

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
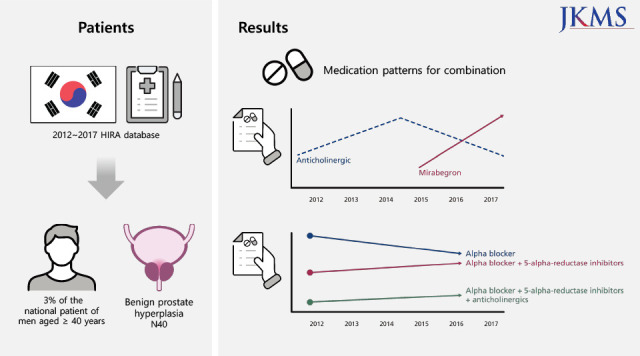
Benign prostatic hyperplasia (BPH) is a common condition in men over the age of 40. BPH causes lower urinary tract symptoms (LUTS), which have a significant adverse effect on quality of life.1 LUTS increases prevalence with age, and can be divided into voiding (e.g., hesitancy, straining, slow stream, intermittency, feeling of incomplete emptying) and storage (frequency, urgency, urge incontinence, nocturia) symptoms. It is known that the storage symptom is the more bothersome of the LUTS.2 Today, South Korea is one of the fastest aging countries in the world, and BPH is one of the major concerns of patients, healthcare providers, and governments.
The main treatment for LUTS/BPH is medication.2 The management of patients diagnosed with LUTS/BPH using a combination of drugs should be based on extensive knowledge and experience, depending on patient-specific conditions such as age, general conditions, subjective symptoms and clinical findings such as prostate size. Alpha-adrenergic receptor blockers (alpha blockers) such as tamsulosin, terazosin, alfuzosin, silodosin, doxazosin are most commonly prescribed as a first-line treatment for men with LUTS caused by BPH. The 5-alpha-reductase inhibitors (5ARI) such as finasteride and dutasteride are recommended for patients with a large prostate (≥ 30 mL).3 Depending on the patient’s presenting symptoms, combination therapy with other categories of drugs can be performed. Anticholinergics (ACH) and/or beta-3-agonist (mirabegron) in combination with an alpha blocker are recommended for those with moderate-to-severe storage symptoms, while desmopressin (DSM) may be offered as a treatment option to those with nocturnal polyuria.3
The prevalence of BPH and prescribed drug categories using nationwide databases has been reported4567; however, the actual data involving the initial prescription patterns for men diagnosed with BPH are limited. Therefore, this study investigated drugs initially prescribed for men diagnosed with BPH, and evaluated changes in the patterns of prescribed drugs for the period of 2012 to 2017 using the Health Insurance Review and Assessment (HIRA) database in Korea.
Go to : 
METHODS
Database and study population
The National Health Insurance Service (NHIS) in South Korea represents an extensive government-managed healthcare system that includes almost all domestic residents. The HIRA database includes the details of all medical services provided, including medical institutions, diagnosis, medication, and surgery of all registered residents, and provides nationwide information regarding epidemiological data and utilization of medical resources in South Korea.
The data we used is sampled data, and the meaning of ‘total patient extraction rate 3%’ means ‘collect all patient data after extracting 1.3% patients.’ After stratifying a sample of 3% of all patients, all treatment details of the patient are constructed as data. The advantage is that compared to the US AHRQ and Taiwan NHRI sample data which are made in a similar format, this data was collected on a patient-by-patient basis, and the socio-economic factors of patients were reflected in the stratified method, so it is very appropriate data to analyze the trend of treatment by year. However, the disadvantage is that it is impossible to tract because the patient’s unique key and the nursing institution’s unique key are newly assigned by year and data type.8
We extracted data involving 3% of the national patient sample of men aged ≥ 40 years between 2012 and 2017 from the HIRA database and investigated the prescribed drugs for men with the BPH code of N40 in the International Classification of Diseases, 10th revision (ICD-10). Men with a diagnosis of BPH but not receiving treatment were excluded from this study.
Definitions and outcome measures
The primary outcome of the present study was the drugs prescribed for men newly diagnosed with BPH from 2012 to 2017, and the changes in the six-year prescription drug pattern in South Korea.
Statistical analysis
All statistical analyses were performed by statisticians using the statistical software SPSS version 20.0 (IBM, Armonk, NY, USA). All parameters are reported as frequency (percentage).
Ethics statement
The present study was approved by the Soonchunhyang University Seoul Hospital Institutional Review Board (IRB numbers: 2019-05-005) and followed the provisions of the Declaration of Helsinki (revised, Edinburgh 2000). This study was exempted from obtaining informed consent after IRB review.
Go to :
RESULTS
Number of drug prescriptions in men with BPH
Table 1 shows the number of prescription drugs for men first diagnosed with BPH (code N40) from 2012 to 2017 in HIRA-National Patient Sample (NPS) database. Alpha blockers were the most commonly prescribed drugs for men with BPH, and tamsulosin was the most common alpha blocker prescribed. Among the total prescribed drugs, the proportion of tamsulosin prescription steadily increased to 45.8% in 2012, 46.2% in 2013, 48.4% in 2014, 50.5% in 2015, 51.8% in 2016, and 54.0% in 2017. The number of 5ARI prescriptions increased gradually to 38.5% in 2012, 39.3% in 2013, 40.6% in 2014, 41.6% in 2015, 42.3% in 2016, and 43.3% in 2017. The proportion of finasteride prescription was the highest at 32.7% in 2015, but has been on a downward trend since then. However, the proportion of dutasteride prescriptions has increased steadily to 8.3% in 2014, 8.9% in 2015, 12.4% in 2016, and 14.1% in 2017. The number of ACH prescriptions increased, and then decreased when mirabegron began to be prescribed in 2015. The proportion of mirabegron prescriptions increased rapidly to 1.0% in 2015, 6.1% in 2016, and 9.0% in 2017.
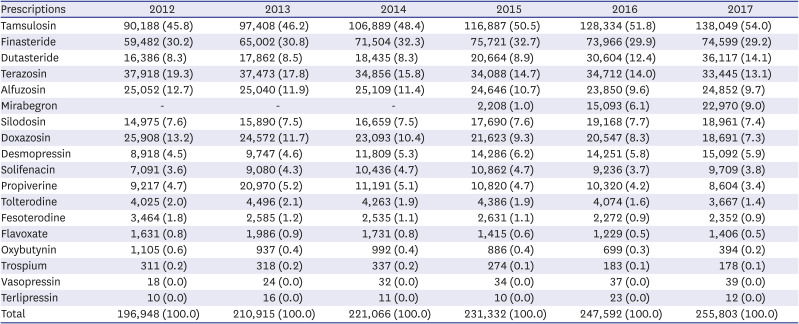
Table 1
Number of prescriptions by drug type from 2012 to 2017 for men with BPH (code N40) in Korea: HIRA-NPS database
Categorical variables as number (%).
BPH = benign prostatic hyperplasia, HIRA = Health Insurance Review and Assessment, NPS = National Patient Sample.
![]()
Prescription patterns by drug category in men with BPH
Table 2 presents the prescription patterns by drug category for men first diagnosed with BPH (code N40) from 2012 to 2017 based on the HIRA-NPS database. The proportion of alpha blocker monotherapies decreased steadily to 49.9% in 2012, 48.8% in 2013, 47.5% in 2014, 45.9% in 2015, 44.2% in 2016, and 42.5% in 2017. The number of combination therapy prescriptions of alpha blockers and 5ARIs remained similar from 2012 to 2017, while the combination of alpha blockers and ACHs increased from 7.0% in 2014 to 8.7% in 2017, and combination of alpha blockers + 5ARIs + ACHs increased steadily to 3.3% in 2012, 3.4% in 2013, 3.5% in 2014, 3.5% in 2015, 4.2% in 2016, and 4.8% in 2017.
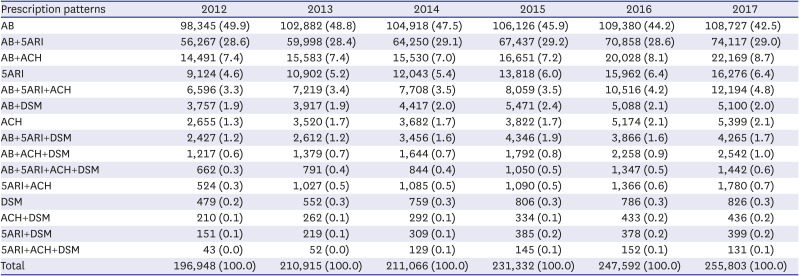
Table 2
Prescription patterns according to drug category from 2012 to 2017 for men with BPH (code N40) in Korea: HIRA-NPS database
Categorical variables as number (%).
BPH = benign prostatic hyperplasia, HIRA = Health Insurance Review and Assessment, NPS = National Patient Sample, AB = alpha-blocker, 5ARI = 5-alpha reductase inhibitor, ACH = anticholinergics, DSM = desmopressin.
![]()
Prescription patterns by drug ingredient in men with BPH
The prescription patterns by drug ingredient for men first diagnosed with BPH (code N40) from 2012 to 2017 in HIRA-NPS database is shown in Table 3. As for the number of prescriptions by drug ingredient, tamsulosin monotherapy was the most common, followed by combination of tamsulosin and finasteride, terazosin monotherapy, and combination of tamsulosin and dutasteride. The number of prescriptions involving the combination of tamsulosin and mirabegron increased steadily from 0.3% in 2015 to 1.7% in 2016 and 2.5% in 2017.
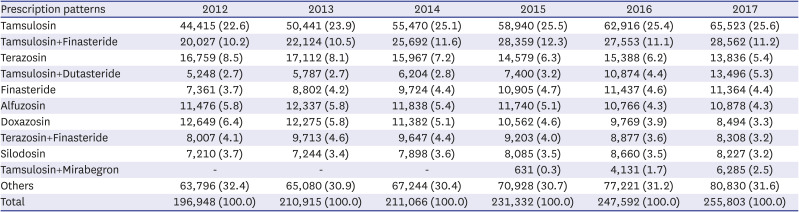
Table 3
Prescription patterns based on drug ingredients from 2012 to 2017 for men with BPH (code N40) in Korea: HIRA-NPS database
Categorical variables as number (%).
BPH = benign prostatic hyperplasia, HIRA = Health Insurance Review and Assessment, NPS, National Patient Sample.
![]()
Go to :
DISCUSSION
This study presents an overview of the patterns of drugs initially prescribed for men over 40 years of age diagnosed with LUTS/BPH in South Korea from 2012 to 2017 using the HIRA database. Similar to studies conducted in various regions such as the United States and Europe,910 the number of men newly diagnosed with LUTS/BPH each year in South Korea has steadily increased to 196,948 in 2012, 210,915 in 2013, 221,066 in 2014, 231,332 in 2015, 247,592 in 2016, and 255,803 in 2017 (Table 1). As the prevalence of LUTS/BPH increases with aging,1112 these results prove that Korean society is rapidly aging during the study period.
Alpha blockers were the most frequently prescribed drugs for men diagnosed with LUTS/BPH, of which tamsulosin was prescribed in about half of all patients, increasing every year: 45.8% in 2012, 46.2% in 2013, 48.4% in 2014, 50.5% in 2015, 51.8% in 2016, and 54.0% in 2017. Meanwhile, the next most prescribed alpha blockers were terazosin (from 19.3% in 2012 to 13.1% in 2017), alfuzosin (from 12.7% in 2012 to 9.7% in 2017) and doxazosin (from 13.2% in 2012 to 7.3% in 2017), and the prescription rates of these drugs steadily decreased every year during the survey period (Table 1). In this study, the high rate of alpha blocker prescriptions suggests that physicians in South Korea follow the guidelines for LUTS/BPH and is similar to studies conducted in the UK and the United States.3513
Based on the analysis of prescription patterns by drug category in this study, the most frequently prescribed drugs for men diagnosed with LUTS/BPH for the first time were alpha blockers, but the proportion of alpha blocker monotherapy steadily decreased, and the proportion of combination therapy of alpha blockers and 5ARI remained similar (approximately 29%) from 2012 to 2017 (Table 2). However, the proportion of combination therapy with alpha blockers and ACH (7.2% in 2015, 8.1% in 2016, and 8.7% in 2017) and alpha blockers, 5ARI, and ACH (3.5% in 2015, 4.2% in 2016, and 4.8% in 2017) has increased recently. A prospective study found that about half of men with bladder outlet obstruction (BOO) had overactive bladder (OAB). Alpha blocker monotherapy did not lead to sufficient improvement in 65% of men with symptomatic BOO and OAB. The addition of ACH improved symptoms in 73% of those who did not respond to alpha blocker monotherapy.14 A meta-analysis indicated that tamsulosin combined with solifenacin is superior to tamsulosin monotherapy against LUTS/BPH. The combination of tamsulosin and solifenacin rapidly decreased the total International Prostate Symptom Score (IPSS), Overactive Bladder Symptom Score (OABSS), and quality of life (QoL) scores during a short follow-up period (≤ 3 months) in patients with LUTS/BPH without increasing the risk of dysuria.15 Large randomized controlled trials suggest that the combination of an alpha blocker and an ACH is well tolerated and has significant efficacy in men with both voiding and storage LUTS.16171819
As the prescription of mirabegron in South Korea started in 2015, the proportion of mirabegron among drugs prescribed for men diagnosed with LUTS/BPH increased rapidly from 1.0% in 2015 to 9.0% in 2017 (Table 1). Based on the analysis of prescription patterns by drug ingredient, the proportion of combination therapies involving tamsulosin and mirabegron also increased to 0.3% in 2015, 1.7% in 2016, and 2.5% in 2017 (Table 3). A prospective study showed that mirabegron add-on therapy improved the total OABSS, IPSS, and IPSS-QoL scores in men with persistent LUTS on alpha blocker monotherapy.20 In a randomized controlled study, the combination of tamsulosin and mirabegron is safe and effective for men with BPH who manifests OAB symptoms after tamsulosin monotherapy.21 Recent data from a randomized, multicenter phase 3 study involving 1,794 patients with “wet” OAB symptoms for ≥ 3 months showed that the combination of mirabegron and solifenacin for OAB symptoms was well tolerated over 12 months and improved treatment efficacy compared with individual monotherapy.22 The results of several well-designed trials reported during the study period may have influenced the changes in the prescription patterns of Korean physicians in men diagnosed with LUTS/BPH.
The present study had some limitations. It was a retrospective, observational study. We extracted data involving only 3% of the national patient sample from the HIRA database. Therefore, this study did not include information on clinical findings such as severity of symptoms or prostate size. However, the HIRA database in South Korea contains the details of all medical services provided to almost all residents. Therefore, a 3% sample cohort of HIRA database provides useful information regarding prescription patterns in men diagnosed with LUTS/BPH in South Korea.
According to HIRA database, alpha blockers were the most commonly prescribed drugs for men first diagnosed with LUTS/BPH in Korea from 2012 to 2017, of which tamsulosin was the most common. Therapies such as alpha blocker plus 5ARI, and alpha blockers combined with 5ARIs and ACH are gradually increasing. Prescriptions of mirabegron have increased rapidly since their first use in 2015, replacing ACH.
Go to :
 XML Download
XML Download