

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The femoropopliteal artery (FPA) is a common target for endovascular therapy in patients with symptomatic lower-extremity artery disease.1) However, providing optimal endovascular therapy for FPA disease is often challenging because these lesions are usually long, occlusive, and calcified.1) Furthermore, the FPA is affected by various mechanical forces generated by leg movements and surrounding structures.2) Implantation of self-expanding nitinol stents has been shown to achieve outcomes superior to those with balloon angioplasty in FPA lesions of intermediate lesion length.3) However, with increasing lesion length, the rate of restenosis after stent implantation rises significantly. In addition, stenting in the distal superficial femoral artery or popliteal artery and in long lesions has been associated with increased risk of stent fractures.4)
Drug-coated balloons (DCBs) with a concept of “leave nothing behind” emerged as an attractive treatment option for FPA disease. In randomized controlled trials and global registry studies, DCBs demonstrated excellent clinical outcomes.5)6)7)8) The recent guidelines recommend an endovascular-first strategy and drug-eluting technologies including DCBs for FPA lesions shorter than 25 cm.9) However, relatively long lesions frequently require provisional stenting due to severe arterial dissections or significant residual stenosis after DCB treatment.7)10) Furthermore, severe calcification has been shown to be associated with increased risk for restenosis after DCB.11) Thus, the reduction and modification of atherosclerotic plaques by atherectomy was suggested as a vessel preparation with potential to improve the outcomes of DCB.12)13) However, two pilot randomized controlled trials showed no significant superiority of atherectomy plus DCB (A+DCB) over DCB alone in the late clinical outcomes,14)15) and the clinical benefit of atherectomy prior to DCB remains uncertain.
Thus, we sought to investigate the efficacy of atherectomy in native FPA disease compared with DCB alone using a two-center cohort.
METHODS
Ethical statement
This study protocol complies with the latest ethical guidelines of the Declaration of Helsinki (2013). The Institutional Review Boards at the participating hospitals approved this study and waived the requirement for informed consent for the retrospective cohort patients (approval number: 4-2013-0463). All patients in the prospective cohort gave written informed consent to data collection.
Study populations
This study analyzed data from retrospective (from January 2006 to November 2016) and prospective (from December 2016 on) observational cohorts of patients who received endovascular therapy for lower-extremity artery disease at two endovascular centers (Severance Cardiovascular Hospital, Seoul, Korea and Chungnam National University Hospital, Daejeon, Korea). We identified a total of 478 patients who underwent endovascular revascularization with DCBs for FPA disease from December 2012 to September 2018. After exclusion of cases with in-stent restenosis, previous intervention with DCBs, and follow-up loss after hospital discharge, a total of 311 patients (348 limbs) with symptomatic native FPA disease were included in this analysis. Of this study population, 72 patients (82 limbs) were treated with atherectomy as vessel preparation prior to DCB angioplasty.
Endovascular procedure
All patients received maintenance daily doses of aspirin (100 mg) and 135 clopidogrel (75 mg) for at least 5 days before the procedure or loading doses of aspirin (300 mg) and clopidogrel (300 mg) 1 day before the procedure. Under local anesthesia, vascular access was obtained by percutaneous puncture of the ipsilateral or the contralateral common femoral artery depending on the location of the target lesion. After placement of a 6–7 Fr sheath, an intra-arterial bolus of heparin (70–100 U/kg) and additional heparin doses were administered to maintain an activated clotting time >250 sec during the procedure. A 0.035-, 0.018-, or 0.014-inch guidewires supported by a 4–5 Fr multipurpose catheter or microcatheter was used to pass the target lesions. Occlusive lesions with failed intraluminal recanalization were recanalized by a subintimal approach with reentrance into the true lumen. All lesions were routinely predilated with a balloon catheter except for patients treated with atherectomy prior to DCB. Pretreatment with an atherectomy device was performed at the operator's discretion in selected patients with heavily calcified or long lesions. Distal embolization protection devices (such as SpiderFX [Medtronic, Dublin, Ireland] or Emboshield NAV6 [Abbott Vascular, Santa Clara, CA, USA]) were used in selected cases of atherectomy when the target lesion was long or heavily calcified. After predilation or atherectomy, all lesions were treated with DCBs (IN.PACT Admiral [Medtronic Inc., Santa Rosa, CA, USA] or Lutonix [Bard, Tempe, AZ, USA]). In lesions requiring more than one DCB, a minimal overlap of 10 mm was obtained. If residual stenosis exceeded 30%, post-dilation was performed with an additional uncoated non-compliant balloon. Stenting was considered only as a last resort in the presence of flow-limiting dissection or when residual stenosis exceeded 30% despite post-dilation. After the procedure, dual-antiplatelet therapy with aspirin (100 mg/day) and clopidogrel (75 mg/day) was continued for at least 6 months unless contraindicated. The use of cilostazol (200 mg/day) was determined at the operator's discretion.
Study endpoints and definitions
The primary endpoint was primary clinical patency defined as freedom from symptom aggravation by at least one Rutherford category change combined with a decrease in ankle-brachial index (ABI) >0.15 or with presence of restenosis (≥50%) on imaging studies, such as duplex ultrasound, computed tomographic angiography, or intra-arterial angiography. For duplex ultrasound, peak velocity ≥180 cm/s or a lesion/adjacent-segment velocity ratio ≥2.4 was considered to indicate significant (≥50%) restenosis. Secondary endpoints were clinically driven target lesion revascularization (TLR) and major adverse limb events (MALE). TLR was defined as reintervention at the target lesion due to symptoms or decrease in ABI >0.15 when compared with post-procedure ABI. MALE was defined as above-ankle amputation of the index limb or major repeat revascularization of the target limb; and all causes of death.
Technical success was defined as residual stenosis ≤30%. A major complication was defined as any event that was either fatal or required surgical management or rehospitalization within 30 days of the procedure. Dyslipidemia was defined as either total cholesterol >200 mg/dL or previous treatment with a lipid-lowering agent.
The severity of arterial calcification was defined based on the peripheral arterial calcium scoring system.16) The presence of unilateral arterial calcification <5 cm in length on fluoroscopy was considered mild calcification (grade 1), whereas calcification was considered moderate if unilateral calcification was >5 cm (grade 2) or if bilateral calcification was <5 cm in length (grade 3). Bilateral calcifications >5 cm in length constituted severe calcification (grade 4).
Statistical analysis
Categorical variables are reported as numbers (percentages) and were compared using the chi-square test or Fisher exact test. Continuous variables are reported as mean ± standard deviation (SD) and were compared using Student's t-test. Propensity score matching (PSM) was performed to reduce treatment-selection bias and potential confounding factors and to adjust for significant differences in characteristics of patients or their lesions. Propensity scores were estimated using a non-parsimonious multiple logistic regression model for usage of atherectomy. Age, sex, hypertension, diabetes mellitus, dyslipidemia, end-stage renal disease, history of coronary artery disease, current smoker, history of a previous stroke, discharge medications (aspirin, clopidogrel, and cilostazol), Trans-Atlantic Inter-Society Consensus (TASC) II C or D lesions, total occlusion, popliteal artery involvement, lesion length, runoff numbers of below-the-knee arteries, and the variables that were significantly different between the two classified groups (critical limb ischemia, chronic kidney disease, combined treatment of infrapopliteal lesion, severe calcification) were selected to calculate the propensity score. Balanced propensity scores were gathered to compare the efficacy of the A+DCB strategy. A local optimal algorithm using the caliper method was used to develop propensity-score–matched pairs without replacement (1:1 match). To ensure that poorly fitting matches were excluded, a matching caliper of 0.2 SDs from the estimated propensity score logit was enforced.
Primary clinical patency, TLR-free survival, MALE-free survival, and overall survival were quantified using the Kaplan-Meier method and were compared by the log-rank test. To identify risk factors of restenosis, univariate and multivariate Cox proportional hazard regression analyses were performed with all baseline clinical and procedural variables. All p svalues were determined in two-sided tests, and p values <0.05 were considered statistically significant. Analyses were performed using IBM SPSS (version 25, Chicago, IL, USAs).
RESULTS
Baseline characteristics
The present study included a total of 348 limbs from 311 patients with native FPA disease who were treated with DCBs (IN.PACT Admiral [Medtronic] or Lutonix [Bard]). Of this study population, 82 limbs (72 patients) were treated with A+ DCB and 266 limbs (236 patients) were treated with DCB without prior atherectomy. Baseline clinical characteristics are summarized in Table 1. The A+ DCB group showed less frequent chronic kidney disease (CKD) (22.0% vs. 34.2%, p=0.050) and critical limb ischemia (31.7% vs. 52.3%, p=0.002) compared with the DCB group. Other characteristics were comparable between the two groups. After PSM, 82 matched pairs of each group were generated. All baseline clinical variables did not differ significantly between the two matched groups. The mean age of the matched study population was 70.2±10.7 years. Diabetes and CKD was present in 73.2% and in 22.0%, respectively.
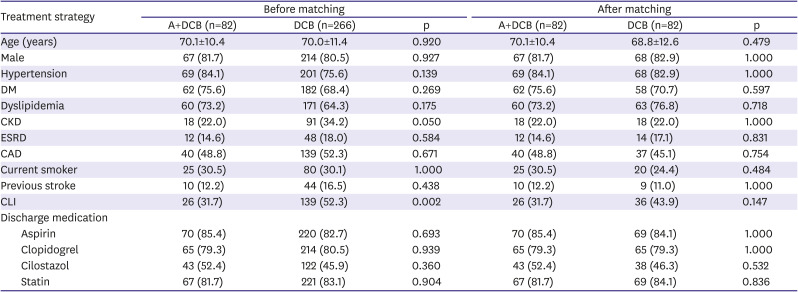
Table 1
Baseline clinical characteristics
Data are presented as mean±standard deviation or number (%).
A+DCB = atherectomy plus DCB; CAD = coronary artery disease; CKD = chronic kidney disease; CLI = chronic limb ischemia; DCB = drug coated balloon; DM = diabetes mellitus; ESRD = end stage renal disease.
![]()
Lesion and procedural data
Lesion and procedural characteristics and in-hospital outcomes are summarized in Table 2. Whereas the A+ DCB group showed more severe calcification (46.3% vs. 17.7%, p<0.001) and intravascular ultrasound use (19.5% vs. 6.0%, p=0.001), the DCB-only group had more combined treatment of infrapopliteal lesions (31.7% vs. 45.5%, p=0.037). After PSM, all lesion variables were comparable between the two groups except intravascular ultrasound usage. For the matched study groups, the mean lesion length was 172.7±111.2 mm. TASC II C or D lesion type and severe calcification was present in 49.4% and 43.3%, respectively.
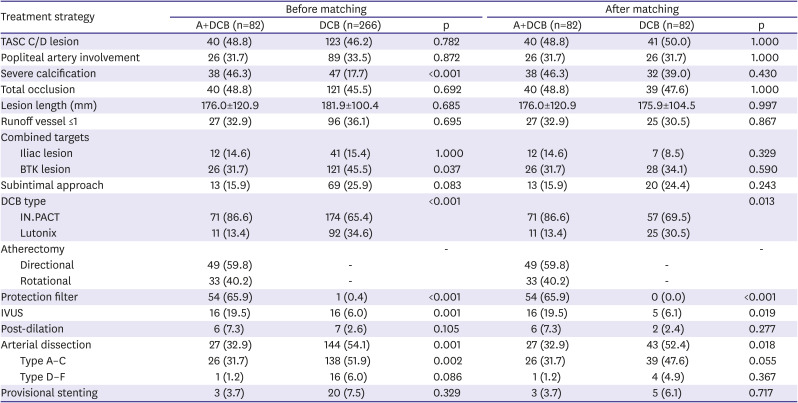
Table 2
Lesion and procedural characteristics
Data are presented as mean±standard deviation or number (%).
A+DCB = atherectomy plus DCB; BTK = below the knee; DCB = drug coated balloon; TASC = Trans-Atlantic Inter-Society Consensus; IVUS = intravascular ultrasound.
![]()
In the A+DCB group, two types of atherectomy devices were used, directional devices (59.8%) and rotational devices (40.2%). Embolization protection filters were used in 65.9% of the A+DCB group. The incidence of arterial dissections was lower in the A+DCB group than in the DCB group (32.9% vs. 52.4%, p=0.018). However, the incidence of complex dissection types, including types D, E, and F, was low and showed no difference between the A+DCB and the DCB groups (1.2% vs. 4.9%, p=0.367). The provisional stenting rates also did not differ significantly between the two groups (3.7% vs. 6.1%, p=0.717). Other procedural characteristics, such as subintimal wiring approach and post-dilation, showed no difference between the two groups.
The technical success rate was higher in the A+DCB group than in the DCB group (80.5% vs. 62.2%, p=0.015) (Table 3). However, the A+DCB group showed more procedure-related minor complications (37.0% vs. 13.4%, p=0.047), including distal embolization and vascular perforation. Regarding the distal embolization rate, there was no difference according to the type of DCB in both groups.
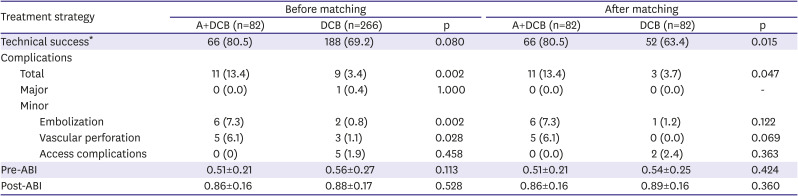
Table 3
Immediate procedure outcomes
Data are presented as mean ± standard deviation or number (%).
ABI = ankle-brachial index; A+DCB = atherectomy plus DCB; DCB = drug coated balloon.
*Defined as residual stenosis ≤30%.
![]()
Mid-term clinical outcomes
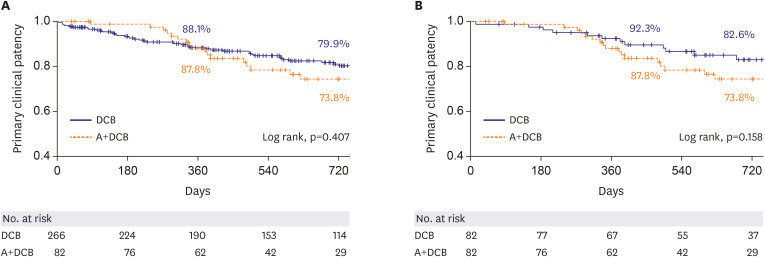
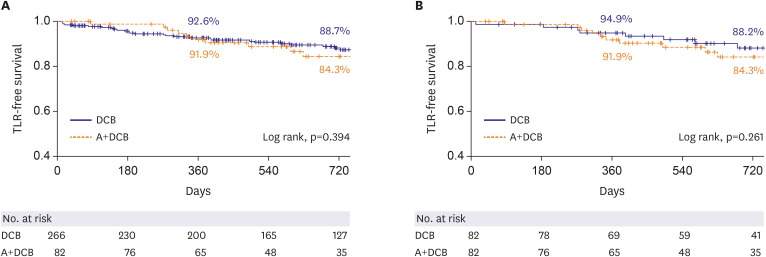
Patients were clinically followed for a mean duration of 24.8±14.3 months. The 2-year primary clinical patency did not differ significantly between the A+DCB and the DCB group before the PSM (73.8% vs. 79.9%, p=0.407) or after the PSM (73.8% vs. 82.6%, p=0.158) (Figure 1 and Supplementary Table 1). Similarly, 2-year TLR-free survival was also not different between the two groups before (84.3% vs. 88.7%, p=0.394) and after the PSM (84.3% vs. 88.2%, p=0.261) (Figure 2 and Supplementary Table 1). The rates of mortality (11.8% vs. 18.5%, p=0.385) and the MALE (21.2% vs. 13.2%, p=0.147) at 2 years also showed no difference between the two matched groups (Supplementary Table 1).
Cox proportional hazard regression multivariate analysis was performed to investigate predictors of loss of clinical patency (Table 4). In this analysis, atherectomy showed no impact on the loss of patency (hazard ratio [HR], 1.25; 95% confidence interval [CI], 0.74–2.13; p=0.408) and TLR (HR, 1.32; 95% CI, 0.69–2.52; p=0.395). Diabetes mellitus (adjusted HR, 0.38; 95% CI, 0.21–0.70; p=0.019) and end-stage renal disease (adjusted HR, 2.17; 95% CI, 1.04–4.55; p=0.040) were identified as independent predictors for the loss of primary clinical patency.
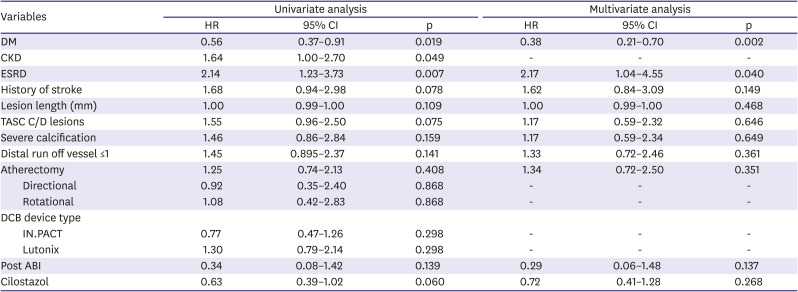
Table 4
Univariate and multivariate Cox proportional hazard analysis for the predictors of loss of primary clinical patency
ABI = ankle-brachial index; CI = confidence interval; CKD = chronic kidney disease; DCB = drug coated balloon; DM = diabetes mellitus; ESRD = end-stage renal disease; HR = hazard ratio; TASC = Trans-Atlantic Inter-Society Consensus.
![]()
DISCUSSION
In this two-center cohort study, the A+DCB achieved a higher technical success rate compared with DCB alone; however, it was associated with more frequent minor procedure-related complications, including distal embolizations and vascular perforations. The primary clinical patency and TLR-free survival showed no significant difference between the two treatment strategies.
Endovascular atherectomy has been adopted to achieve plaque reduction and modification with lower risk of arterial dissections after adjunctive balloon dilation.12) Particularly, the debulking of heavily calcified plaques by atherectomy is considered to improve the vessel response to balloon dilation and the delivery of antiproliferative drug to the vessel wall.11)17) In the present study, pretreatment with atherectomy prior to DCB significantly reduced the incidence of arterial dissection (32.9% vs. 48.8%) and residual stenosis >30% (19.5% vs. 36.6%), resulting in improved technical success (80.5% vs. 62.2%) compared with DCB alone. The A+DCB group showed a trend toward less provisional stenting than the DCB group, although the difference was not statistically significant (3.7% vs. 6.1%). Two small randomized controlled trials also reported similar findings.14)15) In these studies, vessel preparation with atherectomy prior to DCB significantly reduced the incidence of severe dissections and successfully reduced the need for stenting. Despite these favorable immediate results, these trials did not demonstrate superior outcomes of A+DCB compared with DCB alone in primary patency or TLR-free survival. A meta-analysis of five clinical studies also found no statistically significant advantages of atherectomy in addition to DCB in terms of the primary patency or TLR.18) One of the major limitations of these previous trials was the insufficient statistical power due to small study populations. Thus, it remains inconclusive whether atherectomy prior to DCB has clinical benefit in the treatment of FPA disease. Several other factors also need to be considered as reasons why clinical outcomes of atherectomy could not be shown despite theoretical advantages. Firstly, atherectomy in the trials, including the present study, might have not been optimal in the reduction or modification of plaques. It is still unknown how much plaque-volume reduction is required for the optimal late outcomes. On the other hand, excessive atherectomy may induce medial or adventitial injury, which promotes restenosis.19) Secondly, atherectomy prior to DCB may be beneficial only in certain complex lesion subsets, such as heavily calcified or long lesions. Fanelli et al. found that severe calcification was a significant risk factor for loss of patency after DCB.11) Severe calcification may limit the arterial response to balloon dilation and impede the uptake of antiproliferative drugs by the arterial wall. Cioppa et al.17) reported a 1-year primary patency rate of 90% after A+DCB in severely calcified femoropopliteal lesions. In the long-lesion subgroups of the Lutonix and IN.PACT global registries, arterial dissection occurred in 34.3% and 62.1% and provisional stenting was required in 35.7% and 39.4%, respectively.7)10) The incidences of complex type dissections were 14.9–16.7% in these studies. In the present study, the arterial dissection rate was observed in 52.4% of the DCB group, whereas the A+DCB group showed significantly fewer dissections (32.9%). Unlike the previous studies, the complex type dissections were rare and comparable (1.2% vs. 4.9%, p=0.367) between the two groups. The provisional stenting rates remained low in both groups (3.7% vs. 6.1%, p=0.717). However, in complex lesions such as long or calcified lesions with greater tendency towards arterial dissections, pretreatment with atherectomy has potential to reduce the requirement for stenting. Furthermore, in so-called “no-stenting zones,” such as the common femoral or popliteal artery, use of atherectomy prior to DCB may also help to avoid stenting.20)21) Thus, lesion subsets which may benefit from combined atherectomy and DCB need to be in future investigations.
However, there are also disadvantages related to atherectomy. Previous studies reported a high incidence of distal embolization during atherectomy procedures and advocated use of embolic protection devices.22)23) In our study, embolic protection filters were used in 65.9% of cases and observed distal embolization in 7.3%. Meanwhile, a recent study reported that association between the different DCB profiles and distal embolic events.24) However, our results revealed no difference in distal embolic events regarding the type of DCB in both the A+DCB group and the DCB group. In addition, there were five cases (6.1%) of vascular perforation caused by atherectomy devices. A meta-analysis reported a vascular perforation rate of 2.6%.18) Furthermore, use of atherectomy and embolic protection devices is associated with higher medical costs. Therefore, objective cost-effective analysis is also required in the future.
In this study two types of atherectomy devices were used, directional and rotational. The type of atherectomy device showed no impact on the primary patency. In previous studies, male gender, severe calcification, obesity, lesion length, previous ipsilateral revascularization, chronic limb ischemia, and hypercholesterolemia have been reported as risk factors for restenosis after DCB.25)26)27) In the present study, end-stage renal disease was identified as a predictor for loss of primary patency after DCB angioplasty. Interestingly, diabetes was found to be associated with lower risk of restenosis. In a previous study, insulin-dependent diabetes was reported as a predictor of TLR.26) However, whereas previous studies enrolled diabetic patients as 40–45% of cases,5)6)7)8) diabetes was present in more than 70% of enrolled cases in this study. Thus, this finding needs to be understood with regard to study population characteristics.
This study has several limitations. First, this was a retrospective, non-randomized study with inherent limitations, such as differences in the baseline characteristics and potential confounding factors. In particular, detailed reasons for operators' decisions to use one or the other type of atherectomy device could not be fully discerned. Even though we tried to minimize confounding factors using PSM, the bias in the selection of the devices cannot be excluded. Second, this study may be underpowered to assess true differences in late clinical outcomes between the two treatment groups. Third, we defined primary patency based on clinical and hemodynamic status supported by available imaging results. Thus, clinical patency might overestimate target lesion patency rates compared to the primary patency based on the imaging modalities only. Fourth, provisional stenting was performed only in 6.1% of the matched DCB group in this study, despite the suboptimal angiographic results with 52.4% postoperative dissection and 36.6% residual stenosis greater than 30%. Due to this conservative stenting strategy, which deviates from those of previous studies, generalization of the clinical results of the DCB in this study appears to be limited.
In conclusion, the pretreatment with atherectomy improved technical success of DCBs; however, it was associated with increased minor complications. Atherectomy showed no clinical benefit in terms of TLR-free survival or primary patency compared with DCB alone.
 XML Download
XML Download