

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vitrification has a wide range of clinical applications and is currently the recommended technique for cryopreserving embryos.1 Utilizing the frozen embryo transfer (FET) method could circumvent the unfavorable effects of controlled ovarian stimulation on the uterine environment and embryonic synchronicity, resulting in a higher clinical pregnancy rate (CPR) and implantation rate (IR).2 The clinical usability of FET cycles affects consistency in patient care and live birth rates (LBRs) as well as the financial, emotional, and time costs associated with FET cycles.3 Vitrification, known to be safe and efficient, has a broad range of clinical applications. Moreover, vitrified-warmed blastocyst transfer increases the survival rate (SR) and LBR.4 Recently, vitrification is becoming increasingly popular among patients who have undergone 'freeze-all' cycles, had vitrification of surplus embryos, and are at risk of ovarian hyperstimulation syndrome or impaired endometrial receptivity.5 Currently, FET accounts for up to one-third of all children born in the USA with the use of assisted reproductive technology (ART).6
Amongst the indicators of embryo quality, the morphological characteristics based on embryo development are known to be the most basic and important factors; hence, embryo quality is the most important predictor of a successful pregnancy.78 The relationship between the extended culture duration and clinical outcomes has not been fully established. The methodologies of extended culture have not been standardized either; therefore, whether extended culture duration affects clinical outcome remains inconclusive. Embryos derived from patients of advanced maternal age (AMA) are known to be more vulnerable to culture environment than those derived from younger patients.9
The World Health Organization (WHO) and Obstetrical and Gynecological Survey define AMA as a mother’s age > 35 years. A rising proportion of women with AMA has led to a growing trend in ART use and an increasing demand for fertility services.10 In ART cycles, clinical outcomes are highly associated with increasing maternal age. The significant decrease in fertility is related to a decrease in ovarian reserve, a reduction in the number of follicles, and deterioration in embryo quality. Medical complications include an increased risk of adverse pregnancy outcomes.1011
The purpose of this study was to investigate the association between extended culture duration and pregnancy outcomes in patients of AMA. The considerations were as follows: 1) LBR by single vitrified-warmed blastocyst transfer (SVBT) embryo morphology and age combined; and 2) LBR by transfer according to post-warming extended culture duration of blastocysts.
METHODS
Patient characteristics
We conducted a retrospective cohort study to analyze the outcomes of 697 SVBT cycles in women aged < 41 years between January 2016 and December 2017 at the CHA Fertility Center, Gangnam. Pregnancy outcomes regarding neonatal information were obtained using an electronic medical record base, and telephone surveys were conducted for missing data. Of 960 SVBT cycles, cases with short-term culture duration (2–5 hours) or day 3 and day 7 embryo transfer (ET) were excluded, as were individuals who were aged ≥ 41 years, had more than ten years of infertility, had unknown culture duration, and had endometrial thickness less than 7 mm or uterine anomalies. A total of 697 SVBT cycles were included and divided into 3 groups according to the age of the female partners: group I: < 35 years (n = 407), group II: 35–37 years (n = 176), group III: 38–40 years (n = 114).
Recording and calculation of blastocyst culture duration
All procedures were conducted under the electronic witnessing system (Witness®; RI Ltd., Rugby, UK) to keep track of the exact times of all individual parts of the in vitro fertilization (IVF) cycle. RI witness is an ART management system that reduces the risk of human error and safeguards every step of the IVF cycle. Culture duration was recorded based on the time between day 5 thaw and ET using the RI witness system.
Vitrification and warming of blastocysts
The vitrification and warming procedures were performed as described in our previous study.12 For vitrification, artificial shrinkage and assist hatching were performed using the laser system ZILOS-tk (Hamilton Thorn Bioscience Inc., Beverly, MA, USA). The blastocysts were pre-equilibrated in an equilibration solution (7.5% v/v, dimethyl sulfoxide [DMSO] and 7.5% v/v, ethylene glycol [EG]) for 2.5 minutes at 37°C. Blastocysts were then equilibrated with a vitrification solution containing 15% DMSO, 15% EG, and 0.5 mol/L sucrose for 20 seconds. The blastocysts were loaded onto an EM gold grid with a minimal volume of vitrification solution and immediately plunged into SN2 using a VitMaster (IMT, Ness Ziona, Israel).
For warming, the EM gold grid was sequentially transferred into the warming solution (0.5, 0.25, 0.125 and 0.0 M of sucrose) at intervals of 2.5 minutes. Blastocysts were placed in an incubator set at 37°C, 6% CO2, 5% O2, and 89% N2 and cultured overnight. The intactness of the embryo and degree of re-expansion were examined.
Blastocyst quality evaluation and grading
The methods used to evaluate embryo quality and grading were described in our previous study.13 The morphological scores of the blastocysts were assessed as follows14: (Blastocoel Expansion Score) × (Inner Cell Mass Score) × (Trophectoderm Score). The development score was assigned as follows: early blastocyst = 1, expanding (mid) blastocyst = 2, expanded or fully expanded blastocyst = 3, hatching blastocyst = 4, and hatched blastocyst = 5. The scores for the inner cell mass and trophectoderm were assigned separately based on their grade, as follows: A = 3, B = 2, and C = 1. The quality of blastocysts was divided into three groups based on their morphological scores: good (blastocyst score: 45–16), average (blastocyst score: 15–8), and poor (7–1).
Preparation of the endometrium in the SVBT cycle and ET
The preparation of the endometrium in the SVBT cycle and ET procedure was in accordance with the procedure followed in our previous study.15 In brief, the endometrium was prepared for transfer in natural or hormonal replacement cycles. An ET catheter (COOK®, Bloomington, IN, USA) was used to transfer the warmed blastocysts under abdominal ultrasound guidance. Luteal phase support was provided through progesterone vaginal suppositories or intramuscular injection starting 5 days before the ET and continued until 10 weeks of gestation.
Clinical outcome measures
To assess IVF treatment outcomes, serum beta-human chorionic gonadotropin (β-hCG) levels were measured 11 days after ET. A rise in serum β-hCG level (> 20 IU) was considered positive for pregnancy. The IR was calculated as the number of gestational sacs per total number of transferred embryos. Clinical pregnancy was confirmed by the presence of a fetal heartbeat via ultrasonography. Miscarriage was defined as the spontaneous cessation of a clinical pregnancy. LBR was calculated as the number of live births/total number of embryos transferred. The number of live births included only viable infants delivered at > 28 weeks gestation. Obstetric outcome parameters were birth weight, gestational age at delivery, and presence of congenital anomalies. Preterm and post-term births were defined as deliveries before 37 or after 42 completed weeks of gestation, respectively. Neonatal birth weight was categorized into three categories: normal (2.5–4.0 kg), very low birth weight (< 2.5 kg), and macrosomia (> 4.0 kg).
Statistical analysis
All statistical analyses were performed using SPSS ver. 22 (IBM, Armonk, NY, USA). Data are shown as the mean ± standard error of the mean. Data were analyzed using one-way analysis of variance followed by Duncan’s multiple range test. Statistical significance was set at P < 0.001.
Ethics statement
The present study protocol was reviewed and approved by the ethics committee of the Institutional Review Board of CHA Gangnam Medical Center (IRB approval number: GCI 2020-10-004). Owing to the retrospective design of the study, the need for participant consent was waived, and only medical records were used in this analysis.
RESULTS
Patient’s demographics and characteristics of previous IVF cycle
Data regarding the general characteristics of previous fresh IVF cycles are presented in Table 1. Unexplained infertility was more common in the AMA group, probably because of their age, and was significantly different between the groups (37.8%, 50.0%, and 39.5%, P = 0.022). As expected, significantly fewer oocytes were retrieved among the AMA group than among the young age group (16.6, 14.9, and 12.4, P < 0.001), and the fertilization and blastocyst rates were significantly decreased between the groups (11.5, 10.5, and 8.8; 4.5, 3.5, and 3.1, respectively; P < 0.001).
Table 1
Comparison of demographics, patient characteristics, and cycle outcomes among three groups Values are presented as number (%) or mean ± standard deviation. Group I: age < 35 years, group II: age 35–37 years, group III: age 38–40 years.
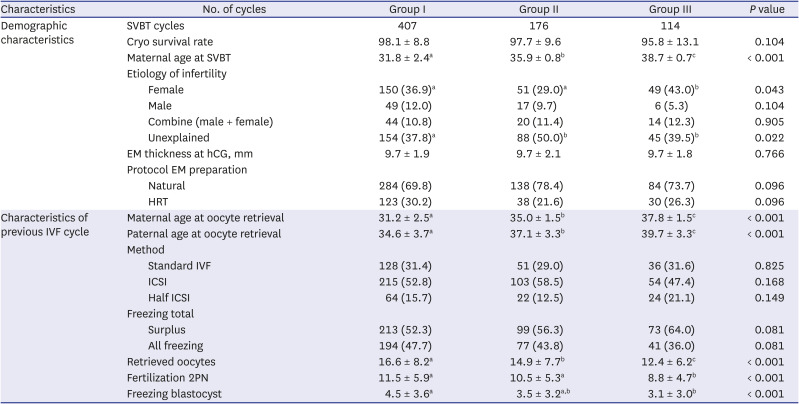
SVBT = single vitrified-warmed blastocyst transfer, EM = Endometrial, hCG = human chorionic gonadotropin, HRT = hormone replacement treatment, IVF = in vitro fertilization, ICSI = intracytoplasmic sperm injection, PN = pronuclear.
a,b,cDifferent superscript denotes a significant difference (P < 0.001).
Morphologic grades and culture duration
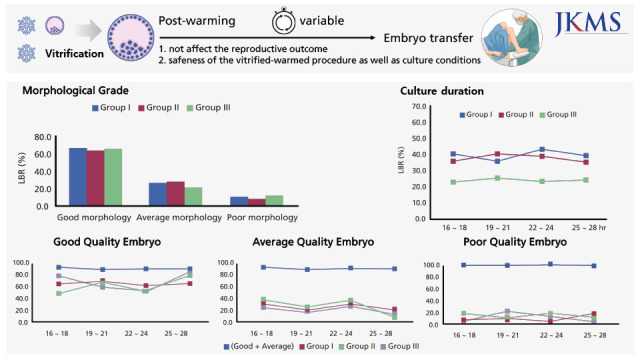
The LBR based on the morphological grades and post-warming extended culture duration is shown in Fig. 1. SVBT embryos were categorized based on their morphological grades as follows: good, average, and poor (Fig. 1A). The LBR per transfer increased with an improvement in blastocyst morphology, and over 80% of vitrified-warmed blastocysts were hatching or hatched on the day of transfer. Accordingly, the good grade had a significantly higher birth rate than the average and poor grades (good: 66.3%, 64.2%, and 66.7%; average: 25.0%, 26.9%, and 20.0%; poor: 8.8%, 9.0%, and 13.3%, respectively; P < 0.001). However, no significant differences were observed in morphological parameters between the embryos of women with AMA and those of younger women.
Fig. 1
Relationship between live birth rate (LBR) and morphological grades and groups. (A) The morphological grades have been sorted into three categories (good: excellent & good quality, average: fair quality, poor: poor quality). The good group had a significantly higher birth rate than average and poor groups (P < 0.001). However, the difference between the average and poor groups was not statistically significant. There was also no statistically significant difference when comparing individual groups within the same morphological grade. (B) LBR by transfer according to blastocyst culture duration and the woman’s age group. (C) Morphological grades by transfer according to blastocyst culture duration and the woman’s age group. The characteristics of the three groups are as follows: (Good + Average)/Total. Competency value, group I: age < 35 years, group II: age 35–37 years, group III: age 38–40 years.
a,bDifferent letters within a column indicate significant differences at P < 0.05.

To determine the result of culture duration in each group, we further divided the culture duration into 4 groups to track the LBR. The result is presented in Fig. 1B. We also analyzed LBR followed by embryo quality and extended culture duration. Our results are presented in Fig. 1C. The linear trend is shown regardless of extended culture duration. The differences in LBR and morphological grades between the post-warming extended culture duration and the woman’s age were not statistically significant.
Clinical outcomes of SVBT cycles
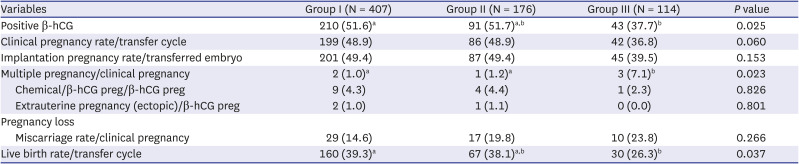
Clinical outcomes after SVBT are presented in Table 2. There were significant differences between patients in groups I, II, and III in the percentage of positive beta-hCG (51.6%, 51.7%, and 37.7%, P = 0.025), multiple pregnancies (1.0%, 1.2%, and 7.1%, P = 0.023), and LBR (39.3%, 38.1%, and 26.3%, P = 0.04). The miscarriage rate increased with age, but no significant difference was found between the groups (14.6%, 19.8%, and 23.8%, P = 0.266).
Table 2
Clinical outcomes of embryo transfer
Neonatal outcomes (obstetrical outcomes)
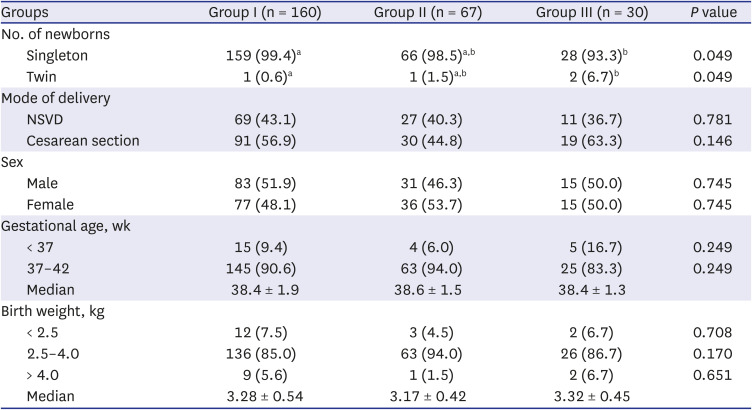
Table 3 shows the obstetric outcomes of the three groups. A total of 257 infants were born. There were no significant differences in sex ratio (percentage of male infants, 51.9% vs. 46.3% vs. 50.0%), median gestational age (38.4 ± 1.9 vs. 38.6 ± 1.5 vs. 38.4 ± 1.3 weeks), median birth weight (3.28 ± 0.54 vs. 3.17 ± 0.42 vs. 3.32 ± 0.45 kg), percentage of low birth weight infants (7.5% vs. 4.5% vs. 6.7%), and incidence of macrosomia (5.6% vs. 1.5% vs. 6.7%) among the three groups. The proportion of preterm birth in group III was high, but was not significantly different from that in the other groups (9.4% vs. 6.0% vs. 16.7%, P = 0.249).
Table 3
Neonatal outcomes of single blastocyst transfer
DISCUSSION
Recently, the SVBT cycle has been increasingly utilized for ART owing to its low morbidity. Consequently, improving the efficiency of the SVBT cycle is essential. One of the issues that has been the focus of recent interest and debate is the optimal culture duration for the vitrified-warmed cycle.
To the best of our knowledge, this is the first study to assess post-warming extended culture duration of SVBT in relation to morphological grades of embryos and its ultimate effect on clinical and obstetric outcomes. Our results indicated that there were no statistically significant differences in morphological grades with variation of the extended culture duration during SVBT. We found no significant differences in SR, CPR, LBR, miscarriage rate, and obstetric outcomes of groups with various culture durations after SVBT. Therefore, we suggest that post-warming extended culture is not harmful for AMA patients regardless of the duration.
Delaying marriage is a current trend worldwide, and consequently, the average age of women giving birth to their first child is also increasing. ART services are in high demand among women of AMA and has become more acceptable.10 The optimal timing of ET, especially SVBT, is essential for successful pregnancy in ART cycles. The study of culture duration and ET timing may provide a way to improve pregnancy rates in patients with AMA. Nevertheless, there is still a lack of evidence in the literature to support this phenomenon. Embryos derived from older patients are more vulnerable during embryo development, but no evidence has been found to support this in the literature. Culture conditions are a major factor that can have long-lasting effects on offspring health.16 Thus, culture duration is an important deciding factor for embryo development and clinical outcomes, especially because embryos of women with AMA are more likely to be sensitive to the culture environment than those of younger women.
The optimal post-warming culture duration has been debated for the past few years. Previous studies have suggested that long-term culture does not improve embryonic developmental potential, and most studies have dealt with vitrified-warmed cleavage stage embryos.171819 In contrast, long-term culture generally results in better embryo expansion during embryo development. It has been reported that overnight culture is the most effective method for transferring embryos after evaluating embryo viability, development status, cell damage/recovery, and developmental ability. Previous studies also stated that post-thaw cleavage resumed after overnight culture.18 However, the optimal post-warming culture duration that determines the developmental potential of blastocysts is yet to be standardized.20 We performed a follow-up study to investigate the post-warming extended culture duration in further detail. As shown in our results, embryonic morphological grades based on different culture durations was not significantly different between patients of AMA and young patients. Therefore, we assume that extended culture duration is not harmful during embryo development (Fig. 1A and C). Additionally, our results did not show a significant increase in pregnancy rate following post-warming extended culture, but embryo quality score and blastocyst status improved. It is believed that among the myriad of factors that affect the results of an SVBT, increased age hinders successful embryo implantation.2122 Correspondingly, one could conclude that increased age is a factor that affects CPR/LBR. Another interesting result of our study was that various culture durations did not affect obstetric outcomes (Fig. 1B). Additionally, AMA has no adverse effects on gestational age, birth weight, or congenital malformation rates (Table 3).23 However, our results also showed a high proportion of multiple pregnancy rates followed by monozygotic twinning (MZT). The incidence of MZT is higher with ART use than in natural conception. The mechanism underlying MZT has not yet been established. According to our study, extended culture improved the hatching stage of the embryo, which may cause embryo splits. This is consistent with previous reports.2425
There were some limitations to this study. First, our study had a retrospective design, which limited the range of analysis. Second, we excluded patients aged ≥ 41 years and did not distinguish between Day 5 and Day 6 embryos. This could be attributed to the small sample size, which may have caused bias and sampling error. Therefore, further studies are necessary on patients aged 41 years and older to assess the impact of older age on various clinical outcomes. To overcome these limitations, our study has several strengths. First, we examined both clinical and obstetric outcomes. Second, to our knowledge, this was the largest study to evaluate the optimal timing of ET that considered the morphological grades of oocytes in SVBT. Additionally, as this was a single-center study, embryos were cultured in the same media using the same techniques, allowing us to avoid errors that may arise from using different media or techniques. Another notable strength of our study is that the blastocysts were morphologically graded.
In conclusion, we determined that post-warming extended culture duration did not affect clinical and obstetric outcomes of SVBT. Therefore, SVBT can be considered stable regardless of culture duration. We also found that culture duration did not affect morphological grades. Accordingly, it should not be fixed but adjusted freely based on the laboratory workflow. This is important given the wide application of SVBT in an attempt to improve clinical and obstetric outcomes for women of AMA.
 XML Download
XML Download