways must be understood. To establish the role of exosomes in vivo and to apply them therapeutically, understanding the specific signaling cascade that exosomes utilize is essential. In pulmonary vascular remodeling, dysregulated immunity is exhibited, and various mediators accumulate. Exosomes have been pivotal as immunomodulators in intercellular communication and antigen presentation that induce immunological responses. This role contributes to providing cargo that transports mRNAs and miRNAs contained therein and shuttles proteins. In addition, although their role has not yet been fully elucidated, according to recent studies, exosomes appear to be critical regulators in the inflammatory reaction, which is one of the mechanisms causing deterioration of vascular diseases. Contrary to concerns about the irrelevant proliferative potential of treatment with stem cells, therapies with exosomes as powerful emerging curative solutions for many diseases, including PH, have the advantage that a large amount can be directly applied to damaged tissues.
Mesenchymal stem cell environment
MSCs, as previously discussed, are pluripotent cells that are relatively easily obtained from diverse tissues, such as bone marrow, dental pulp, adipose tissue, the placenta, and umbilical cord blood. MSCs can be differentiated into various cells under specific circumstances. In the therapeutic approach to cardiac diseases, MSCs have been frequently discussed and applied in various ways. Using their anti-inflammatory and regenerative potential, MSCs and products derived from MSCs can be exploited for therapeutic sources. Many reports have revealed that the therapeutic ability of MSCs utilizes MSC derived medium, and the exosomes therein are the major instruments for treatment. In a porcine myocardial ischemic/reperfusion model, the therapeutic effect of MSCs and products derived from MSCs involve significant reduction of the extent of damaged myocardium.38) In addition, when exosomes from MSCs (MSCs-exo) were applied to a mouse myocardial infarction model, a protective effect was revealed.39) In terms of the niche of MSCs, MSCs obtained from the umbilical cord are superior in some reports is because they can be isolated in a noninvasive manner and proliferate to show appropriate immunological modulatory capacities.40) However, other hypotheses have been proposed, and the therapeutic effects of MSCs-exo from various tissues, including the endometrium, human bone marrow, and adipose tissues, have been analyzed and compared in a myocardial infarction rat model.41) Depending on the derivation of the MSCs from which the exosomes are obtained, studies on the superiority of the therapeutic effects should be further investigated.
The hypoxic environment is one of the major triggering factors of PH. One study demonstrated that MSCs-exo modulate and prevent the remodeling process of pulmonary vasculature in a hypoxic environment by contributing to detrimental responses in PH.42) Many trials have proposed that MSCs-exo take hold therapeutic options. One recent study showed that MSCs-exo significantly suppressed apoptosis of hypoxia-induced pulmonary ECs and proliferation of pulmonary arterial SMCs in vitro. MSCs-exo also effectively decreased right ventricular hypertrophy and suppressed the remodelling process of pulmonary vascularature in an MCT PH rat model. This study clearly indicated the beneficial effects of MSCs-exo in PH and showed that the curative influence of MSCs-exo is mediated by Wnt5a.43) In addition, favorable therapeutic applications for MSCs-exo have been revealed in a hypoxic PH mouse model. MSCs-exo improve the exacerbated right ventricle and PH by inhibiting signal-transducer-and-activator-of-transcription 3.44)
Induced pluripotent stem cells environment
iPSCs are able to differentiate and multiply into any cell type in vivo, irrespective of where they originate, such as ESCs. Researchers have reported that exosomes from ESCs promote the recovery of damaged myocardium and ameliorate cardiac function after immediate myocardial infarction.45) Many studies on the therapeutic effects of exosomes from iPSCs (iPSCs-exo) and iPSC-derived products have been conducted. Several reports have demonstrated that iPSCs-exo propel injured tissues toward repair and lower fibrotic changes, have protective and preventive effects, and enhance the regenerative ability of ischemic tissues. Moreover, microvesicles obtained from iPSCs are feasible prospective therapeutic vectors that support the differentiation of cardiac-derived MSCs into cardiac ECs.46)
Recently, several studies have shown that the bioactive molecules carried by EVs generated from iPSC- derivatives have significant therapeutic effects in myocardial infarction.47) Researchers found that EVs generated from iPSC-derived cardiomyocytes (iCMs) enriched mitochondria (M-EVs). The data revealed that M-EVs-derived mitochondria were transfused into recipient iCMs, significantly recovered intracellular adenosine triphosphate production and ameliorated the contractility of hypoxia-injured iCMs in vitro. Significant cardiac function improvement was also found when M-EVs were administered intramyocardially after blocking left anterior descending coronary artery flow through the redistribution of bioenergetics and mitochondrial biogenesis.48) Another study showed that specific microRNA cluster-enriched EVs derived from hypoxia-injured iCMs have therapeutic effects on oxidative stress and restored cardiac function after ischemic injury by targeting the Notch3 signaling pathway.49) These studies indicate the possibility of developing novel treatments for cardiac diseases, including heart failure, by using EVs derived from iPSCs and their derivatives. They suggested that iPSC-derived exosomes may treat degenerative diseases through endogenous repair.
FUTURE DIRECTION TO CONQUER DISEASE
The development of innovative therapies using stem cells opens new horizons for PAH treatment, but some hurdles to clinical application remain. These hurdles include difficulties in technical steps. To describe the steps, stem cells/exosomes are isolated consistently, survive viably, are properly delivered to the targeted destination, and engraft well. For example, in one preclinical attempt to improve the therapeutic potential for myocardial regeneration, EVs were applied using nanoparticles to address the engraftment and stability of exosomes derived from MSCs.50) In addition, disease model research reported that nanoparticles delivered via the intravascular space play a therapeutic role to improve pulmonary angiogenesis and block PH progression.44)
CONCLUSIONS
Although therapeutic options are being applied using various channels with the development of targeted drugs, PAH is still a fatal progressive disease. Targeted therapies, which have been used in PAH patients in various manners thus far, are based on the following mechanisms: prostacyclin, nitric oxide, and endothelin pathways. The recent approval of all drugs based on the above mechanisms had facilitated restoration of vascular EC function and inhibition of obstructive progressive changes by regulating vascular activities and vasoactive mediators that cause pulmonary vascular remodeling, which has led to an improvement in the survival rate of PAH, thus benefitting patients' quality of life, and slowed progression of the disease over the past two decades, but PAH is still difficult to completely cure. Therefore, a promising treatment strategy is urgently needed. As awareness of and pathophysiological insight into the disease expand and technical research and academic attempts are executed, researchers are proposing robust and novel strategies to improve treatment performance in the current challenging conditions. The therapeutic field involving cell-based therapies and cell-free therapies using small molecules has shown promising results for PAH treatment in preclinical studies (Tables 1 and 2). More solid and optimal achievements should be supported for the clinical application of those therapies. In ongoing preclinical investigations, cell therapies have been demonstrated to be effective through hypothesis testing and are awaiting development as commercial items in clinical practice.
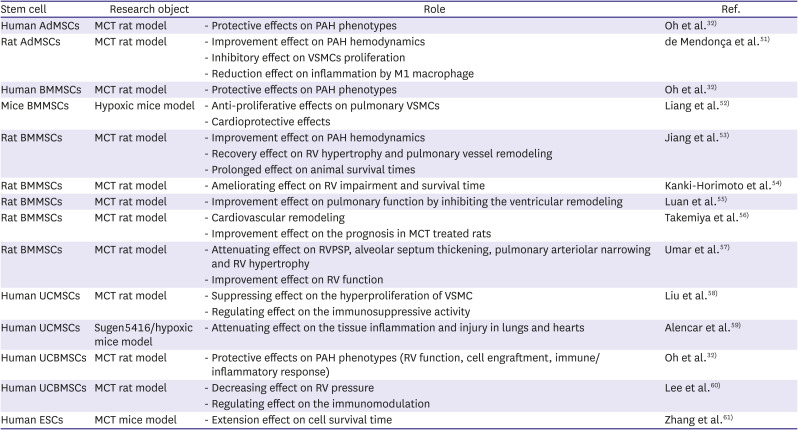
Table 1
Therapeutic role of stem cells in pulmonary arterial hypertension
| Stem cell | Research object | Role | Ref. |
|---|---|---|---|
| Human AdMSCs | MCT rat model | - Protective effects on PAH phenotypes | Oh et al.32) |
| Rat AdMSCs | MCT rat model | - Improvement effect on PAH hemodynamics | de Mendonça et al.51) |
| - Inhibitory effect on VSMCs proliferation | |||
| - Reduction effect on inflammation by M1 macrophage | |||
| Human BMMSCs | MCT rat model | - Protective effects on PAH phenotypes | Oh et al.32) |
| Mice BMMSCs | Hypoxic mice model | - Anti-proliferative effects on pulmonary VSMCs | Liang et al.52) |
| - Cardioprotective effects | |||
| Rat BMMSCs | MCT rat model | - Improvement effect on PAH hemodynamics | Jiang et al.53) |
| - Recovery effect on RV hypertrophy and pulmonary vessel remodeling | |||
| - Prolonged effect on animal survival times | |||
| Rat BMMSCs | MCT rat model | - Ameliorating effect on RV impairment and survival time | Kanki-Horimoto et al.54) |
| Rat BMMSCs | MCT rat model | - Improvement effect on pulmonary function by inhibiting the ventricular remodeling | Luan et al.55) |
| Rat BMMSCs | MCT rat model | - Cardiovascular remodeling | Takemiya et al.56) |
| - Improvement effect on the prognosis in MCT treated rats | |||
| Rat BMMSCs | MCT rat model | - Attenuating effect on RVPSP, alveolar septum thickening, pulmonary arteriolar narrowing and RV hypertrophy | Umar et al.57) |
| - Improvement effect on RV function | |||
| Human UCMSCs | MCT rat model | - Suppressing effect on the hyperproliferation of VSMC | Liu et al.58) |
| - Regulating effect on the immunosuppressive activity | |||
| Human UCMSCs | Sugen5416/hypoxic mice model | - Attenuating effect on the tissue inflammation and injury in lungs and hearts | Alencar et al.59) |
| Human UCBMSCs | MCT rat model | - Protective effects on PAH phenotypes (RV function, cell engraftment, immune/inflammatory response) | Oh et al.32) |
| Human UCBMSCs | MCT rat model | - Decreasing effect on RV pressure | Lee et al.60) |
| - Regulating effect on the immunomodulation | |||
| Human ESCs | MCT mice model | - Extension effect on cell survival time | Zhang et al.61) |
AdMSC = adipose-derived mesenchymal stem cell; BMMSC = bone marrow-derived mesenchymal stem cell; ESC = embryonic stem cell; MCT = monocrotaline; PAH = pulmonary arterial hypertension; RV = right ventricular; RVPSP = right ventricular peak systolic pressure; UCBMSC = umbilical cord blood-derived mesenchymal stem cell; UCMSC = umbilical cord-derived mesenchymal stem cell; VSMC = vascular smooth muscle cell.
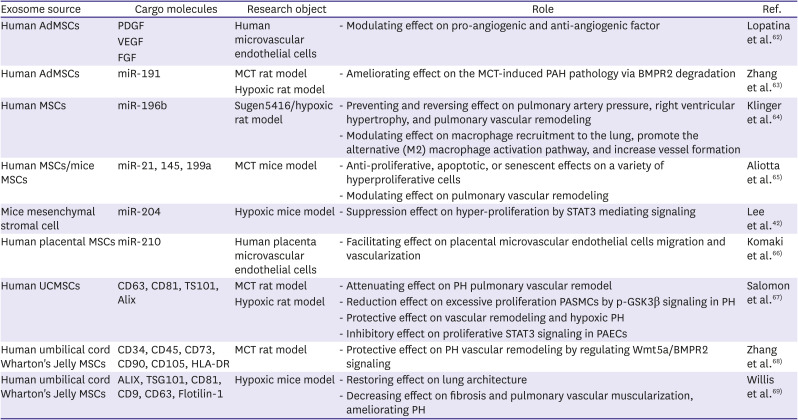
Table 2
Therapeutic role of stem cells-exosome in pulmonary arterial hypertension
| Exosome source | Cargo molecules | Research object | Role | Ref. |
|---|---|---|---|---|
| Human AdMSCs | PDGF | Human microvascular endothelial cells | - Modulating effect on pro-angiogenic and anti-angiogenic factor | Lopatina et al.62) |
| VEGF | ||||
| FGF | ||||
| Human AdMSCs | miR-191 | MCT rat model | - Ameliorating effect on the MCT-induced PAH pathology via BMPR2 degradation | Zhang et al.63) |
| Hypoxic rat model | ||||
| Human MSCs | miR-196b | Sugen5416/hypoxic rat model | - Preventing and reversing effect on pulmonary artery pressure, right ventricular hypertrophy, and pulmonary vascular remodeling | Klinger et al.64) |
| - Modulating effect on macrophage recruitment to the lung, promote the alternative (M2) macrophage activation pathway, and increase vessel formation | ||||
| Human MSCs/mice MSCs | miR-21, 145, 199a | MCT mice model | - Anti-proliferative, apoptotic, or senescent effects on a variety of hyperproliferative cells | Aliotta et al.65) |
| - Modulating effect on pulmonary vascular remodeling | ||||
| Mice mesenchymal stromal cell | miR-204 | Hypoxic mice model | - Suppression effect on hyper-proliferation by STAT3 mediating signaling | Lee et al.42) |
| Human placental MSCs | miR-210 | Human placenta microvascular endothelial cells | - Facilitating effect on placental microvascular endothelial cells migration and vascularization | Komaki et al.66) |
| Human UCMSCs | CD63, CD81, TS101, Alix | MCT rat model | - Attenuating effect on PH pulmonary vascular remodel | Salomon et al.67) |
| Hypoxic rat model | - Reduction effect on excessive proliferation PASMCs by p-GSK3β signaling in PH | |||
| - Protective effect on vascular remodeling and hypoxic PH | ||||
| - Inhibitory effect on proliferative STAT3 signaling in PAECs | ||||
| Human umbilical cord Wharton's Jelly MSCs | CD34, CD45, CD73, CD90, CD105, HLA-DR | MCT rat model | - Protective effect on PH vascular remodeling by regulating Wmt5a/BMPR2 signaling | Zhang et al.68) |
| Human umbilical cord Wharton's Jelly MSCs | ALIX, TSG101, CD81, CD9, CD63, Flotilin-1 | Hypoxic mice model | - Restoring effect on lung architecture | Willis et al.69) |
| - Decreasing effect on fibrosis and pulmonary vascular muscularization, ameliorating PH |
AdMSC = Adipose-derived mesenchymal stem cell; FGF = fibroblast growth factor; MCT = monocrotaline; MSC = mesenchymal stem cell; PAEC = pulmonary arterial endothelial cell; PASMC = pulmonary arterial smooth muscle cell; PAH = pulmonary arterial hypertension; PDGF = platelet-derived growth factor; PH = pulmonary hypertension; STAT3 = signal transducer and activator of transcription 3; UCMSC = umbilical cord-derived mesenchymal stem cell; VEGF = vascular endothelial growth factor.
For cell therapy, as representatives of stem cell therapy, iPSCs have shown application feasibility as reparative agents for lung diseases through designed disease models, drug stability screening tests, and direct replacements. However, many difficulties in clinical application exist, and when these cells are applied, more rigorous evidence must be supported in terms of accurate quality control and safety. Consistent, predictable and good-quality cell materials are essential for manufacturing commercial products. Thorough and powerful preclinical methodologic studies should be conducted to test these cell products in patients.
In terms of being free from cell therapy, exosomes obtained from diverse stem cells offer new therapeutic possibilities for cardiac revitalization. Exosomes moderate and control the main pathological signaling process of disease progression as superb communicators and exceptional transporters at the molecular level, leading to regeneration and the prevention of progressive diseases. Exosomes have many adhesion membrane proteins, which can be used for effective launching and tissue targeting. In addition, they possess resistant membrane proteins to assist hoarding and anchoring and might be beneficial in various alternative transplantation situations for patients with cardiovascular diseases. More than 200 clinical trials on exosomes are ongoing or have been completed thus far (http://clinicaltrials.gov), and further investigations are still needed in regenerative medicine, where long-term stability must be secured for exosomes’ usefulness as a therapeutic agent. The field of exosomes still has several hurdles to be overcome in therapeutic applications. Optimized technology can be used to obtain exosomes to efficiently engraft targeted tissues. Due to their heterogeneous nature, reproducibility is poor. A risk of immunologic reactions in recipients is evident due to the immunogenicity of the exosome membrane. To circumvent such immunological responses, personalized exosome analogs without immunity may be developed. In addition, the field of actual cell-free treatment extending beyond the limit of exosomes isolated from stem cells will unfold in the foreseeable future (Figure 1).
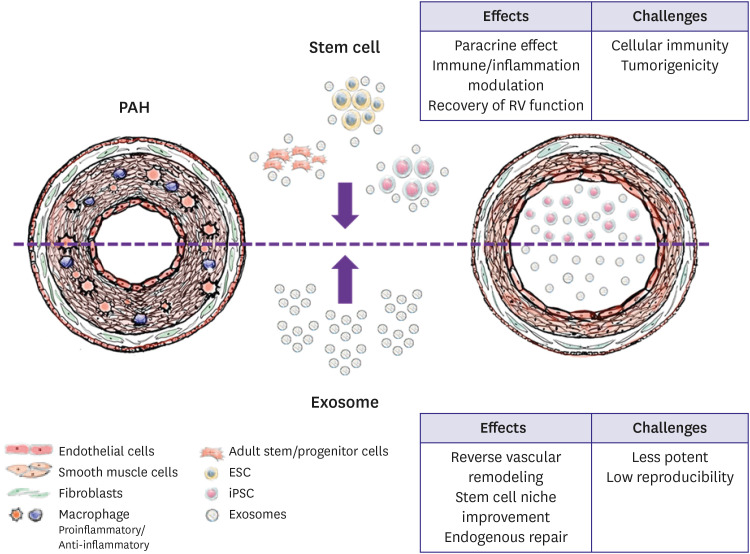
Figure 1
Major effects and clinical obstacles of stem cells and exosomes therapy.
Stem cells can be obtained by adult stem/progenitor cells, ESCs, and iPSCs. ESCs and iPSCs which have multi-potency to differentiate are faced several clinical obstacles as tumorigenicity, immunogenicity effects and de-differentiation after transplantation. Also, ESCs have ethical consideration and iPSCs confront financial burden. Adult stem/progenitor cells have limited proliferative capacity and variability quality. Exosomes which act anti-autophagy, anti-apoptosis, anti-proliferation, and mediating the proangiogenic action are presented as effective treatment. As intracellular messengers, exosomes can modulate critical role to reverse vascular remodeling process, but they have limitations in optimal isolation and less potency.
ESC = embryonic stem cell; iPSC = induced pluripotent stem cell; PAH = pulmonary arterial hypertension; RV = right ventricular.
Especially in cardiopulmonary diseases, which are linked to organs that do not regenerate well once damaged, these regenerative medicine-relevant therapies will introduce a new chapter by overcoming various difficulties.
 XML Download
XML Download