

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The clinical spectrum of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) ranges from asymptomatic or mild disease with or without mild respiratory symptoms to critical disease with acute respiratory distress syndrome or sepsis.12 In addition, reports of neurological manifestations in COVID-19 patients have increased rapidly since they were first described in Wuhan, China.3 These manifestations may be due to the neurotropism of SARS-CoV-2 or collateral injury due to concurrent inflammatory cascades.4
Seizure is an uncommon complication of COVID-19 with a prevalence of less than 1%,23567 and may be caused by nonspecific mechanisms, such as fever, hypoxia, cytokine storm, and metabolic derangements.8 Rarely, seizures may also occur due to meningoencephalitis associated with COVID-19.91011 Here, we describe the clinical characteristics of six hospitalized patients who developed new-onset seizures after SARS-CoV-2 infection at the National Medical Center in Seoul, South Korea.
Go to : 
CASE DESCRIPTION
A total of 1,487 patients with confirmed COVID-19 were admitted to our hospital during the study period (June 2020 and August 2021). Out of these, six patients (0.4%) developed new-onset seizures during hospitalization. For the purpose of this study, patients with epilepsy (PWE) or a prior history of seizure were excluded. Patient demographics and clinical characteristics are summarized in Table 1. Patients’ age ranged from 39 to 84 years, and four of the six patients were older than 60 years. Five patients were men. According to the COVID-19 disease severity classification, all patients had severe or critical COVID-19.1 In addition, all six patients were admitted to an intensive care unit (ICU), accounting for about 3.6% of all COVID-19 patients admitted to the ICU (n = 169) during the study period.
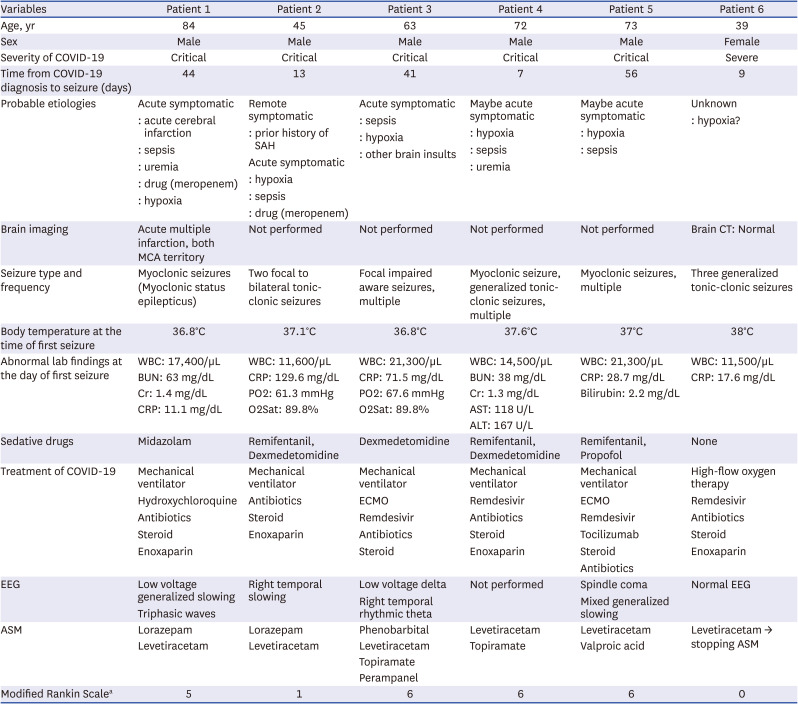
Table 1
Demographics and clinical characteristics of the six reported patients
COVID-19 = coronavirus disease 2019, SAH = subarachnoid hemorrhage, MCA = middle cerebral artery, CT = computed tomography, WBC = white blood cell, BUN = blood urea nitrogen, Cr = creatinine, CRP = C-reactive protein, PO2 = partial pressure of oxygen, O2Sat = oxygen saturation, AST = aspartate aminotransferase, ALT = alanine transaminase, ECMO = extracorporeal membrane oxygenation, EEG = electroencephalography, ASM = antiseizure medication.
aModified Rankin Scale: 0 (no symptom), 1 (no significant disability despite symptoms), 2 (slight disability), 3 (moderate disability), 4 (moderately severe disability, unable to walk unassisted), 5 (severe disability, requires constant nursing care and attention), 6 (dead).
![]()
The duration from COVID-19 diagnosis to seizure onset ranged from 7 to 56 days (mean duration: 28 ± 21 days). Because most patients were receiving mechanical ventilation and/or extracorporeal membrane oxygenation therapy, only two patients underwent brain-imaging. Diffusion-weighted imaging in Patient 1 showed multiple acute infarctions in both hemispheres (Fig. 1). Patient 2 had a history of subarachnoid hemorrhage 2 years prior, but he experienced his first seizure after COVID-19 infection. All patients except Patient 6 had acute respiratory distress syndrome and sepsis. Patients 1 and 2 were receiving meropenem (seizure threshold-lowering antibiotics). Patient 6 was a postpartum woman (3 days after delivery), who had two generalized tonic-clonic seizures within 24 hours while receiving high-flow oxygen therapy in the ICU. She did not have symptoms suggestive of eclampsia, such as headache, elevated blood pressure, proteinuria, or peripheral edema. Her brain computed tomography (CT) scan and electroencephalography (EEG) were normal.
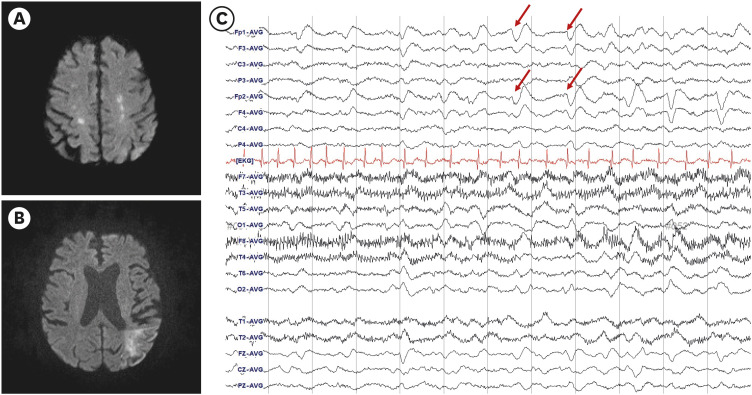 | Fig. 1Brain imaging and EEG of patient 1. (A, B) Diffusion-weighted imaging shows multiple acute infarctions in both hemispheres (both internal borderzones and left posterior borderzone of middle cerebral artery territory). (C) EEG reveals diffuse slowing with triphasic waves (arrows).EEG = electroencephalography.
|
All five patients with critical disease were receiving mechanical ventilation and continuous intravenous sedation(s) (remifentanil, dexmedetomidine, midazolam, or propofol). Five patients underwent EEG, and most findings showed nonspecific diffuse cerebral dysfunction and/or sedation effects, such as generalized slowing, spindle coma, or triphasic waves. Patient 3 had recurrent focal clonic seizures of the left face and arm. His EEG revealed electrographic seizures of intermittent rhythmic theta waves in the right temporal electrodes. However, there was no motor seizure (i.e., nonconvulsive seizure) during EEG monitoring.
All patients experienced multiple seizures, and seizures in Patient 1 met the criteria for status epilepticus (myoclonic seizures > 5 minutes). Patient 6 had two generalized tonic-clonic seizures, whereas the other three patients had myoclonic seizures. Focal seizures with or without bilateral tonic-clonic seizures were observed in two patients. In five patients, seizures responded to one or two antiseizure medications (ASMs). Patient 3 received four ASMs to reduce the electrographic seizures.
Three patients died due to COVID-19 pneumonia or sepsis, and one had a severe disability at discharge. Patients 2 had no significant disability, and Patient 6 was fully recovered at discharge.
Go to :
DISCUSSION
In select COVID-19 cases, neurological complications may manifest as seizures.12 A prospective, multicenter study of neurological disorders in COVID-19 revealed that seizures occurred in 74 of 4,491 patients (1.6%).5 Out of those 74 patients, 34 (46%, 0.76% of overall patients) had no prior history of seizure or epilepsy. In another observational study, the incidence of seizure was 5 out of 6,147 patients (0.08%).6 A recent systematic review reported that 127 out of 15,467 patients (1%, 95% confidence interval:0–2%) experienced seizure as a complication of COVID-19.2 In our study, the frequency of seizures was less than 1%, suggesting that seizures are a rare complication in patients with COVID-19.
The mechanisms behind the neurological manifestations of COVID-19, including seizures, are not yet fully understood. A postmortem analysis of brain samples from patients with COVID-19 demonstrated the presence of SARS-CoV-2 viral protein in 21 (53%) of the 40 examined patients.13 Another study reported the presence of SARS-CoV-2 in cerebrospinal fluid (CSF) samples of 17 (6%) out of 304 patients.14 SARS-CoV-2 enters human host cells via the spike (S) protein through angiotensin-converting enzyme 2 (ACE2) receptors, found on various endothelial cells, including those in the lung, blood vessels, kidneys, and small intestine.15 The ACE2 receptor is also present on the pericytes of the blood-brain barrier, choroid plexus, neocortical neurons, glial cells, and olfactory epithelial cells, making these cells potential targets for SARS-CoV-2.101617 SARS-CoV-2 may invade the central nervous system through the olfactory epithelium/bulb or hematogenous spread across a destroyed blood - brain barrier.1017 However, detection of SARS-CoV-2 in the CSF of patients with seizures who have COVID-19 is uncommon (13%), and even when it is present, the significance of this finding is unknown.18
Various indirect mechanisms, such as fever, hypoxia, hypoperfusion, cytokine storm/septic encephalopathy, coagulation dysfunction, cardiovascular disturbance, metabolic derangement, and multiorgan failure, may also be associated with the development of seizures in patients with COVID-19.81017 Meningoencephalitis related to COVID-19 can cause seizures or status epilepticus.91011
In this case series, most patients had structural lesions or medical illnesses that could affect the development of seizures. Several systemic insults (e.g., metabolic derangements and hypoxia), acute brain insults, and certain medications can lead to acute symptomatic seizures.1920 Patient 1 had myoclonic seizures, and his EEG showed triphasic waves associated with metabolic or toxic encephalopathy. Therefore, the etiology of his seizures was more likely to be sepsis, uremia, or seizure threshold-lowering drug (e.g., meropenem) than acute cerebral infarction. On the other hand, in the case of Patient 2, the remote subarachnoid hemorrhage was likely a major cause of seizures considering focal onset seizures. Patient 6, a postpartum woman with COVID-19, had no obvious cause of seizures, though hypoxia and fever may have contributed to her seizures. Additionally, as none of the patients underwent lumbar puncture, and brain imaging was performed only in two patients, encephalitis or encephalopathy due to direct invasion of SARS-CoV-2, or other brain structural etiologies could not be excluded.
Early systematic reviews described that the mean duration from the onset of initial COVID-19 symptoms to the development of seizure was 5 days.21 The seizure was also described as an initial presenting symptom of COVID-19.622 However, in half of our patients, seizures occurred late after COVID-19 onset. Late-onset seizures may be because the patients had severe or critical COVID-19 disease (that is, after COVID-19 disease had progressed). In another case report, seizures occurred 3 weeks after COVID-19 diagnosis in two patients with critical disease.23
Continuous EEG monitoring is an important tool for detecting seizures and assessing brain function in the critical care environment. In a case series of 100 non-postarrest patients with COVID-19 monitored with EEG, seven patients (7%) were positive for seizures.24 This incidence is similar to or slightly lower than the incidence of seizures (10–11%) in other critically ill patients admitted to medical ICUs.2526 In addition, nonconvulsive seizure is an uncommon contributor to encephalopathy in patients hospitalized with COVID-19.24 In our study, the incidence of seizures in COVID-19 patients admitted to ICU (3.6%) was much lower than in studies using continuous EEG monitoring, but similar to the incidence reported in a previous study investigating clinical seizures in medically ill patients admitted to ICU (3.47%).27 Since only patients with clinical motor seizures underwent EEG, subtle seizures or nonconvulsive seizures may have been more prevalent in our cohort. In summary, seizures do not appear to occur more frequently in patients with severe/critical COVID-19 than in patients with other critical medical illnesses.
All our patients had severe or critical COVID-19 and half died. However, a recent systematic review found no association between seizure and severity of COVID-19.2 Moreover, altered mentation or stroke were associated with higher in-hospital mortality in COVID-19, but not seizures.7 Several previous studies included patients with a prior history of seizure or epilepsy.5722 Therefore, those studies may have included habitual or breakthrough seizures in PWE as well as seizures directly associated with COVID-19. In addition, fever is one of the seizure precipitants in PWE, and therefore the frequency of seizures in PWE may increase even in mild COVID-19 cases.28 In other case series, most of the patients with COVID-19 who developed new-onset seizures were critically ill.2329
New-onset seizures are a rare complication of COVID-19, but may occur more commonly in critically ill patients. Nonspecific mechanisms related to COVID-19 can trigger the development of acute symptomatic seizures. In addition, direct brain invasion of SARS-CoV-2 may be related to the occurrence of seizures in some COVID-19 patients with seizure.
Ethics statement
The Institutional Review Board of the National Medical Center reviewed and approved the study protocol (Approval No. NMC-2022-01-001). The need to obtain informed consent was waived by the board.
Go to :
 XML Download
XML Download