

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Percutaneous coronary intervention (PCI) is widely used to treat coronary chronic total occlusion (CTO) owing to its improved success rate in recent years attributed to advanced technology and medical devices. Even though improved ischemic symptoms and functional capacity after CTO-PCI has been proven by several randomized trials and large observational studies, there is still ongoing debate regarding the survival benefits of CTO-PCI.1)2)3)4)5)6)7)8) Not only different clinical demographics, angiographic characteristics, but also ischemic burden of subtended myocardium may play a role in the discrepancies of these results.
Ischemic burden is a geometric measure of the severity of ischemia to subtended myocardium owing to an occluded coronary artery. There has been clear evidence that patients with large myocardial ischemic burden experience future cardiovascular events and increased mortality at higher rates, and also benefit from coronary revascularization compared with patients with small ischemic burden.9)10)11)12) Patients with large myocardial ischemic burden may be suitable candidates for PCI to improve survival by reducing ischemic extent significantly. The appropriate use criteria proposed the assessment of ischemic burden to be required for decision-making for percutaneous revascularization in patients with CTO lesions.13) However, studies which assessed ischemic burden in patients with CTO are still lacking. Therefore, we investigated ischemic burden using single photon emission computed tomography (SPECT) in patients diagnosed with coronary single vessel CTO by coronary angiography.
METHODS
Ethical statement
All study participants were provided informed consents, and Institutional Review Board (IRB) of Asan Medical Center approved this study (IRB approval No. 2017-0321).
Study population, data collection, and definitions
In total, 928 patients were included in the CTO registry of the Asan Medical Center (Seoul, South Korea) from January 2007 to July 2015. This registry enrolled patients who underwent successful PCI for CTO which met the criteria: 1) occlusion of major epicardial vessels with a Thrombolysis In Myocardial Infarction 0 flow in a reference vessel with a diameter ≥2.5 mm, and 2) angina symptoms or evidence of ischemia which lasted for at least 3 months. For this study, population with single vessel CTO without any significant lesions (>50% luminal stenosis) in other epicardial coronary arteries were screened first. Among them, the patients with available SPECT results acquired during hospitalizations before any kind of revascularization treatment were finally included in this study.
Clinical, angiographic, and procedural data of study subjects were collected in a dedicated electronic database by independent research personnel through the reviews of electrical medical records or telephone interviews. Two cardiologists who were unaware of the clinical information and SPECT results of the participants analyzed index angiography including the assessment of CTO characteristics (location, segment length, anatomical complexity, and collateral grades to distal part of CTO vessels) and the presence of other epicardial coronary artery disease.
CTO locations in epicardial coronary arteries were categorized into 3 segments (proximal, middle, or distal) in LAD and RCA CTOs, and 2 segments (proximal or distal) in LCX CTO.14) The anatomical complexities of CTOs were assessed based on the Japanese-CTO (J-CTO) score.15) Collateral grades for vessels distal to occluded vessels were assessed by coronary angiography according to the Rentrop scale.16)
Myocardial SPECT acquisition and analysis
The SPECT acquisition protocol was described previously.17) In brief, post-stress and redistribution-gated SPECT using 201Tl chloride was acquired after adenosine stress and after 4 hours (redistribution). Patients stopped the consumption of caffeine and drugs which contained aminophylline and theophylline 24 hours before the test. Adenosine was intravenously administered (for periods >6 minutes) at a rate of 140 μg/kg/min. At peak stress, 74–148 MBq of 201Tl was injected intravenously depending on the body weight. After 6 minutes of adenosine infusion, post-stress myocardial perfusion images were acquired using Ventri (GE Healthcare, Chicago, IL, US), Infinia (GE Healthcare), Ecam (Siemens, Munich, Germany), Symbia T2 (Siemens), or Precedence 16 (Philips, Amsterdam, Netherland). All systems were equipped with low-energy, general-purpose collimators. Images were reconstructed with ordered-subset expectation-maximization with two iterations and 10 subsets. No attenuation or scatter correction was applied. Semi-quantitative analysis of SPECT images was performed using a 17-segment model and a 5-point scale (0 to 4) according to the current American Society of Nuclear Cardiology guideline by an experienced nuclear cardiologist (S. Han) in a blinded manner.18)19)
In addition to individual segment score, summed stress score (SSS), summed rest score (SRS), and summed difference score (SDS) were calculated for the assessment of ischemic burden. The SSS and SRS were defined as the sum of the individual score in all 17-segments in stress and redistribution phase images.20) SDS was calculated by subtracting the SRS from the SSS. Ischemic burden was defined as the SDS divided by the possible maximal score (68 = 4 × 17 segments) in the entire myocardium, and was presented as percent scores (= SDS/68). Fixed ischemic burden indicated the percentage of the irreversible amount of myocardium (= SRS/68).18)21)
Statistical analysis
Continuous variables are analyzed and reported as median with interquartile range values in the entire population and each CTO group, and categorical variables were expressed as frequencies. Comparisons of SPECT results between different CTO groups were performed using the Kruskal–Wallis test for continuous variables or Fisher’s exact test for categorical variables. For the prediction of high-ischemic burden (>10%),12) the multivariate logistic regression model with backward elimination was used. Initial input variables are as follows: age, sex, initial presentation, smoking, hypertension, diabetes, dyslipidemia, chronic kidney disease, prior myocardial infarction, peripheral vascular disease, baseline ejection fraction (EF), occluded coronary vessel, CTO location, J-score, collateral grade, CTO length, and presence of regional wall motion abnormality. All reported p values are two-sided. A p value less than 0.05 was considered statistically significant. Analyses were performed with the use of the software R (version 3.5.3; R Project for Statistical Computing, Vienna, Austria).
RESULTS
Study population and baseline characteristics
In the population of Asan-CTO registry, single vessel CTOs in the absence of significant lesions in other epicardial coronary arteries were identified in 407 patients. Of them, 165 patients with available SPECT results were eligible for this analysis. The median age of the study patients was 60 years and 84.8% were men. Prior history of myocardial infarction was observed in 18 patients (10.9%), and 51 patients (30.9%) underwent PCI before their enrolment in the study. The median baseline EF was 60.0%, and regional wall motion abnormality was found in 76 patients (46.1%) (Table 1). Comparison in baseline demographics of single-vessel CTO patients with or without SPECT is summarized in Supplementary Table 1.
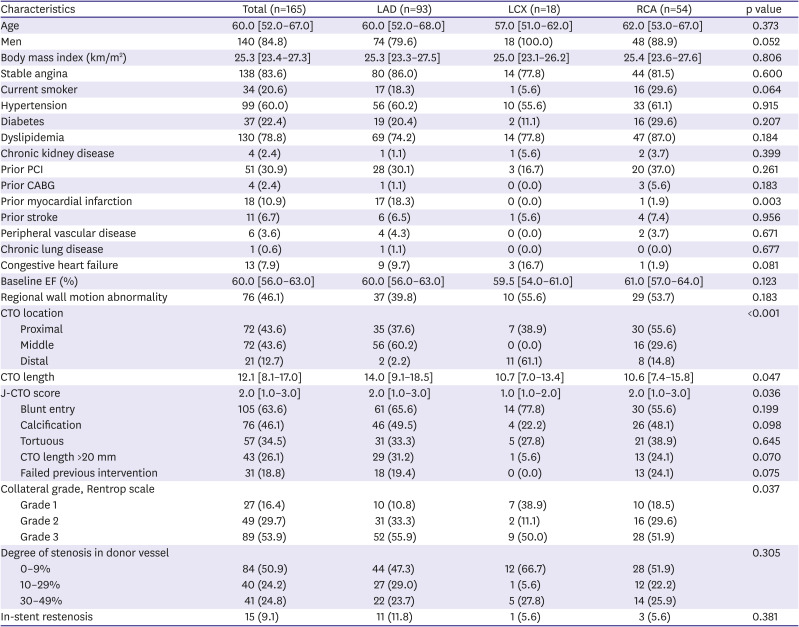
Table 1
Baseline demographics and angiographic findings
Values are presented as median [interquartile range] or number (%).
CABG = coronary artery bypass graft; CTO = chronic total occlusion; EF = ejection fraction; J-CTO score = Japanese-CTO score; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; PCI = percutaneous coronary intervention; RCA = right coronary artery.
![]()
Left anterior descending coronary artery (LAD), left circumplex coronary artery (LCX), and right coronary artery (RCA) CTO accounted for 93 patients (56.4%), 18 (10.9%), and 54 (32.7%), respectively. There were statistically significant differences in CTO location, CTO length, J-CTO score, and collateral grade according to the CTO vessels. The most prevalent location of CTO was at the middle part of the LAD CTO, and in the distal or proximal parts of the LCX or RCA. Collateral grade ≥ Rentrop scale 2 was found in more than 80% cases of LAD or RCA CTOs. There were no differences in the prevalence of in-stent restenotic CTO cases in the 3 groups.
SPECT analysis
Table 2 and Figure 1 show the results of SPECT of the entire population and differential groups according to CTO vessels. The median SSS and SRS were 11.0 (8.0–16.0) and 3.0 (0–8.0) in the LAD CTO group, which yielded the highest scores compared with those of LCX and RCA CTO groups. (p<0.001 and p=0.037). The median SDSs of LAD, LCX, and RCA CTO groups were 7.0 (5.0–10.0), 4.0 (2.0–7.0), and 4.0 (2.0–6.0), respectively. The prevalence of high-ischemic burden (>10%) of the entire study population was 40%. The median ischemic burden of LAD CTO was 10.3%, and 47 patients (50.5%) had high-ischemic burden (>10%) in LAD CTO group. Significantly lower numbers of patients in the LCX and RCA CTO groups had high-ischemic burdens compared with LAD CTO group (33.3% and 24.1%, p=0.001).
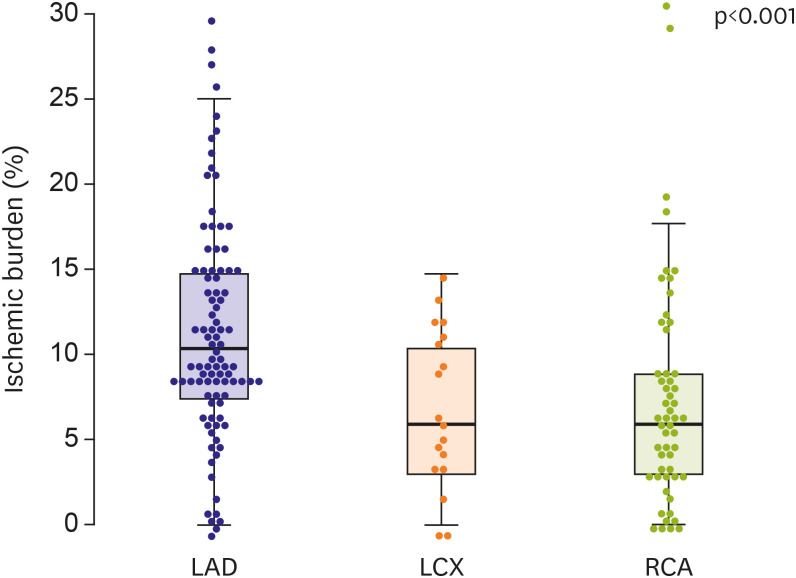
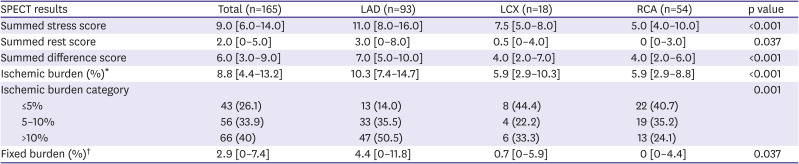
Figure 1
Box-Whisker plot of ischemic burden in each coronary vessel CTO.
CTO = chronic total occlusion; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery
![]()
Table 2
SPECT result according to the CTO vessels
Values are presented as median [interquartile range] or number (%).
CTO = chronic total occlusion; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery; SPECT = single photon emission computed tomography.
*Ischemic burden = (summed difference score/68); †Fixed ischemic burden = (summed rest score/68).
![]()
Analysis of the ischemic burden according to the location of the CTO lesion and collateral grade defined by Rentrop scale in each coronary artery is illustrated in Figure 2. In the proximal LAD CTO, the median value of the ischemic burden was 14.7%, and the middle and distal LAD CTO were 8.8% and 8.1%, respectively (p=0.037). By contrast, there was no significant relationship between the lesion location and ischemic burden in the LCX and RCA CTOs. In the LAD CTO group, there was no correlation between the collateral scale and ischemic burden (grade 1, 10.3%; grade 2, 11.8%; grade 3, 8.8%; p=0.51). This null relationship was also observed in LCX and RCA CTO groups. Figure 3 shows 2 representative cases in the study subjects.
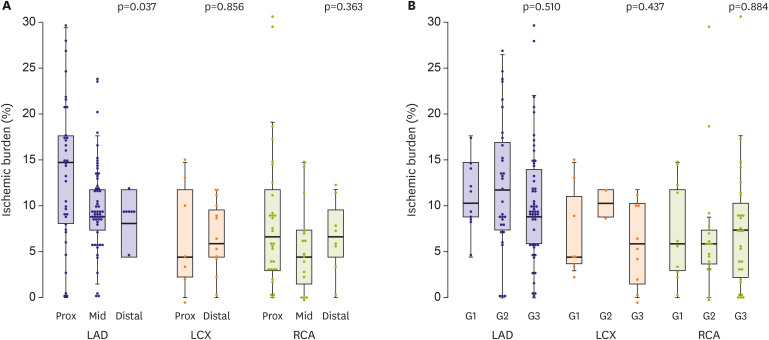
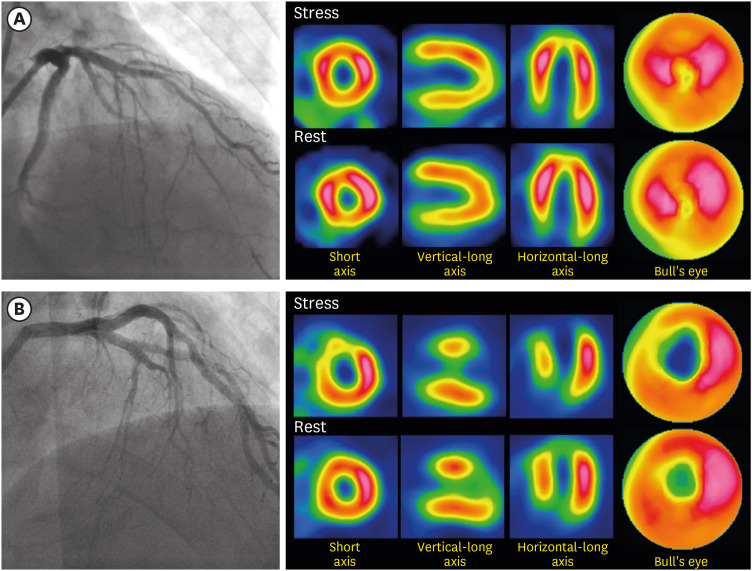
Figure 2
Box-Whisker plot of ischemic burden in each coronary vessel CTO according to CTO location or collateral grade. (A) Ischemic burden based on the location of CTO in each coronary vessel. (B) Ischemic burden based on Rentrop collateral grade in each coronary vessel.
CTO = chronic total occlusion; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery.
![]()
Figure 3
Angiography and SPECT images of representative 2 cases. (A) The 65-year-old man presenting with stable chest pain started 4 months ago. An echocardiogram showed EF of 63%, and there was no regional wall motion abnormality. Angiography showed mid LAD CTO with collateral grade 3 via diagonal branch and septal-septal channels. The SPECT showed a low ischemic burden (SRS = 3, SSS = 4, SDS = 1, ischemic burden = 1.5%). (B) The 72-year-old man presenting with stable chest pain started 8 months ago. An echocardiogram showed EF of 47%, and there was regional wall motion abnormality in LAD territory. Angiography showed mid LAD CTO with collateral grade 2 via diagonal branch and septal-septal channels. The SPECT showed a high ischemic burden (SRS = 6, SSS = 20, SDS = 14, ischemic burden = 20.1%).
CTO = coronary total occlusion; EF = ejection fraction LAD = left anterior descending coronary artery; SDS = summed difference score; SPECT = single photon emission computed tomography; SRS = summed rest score; SSS = summed stress score.
![]()
Predictors of high-ischemic burden
Table 3 lists the results of univariate and multivariate logistic regression models for the prediction of high-ischemic burden. The statistically significant predictors of high-ischemic burden after multivariate analysis were the presence of hypertension, baseline EF >45%, LAD CTO, proximal CTO location, and de novo CTO. Anatomical complexity quantified by the J-CTO score, collateral grade, and CTO length was not a predictor of high-ischemic burden.
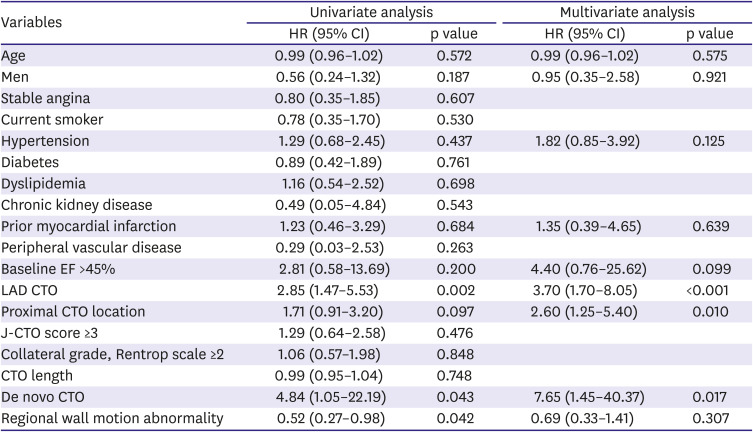
Table 3
Logistic regression models for the prediction of high-ischemic burden
CI = confidence interval; CTO = chronic total occlusion; EF = ejection fraction; HR = hazard ratio; J-CTO = Japanese-CTO; LAD = left anterior descending coronary artery.
![]()
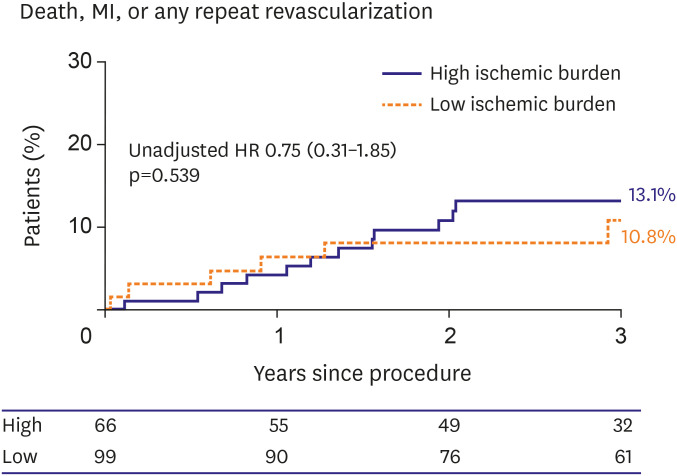
Clinical outcomes
Figure 4 shows long-term clinical outcomes according to ischemic burden (high >10% and low ≤10%) at baseline SPECT result. There was no difference in the rate of composite endpoint including all-cause mortality, myocardial infarction, or any repeat revascularization at 3 years since index CTO-PCI.
DISCUSSION
We evaluated the ischemic burden in patients with single vessel CTO with the use of SPECT analysis. The major findings of the study were as follows: 1) In patients with single vessel CTO, high-ischemic burden (defined as values >10%) was identified in 40% of all CTO patients. Most of these patients were in the LAD CTO group. 2) The presence of hypertension, baseline EF >45%, LAD CTO, proximal location of CTO, and de novo CTO were the statistically significant predictors of the high-ischemic burden in multivariate analysis. 3) The anatomical complexity was measured based on the J-CTO score, CTO length, and the angiographically determined collateral grade, which was not associated with the high-ischemic burden.
PCI for CTO has been accepted as an established treatment option over the past decades, and the rationale for the use of this treatment is the relief of ischemia and the reduction of jeopardized myocardium supplied by the occluded coronary vessel.22)23)24) Our study results showed that only 40% of the total population suffered from ischemia which covered >10% of the total myocardial geometry. Most of the high-ischemic burden patients had the CTO in the LAD coronary artery. Uncertain survival benefit was observed in the CTO-PCI from contemporary randomized trials which compared PCI and optimal medical treatment for CTO.6)7)8) A total of 60% of patients in our patients had ischemic burdens <10%. These findings would partly explain why these randomized trials concluded neutral PCI effects in terms of survival benefits in patients with CTO.
To assess the true ischemic burden induced by CTO itself in the coronary artery, single vessel CTO without significant disease in other coronary arteries should be evaluated. However, to date, only limited data have existed for the assessment of the ischemic burden of the single vessel CTO disease. A prior study evaluated the ischemic burden in patients with CTO, and high-ischemic burden (>10%) was found in 56.8% of the patients, which was higher than our results.25) However, the referred study included patients with multivessel disease. Thus, the results could be biased to higher ischemic burdens because of the significant stenosis in the other coronary arteries. Our study excluded patients with coronary stenoses >50% in other epicardial arteries. Presented results showed relatively low prevalence of high-ischemic burden. Cardiac magnetic resonance was used in a previous study to assess changes after CTO-PCI, and reported that all patients had reversible perfusion defects with variable degrees of ischemia (subendocardium in 37%, transmural in 13%, peri-infarct ischemia in the subepicardial viable rim in 50%).26) Myocardial perfusion reserve was significantly lower in the CTO territory compared with remote territories. This was improved after CTO-PCI, and outcomes reached levels which were similar to those in remote territories of the left ventricle. However, there are still limited studies evaluating the true ischemic burden in CTO. Accordingly, additional studies with large sample sizes, and use of different diagnostic modalities are needed.
Collateral flow is the main blood supply to the myocardium at distal parts of the occluded vessel. The Rentrop scale based on angiography is a common tool used for the assessment of collateral flow, and good collateral channel and flow were deemed to be associated with a sufficient blood supply to the subtended myocardium. In a previous study, a higher collateral flow index measured by a pressure wire was associated with favorable cardiovascular outcomes in stable coronary disease in long-term follow-ups.27) However, the results of our study showed lack of significant impacts of collateral grade to the SPECT results and the degree of ischemia. Discrepancy between collateral grade and objective ischemia measured by SPECT could be explained by a coronary “steal phenomenon” during adenosine stress or microvascular dysfunction.28)29) In addition, the collateral grade in our study was determined by angiography alone that can neglect microvascular function. SPECT imaging was superior in its ability to predict future cardiac events than angiographically defined collateral grade in CTO patients.30) Therefore, assessing whether there is sufficient blood supply to the distal myocardium of the CTO segment by angiography alone may be misleading, and SPECT analysis should be considered to assess the true ischemic burden of the CTO segment.
In the nuclear sub-study of the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial (where patients with CTOs were excluded), patients with a large ischemic burden were associated with improved survival after revascularization.12) A large registry study also showed that early revascularization was beneficial when ischemic burden was >12.5%.11) However, CTO lesions need more complex techniques accompanied with higher rates of periprocedural complications when compared with stenotic coronary disease. Therefore, careful decisions for the treatment should be made by considering the patient’s baseline demographics, anatomical complexity, as well as ischemic burden, especially when SPECT is used, to achieve improved long-term survival after revascularization.
There are several limitations in our study. First, this study is a retrospective analysis of a small-sized dataset from a single tertiary center. Therefore, there must be selection bias in the enrolment of study subjects, and the results cannot be directly applied to other clinical settings. Second, ischemic burden assessment using SPECT was performed in selected populations with single vessel CTO, which imposes an inevitable bias in the selection of the study population. Since PCIs for CTO without SPECT are often performed in many patients suspected of having obvious ischemic symptoms and signs that might impose higher ischemic burden, it is possible that the true ischemic burden of a single vessel CTO might be underestimated in our result even though there were no differences between patients whether undergoing SPECT or not in terms of CTO vessel, location, baseline EF, and regional wall motion abnormality. Third, a large number of patients show significant stenosis of coronary arteries other than the CTO in clinical practice and previous studies. Our result cannot directly be applied to those patients with multi-vessel disease involving CTO. Forth, the ischemic burden was calculated only with the use of SPECT with a semi-quantitative process, and not compared with other modalities, such as cardiac positron emission tomography, or magnetic resonance. However, SPECT is widely used modality that has been validated in many studies in assessing objective ischemia in coronary artery disease. Fifth, we did not compare ischemic burden of CTO and stenotic coronary artery disease. Finally, our study did not include the clinical outcomes after CTO-PCI according to the grade of the ischemic burden.
In conclusion, we evaluated the ischemic burden in patients with single vessel CTO using SPECT. High-ischemic burden was found only in 40% of total population, and they were more likely to have LAD CTO, proximal location, preserved left ventricular function, and de novo CTO. The collateral grade and anatomical complexity assessed by the coronary angiography alone were not associated with true ischemic burden. The assessment of ischemic status with the use of SPECT should be considered when treatment decisions are made to improve the clinical outcomes following PCI for CTO.
 XML Download
XML Download