

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic hepatitis B (CHB) has been identified as a major health problem since hepatitis B virus (HBV) was first identified in 1963 by Dr. Blumberg.1 It affects more than 350 million people worldwide and 1 million people each year die due to HBV associated cirrhosis and hepatocellular carcinoma (HCC).23 The primary target of HBV treatment is HBV DNA replication. Suppression of HBV DNA replication can inhibit the development and progression of cirrhosis, HCC development, and even prolongs the overall survival and transplantation-free survival among patients with CHB.456789
Currently, several kinds of nucleos(t)ide analogues (NAs) are recommended for the suppression of HBV DNA replication, such as entecavir (ETV), tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide. TDF shows strong effects by rapidly suppressing HBV DNA replication and normalizing alanine aminotransferase (ALT) like other NAs. In addition, TDF has several benefits compared to other NAs. First, it has no resistance-associated mutation during long-term treatment.910 Second, it is more effective in suppressing HCC development than ETV.11 Third, it can be used safely in pregnant women with CHB.910 Fourth, it can be used with food inintake.12 However, TDF can decrease bone mineral density, kidney function, and serum phosphate level.910
Tenofovir disoproxil orotate (DA-2802, Virreal®; Dong-A ST Co., Ltd., Seoul, Korea) as a new form of base change of TDF (Viread®; Gilead Sciences Inc., Foster City, CA, USA) is a novel salt formulation with improved physicochemical properties in terms of thermal stability and photostability. A phase I study showed that the pharmacokinetic of DA-2802 was similar to Viread®.13 This clinical trial was designed to compare the efficacy and safety of DA-2802 with those of Viread® in patient with CHB.
METHODS
Study design
The present study was a double blind randomized controlled clinical trial at phase III and registered at ClinicalTrials.gov (NCT02967939). Patients were recruited from 25 hospitals in Korea, stratified according to the status of hepatitis B envelop antigen (HBeAg), and given DA-2802 at a dose of 319 mg once daily or Viread® at a dose of 300 mg once daily for 48 weeks. Patients received drug and placebo simultaneously because the size of DA-2802 was smaller than that of Viread®. In fact, patients ingested the DA-2802 and placebo of Viread® or the placebo of DA-2802 and Viread® simultaneously.
The present study was designed by the sponsor (Dong-A ST Co., Ltd) and hepatologists working in university hospital.
Patients
The present study enrolled patients aged 18 years or more between March 2017 and January 2019. They had HBeAg-positive or HBeAg-negative CHB and compensated liver function. They were suffering from CHB for at least 6 months before screening and also had hepatitis B surface antigen (HBsAg)-positive at screening, HBV DNA level of ≥ 1 × 105 copies/mL in patients with HBeAg-positive or HBV DNA level of ≥ 104 copies/mL in patients with HBeAg-negative by commercial polymerase chain reaction (PCR) method at screening, serum ALT level ≥ 80 U/L to 10.0 times the upper limit of normal (ULN) in patients without liver cirrhosis or serum ALT level 1.0 to 10.0 times the ULN in patients with liver cirrhosis at screening. They had never received interferon alfa or antiviral agents against HBV for more than 12 weeks before participating in the present study and within 24 weeks before screening. Exclusion criteria included coinfection with hepatitis C, hepatitis D, or the human immunodeficiency virus; use of immunosuppressant or systemic corticosteroids for more than 4 weeks within 24 weeks before screening, decompensated liver function (total bilirubin > 2.5 mg/dL, prothrombin time ≥ 3 seconds over ULN, serum albumin < 3 g/dL, history of ascites, jaundice, variceal bleeding, hepatic encephalopathy, or other signs of hepatic dysfunction); creatinine clearance < 50 mL/min at screening, alpha-fetoprotein > 50 ng/mL at screening and suspected of having HCC based on results of relevant imaging tests, patients with malignant cancer, musculoskeletal diseases, pregnant women or breast feeding women, patients with alcohol use disorder or psychologic diseases.
Efficacy endpoints
The primary efficacy endpoint was the difference between HBV DNA level at week 48 and baseline. HBV DNA was measured by COBAS Taq-Man PCR assay (limit of detection ≥ 116 copies/mL). Secondary efficacy endpoints included the proportion of patients with undetectable HBV DNA level at week 24 and 48, the proportion of patients with normalized ALT at week 24 and 48, HBeAg loss or seroconversion at week 48, HBsAg loss or seroconversion at week 48, and resistant mutation in region of HBV polymerase.
Resistance surveillance
Serum from patients with virological breakthrough during treatment or with detectable HBV DNA ≥ 400 copies/mL at week 48 were examined for the detection of mutation in HBV polymerase-reverse-transcriptase region. Virological breakthrough was defined as 10 times increase of HBV DNA level (1 log10 copies/mL) compared to the lowest level of HBV DNA during treatment or detectable HBV DNA after complete virological response (< 116 copies/mL).
Safety analysis
The safety analyses included all patients who received at least one dose of a study drug and all events that occurred during treatment. Adverse events (AEs), serious AEs, laboratory abnormalities, discontinuation of the study drug due to AEs, and death were investigated. ALT flare during treatment was defined as elevations of ALT level to more than twice the baseline level and to more than 10 times the ULN, and the investigator considered findings clinically significant. Especially, serum phosphate, serum creatinine, and creatinine clearance (estimation of glomerular filtration rate, eGFR: [140 – age] × weight [kg] × 0.85 [if female]/72 × serum creatinine [mg/dL]) were evaluated to determine whether they had abnormal levels: serum phosphate < 2 mg/dL, serum creatinine increase from baseline ≥ 0.5 mg/dL, and eGFR < 50 mL/min. In addition, bone densitometry was undertaken at baseline and week 48 for the change of T score in spine and hip. The abnormal T score by bone densitometry was set when the score in either spine or hip decrease up to < −1 in patients who have T score ≥ −1 at baseline.
Statistical analysis
The planned sample size of 120 patients would provide a power of at least 90% and a significance level of 0.25 (one-sided) to test the noninferiority of DA-2802 compared to Viread® with a noninferiority margin of 1, assuming a standard deviation of 1.5 and 20% drop-out rate.
All statistical analyses were performed using the full analysis set which included all patients who had ingested the drug. Values are presented as mean ± standard deviation (SD) or number of patients (%). Two sample t-test (or Wilcoxon rank sum test) and paired t-test (or Wilcoxon signed rank test) were performed for continuous variables. χ2 test or Fisher’s exact test were performed for categorical variables.
The primary endpoint, the difference between HBV DNA level at baseline and week 48, was compared between groups by analysis of covariance (ANCOVA). The non-inferiority of DA-2802 to Viread® was evaluated by prespecified margin of 1. The primary endpoint according to HBeAg (positive/negative) status was compared between groups by nonparametric ANCOVA. The proportions of undetectable HBV DNA and ALT normalization were compared between the two groups using Cochran-Mantel-Haenszel test. If missing data occurred during the clinical trial in the full analysis set, the analysis was performed using the Last Observation Carried Forward (LOCF) method, which replaced missing data using the most recently obtained data based on the time of the missing data for subjects with efficacy endpoint measured at least once since baseline. Safety analyses included all patients who received at least one dose of a study drug and all events that occurred during treatment. For all statistical analyses, P < 0.05 was considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
The present study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was consistent with Good Clinical Practice guidelines. This study was approved by the Institutional Review Board (IRB) of Gachon University Gil Medical Center (IRB numbers: GAIRB2017-063) and the IRB of each participating hospital. Patients were centrally allocated and gave written informed consents in each hospital.
RESULTS
Study subjects
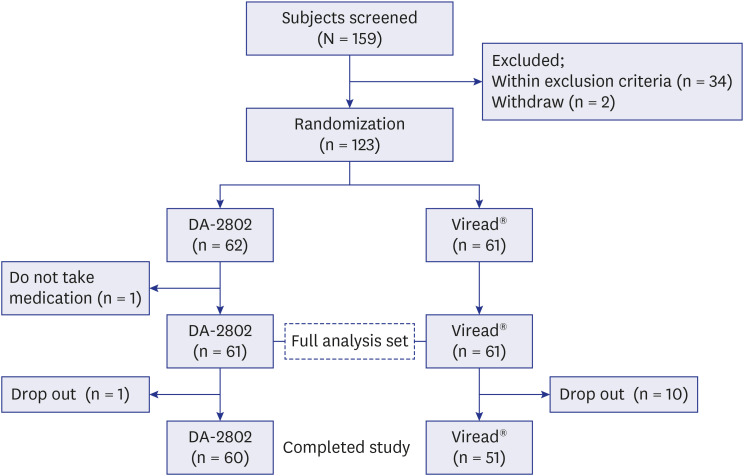
A total of 159 patients were screened for the present study. One hundred twenty-three of those patients were randomly allocated to each group at 1:1 (DA-2802 group: 62 patients, Viread® group: 61 patients). However, one of 123 patients did not ingest the drug. Therefore, 122 patients were used for the full analysis set (DA-2802 group:61 patients, Viread® group:61 patients) to determine the efficacy and safety of test drug. Eleven of 122 patients dropped out: 1 from DA-2802 group and 10 from Viread® group. Six, three, and two of those dropped out due to compliance, violation of study protocol, and prohibited medication, respectively. A total of 111 patients completed the present study (Fig. 1).
Fig. 1
Flow chart showing the enrollment of patients. Full analysis set consisted of 61 subjects in the DA-2802 group and 61 subjects in the Viread® group. Sixty subjects in the DA-2802 group and 51 subjects in the Viread® group completed the present study.
The mean age was 47 ± 11 years for the DA-2802 group and 48 ± 11 years for the Viread® group, showing no significant difference between the two groups. The proportion of male was 59.0% in the DA-2802 group and 68.9% in the Viread® group, showing no significant difference between the two groups. Except for serum phosphate levels, other laboratory data, virologic characteristics, spine T score, and hip T score were not different between the two groups either (Table 1).
Table 1
Demographic and baseline characteristics
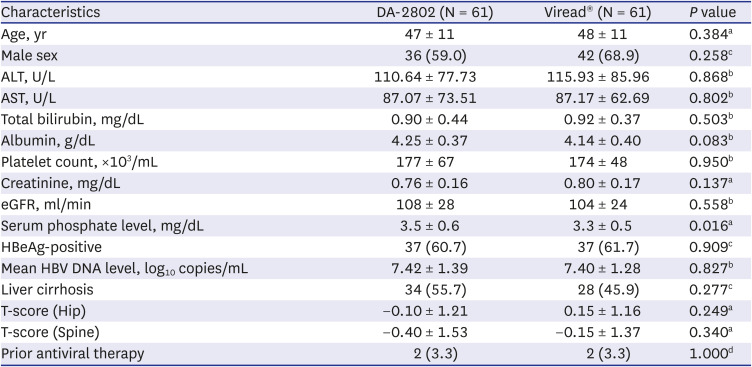
Data are expressed as mean ± standard deviation or number (%).
ALT = alanine aminotransferase, AST = aspartate aminotransferase, eGFR = estimation of glomerular filtration rate, HBeAg = hepatitis B envelop antigen, HBV = hepatitis B virus.
aTwo sample t-test, bWilcoxon rank sum test, cχ2 test, dFisher’s exact test.
Primary efficacy endpoint
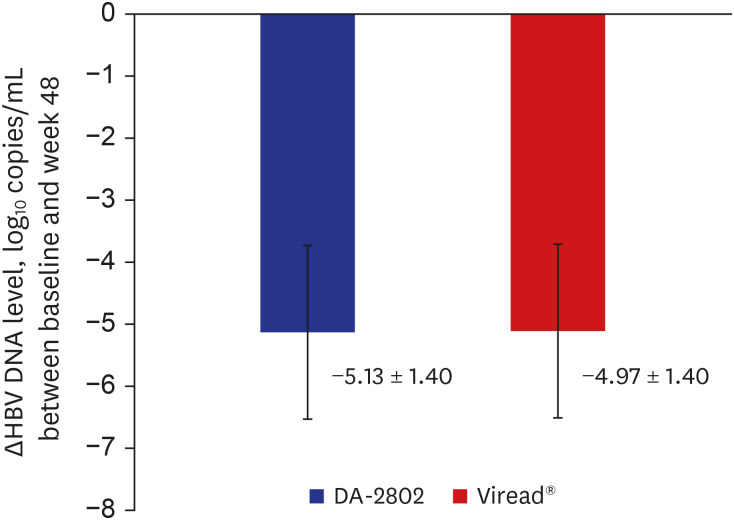
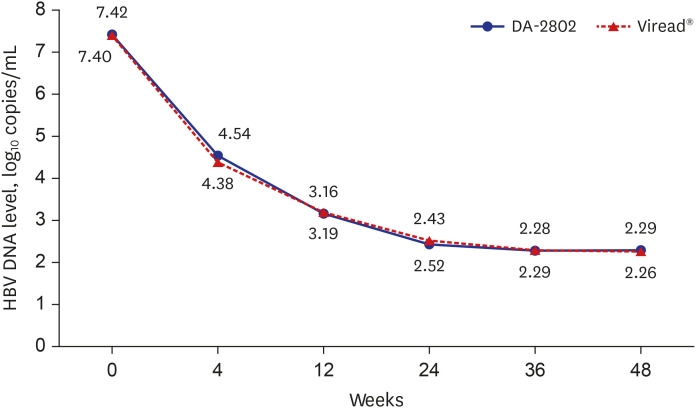
The mean HBV DNA level was significantly decreased from 7.42 ± 1.39 at baseline to 2.29 ± 0.60 log10 copies/mL at week 48 in the DA-2802 group (P < 0.001). The change of HBV DNA level was −5.13 ± 1.40 log10 copies/mL in the DA-2802 group. The mean HBV DNA level was also significantly decreased from 7.40 ± 1.28 at baseline to 2.43 ± 0.89 log10 copies/mL at week 48 in the Viread® group (P < 0.001). The change of HBV DNA level was −4.97 ± 1.40 log10 copies/mL in the Viread® group. As a result of nonparametric ANCOVA for primary endpoint, it was confirmed that DA-2802 was non-inferiority to Viread® (P < 0.001). In addition, the change in HBV DNA level at week 48 and the pattern of decreasing HBV DNA level according to the mean at each time point were presented (Figs. 2 and 3). Subgroup analysis according to positivity of HBeAg was done. The mean HBV DNA level was significantly decreased from 7.99 ± 0.98 at baseline to 2.44 ± 0.73 log10 copies/mL at week 48 in HBeAg positive-DA-2802 group (P < 0.001) and from 7.91 ± 1.08 at baseline to 2.46 ± 0.83 log10 copies/mL at week 48 in HBeAg positive- Viread® group (P < 0.001). The change of HBV DNA level was −5.55 ± 1.18 in the HBeAg positive-DA-2802 group and −5.44 ± 1.18 log10 copies/mL in the HBeAg positive-Viread® group. There was no difference in the change of HBV DNA level between the two groups (P = 0.711). The mean HBV DNA level was significantly decreased from 6.55 ± 1.49 at baseline to 2.06 ± 0.00 log10 copies/mL at week 48 in HBeAg negative-DA-2802 group (P < 0.001) and from 6.56 ± 1.16 at baseline to 2.36 ± 0.99 log10 copies/mL at week 48 in HBeAg negative- Viread® group (P < 0.001). The change of HBV DNA level was −4.48±1.49 in the HBeAg negative-DA-2802 group and −4.20±1.40 log10 copies/mL in the HBeAg negative-Viread® group. There was no difference in the change of HBV DNA level between the two groups (P = 0.509).
Secondary efficacy endpoints: the proportion of undetectable HBV DNA
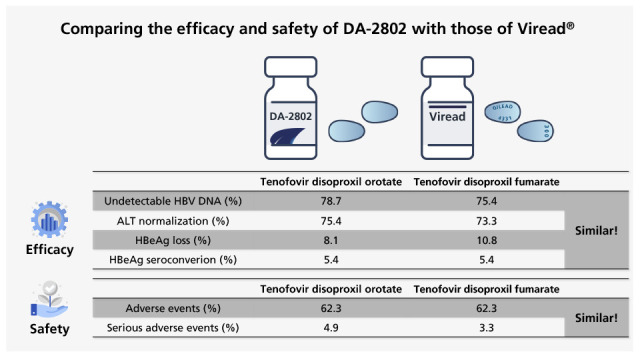
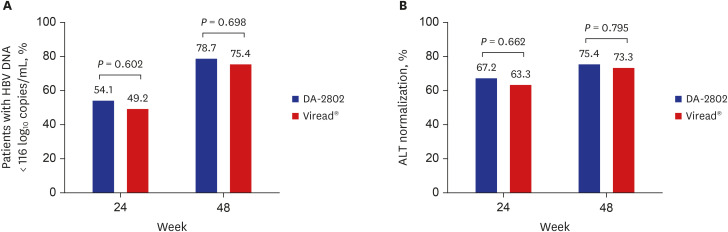
Proportions of undetectable HBV DNA at week 24 and 48 were 54.1% and 78.7% in the DA-2802 group and 49.2% and 75.4% in the Viread® group, respectively. There was no difference in the proportion of undetectable HBV DNA at week 24 (P = 0.602) and 48 (P = 0.698) between the two groups (Fig. 4A).
Secondary efficacy endpoints: the proportion of ALT normalization
The mean ALT level was significantly decreased from 110.64 ± 77.73 at baseline to 32.16 ± 15.17 U/L at week 48 in the DA-2802 group (P < 0.001) and from 115.93 ± 85.96 at baseline to 35.38 ± 20.16 U/L at week 48 in the Viread® group (P < 0.001). Proportions of ALT normalization at week 24 and 48 were 67.2% and 75.4% in the DA-2802 group and 63.3% and 73.3% in the Viread® group, respectively. There was no difference in the proportion of ALT normalization at week 24 (P = 0.662) and 48 (P = 0.795) between the two groups (Fig. 4B).
Secondary efficacy endpoints: serologic response
The rate of HBeAg loss at week 48 was 8.1% (3/37) in the DA-2802 group and 10.8% (4/37) in the Viread® group (P = 1.000). The rate of HBeAg seroconversion at week 48 was 5.4% (2/37) in the DA-2802 group and 5.4% (2/37) in the Viread® group (P = 1.000). There was no HBsAg loss or seroconversion at week 48 in any patient.
Secondary efficacy endpoints: virological breakthrough and resistance surveillance
There were 3 cases of virological breakthrough: 1 in the DA-2802 group and 2 in the Viread® group. Two patients among them had undetectable HBV DNA until week 36. However, HBV DNA level in the DA-2802 group and in the Viread® group increased to 530,784 and 178,092 log10 copies/mL at week 48, respectively. The later patient had a problem of compliance. Those 2 patients were subjected to genotyping for detecting substitutions of polymerase-reverse transcriptase. They did not have genotypic substitution associated with decreased sensitivity to tenofovir. They were treated with Viread® according to protocol after completing the study. However, they were not followed up further because the present study was not allowed to take more data after completing study. Another 1 patient in the Viread® group had undetectable HBV DNA until week 12. However, HBV DNA level was increased to 151 log10 copies/mL at week 24. It was then undetectable at week 36 and 48.
Twenty-two of 122 patients (DA-2802 group: 11 patients, Viread® group: 11 patients) with detectable HBV DNA ≥ 400 copies/mL at week 48 were subjected to genotyping for detecting substitutions of polymerase-reverse transcriptase at week 48. There was no genotypic substitution associated with decreased sensitivity to tenofovir among these patients who received DA-2802 or Viread®.
Comparing changes of T score, creatinine, eGFR, and serum phosphate level between DA-2802 and Viread® groups
The mean hip T score significantly decreased from −0.10 ± 1.21 at baseline to −0.27 ± 1.26 at week 48 in the DA-2802 group (P < 0.001) and from 0.15 ± 1.16 at baseline to −0.01 ± 1.15 at week 48 in the Viread® group (P < 0.001). The decrease of hip T score was −0.18 ± 0.41 in the DA-2802 group and −0.16 ± 0.38 in the Viread® group (P = 0.968, Fig. 5A). The mean spine T score significantly decreased from −0.40 ± 1.53 at baseline to −0.60 ± 1.55 at week 48 in the DA-2802 group (P < 0.001) and from −0.15 ± 1.37 at baseline to −0.33 ± 1.30 at week 48 in the Viread® group (P < 0.001). The decrease of spine T score was −0.19 ± 0.31 in DA-2802 group and −0.15 ± 0.36 in Viread® group (P = 0.377, Fig. 5B). Among 51 patients in the DA-2802 group and 51 patients in the Viread® group whose T scores of the hip or spine at baseline were −1 or greater, the number of patients who had T score in hip or spine < −1 at week 48 were 9 (17.6%) in the DA-2802 group and 5 (9.8%) in the Viread® group (P = 0.250). Only 1 patient in the DA-2802 group had a hip T score ≤ −2.5 at week 48.
Fig. 5
Comparing the change of (A) Hip T score, (B) Spine T score, (C) Creatinine, (D) eGFR, and (E) Serum phosphate level.
eGFR = estimation of glomerular filtration rate.
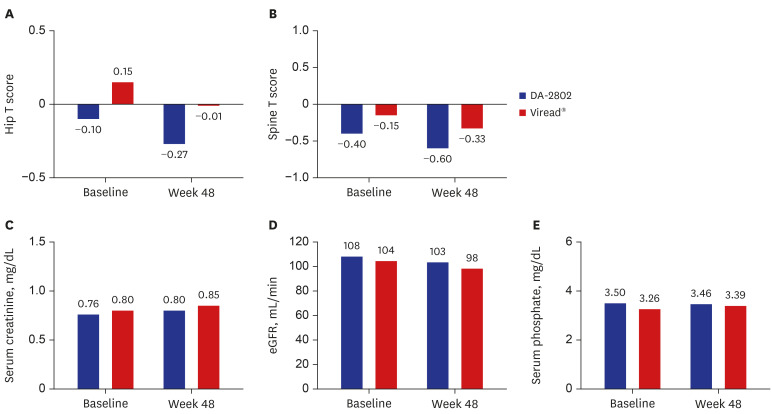
The mean creatinine level was significantly increased from 0.76 ± 0.16 at baseline to 0.80 ± 0.17 mg/dL at week 48 in the DA-2802 group (P = 0.001) and from 0.80 ± 0.17 at baseline to 0.85 ± 0.15 mg/dL at week 48 in the Viread® group (P < 0.001). There was no difference in the increase of creatinine level between the two groups (P = 0.734, Fig. 5C). The mean eGFR significantly decreased from 108 ± 28 at baseline to 103 ± 30 mL/min at week 48 in the DA-2802 group (P = 0.003) and from 104 ± 24 at baseline to 98 ± 25 mL/min at week 48 in the Viread® group (P = 0.002). There was no difference in the decrease of eGFR between the two groups (P = 0.840, Fig. 5D). The number of patients with eGFR below 50 ml/min was 2 in the DA-2802 group and 1 in the Viread® group during treatment. However, no patients in either group showed increase of serum creatinine level ≥ 0.5 mg/dL compared to baseline serum creatinine level. One patient in the DA-2802 group and one patient in the Viread® group had eGFR of 44 and 45 mL/min at week 48, respectively. One patient in the DA-2802 group had eGFR of 49 mL/min at week 12 and 78 mL/min at week 48. However, these 3 patients did not discontinue medication during treatment.
The mean serum phosphate level changed from 3.50 ± 0.59 at baseline to 3.46 ± 0.60 mg/dL at week 48 in the DA-2802 group (P = 0.586) and from 3.26 ± 0.50 at baseline to 3.39 ± 0.55 mg/dL at week 48 in the Viread® group (P = 0.082, Fig. 5E) No patients showed serum phosphate level below 2.0 mg/dL.
Safety and AEs in DA-2802 and Viread® groups
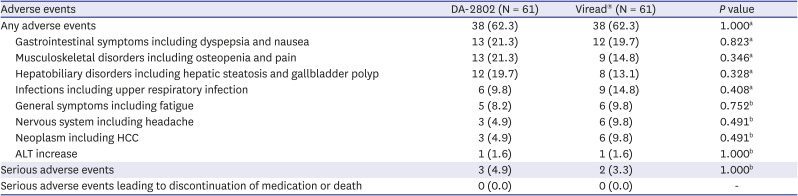
Safety and AEs were investigated in 122 patients (Table 2). The frequency of AEs during treatment was similar between the two groups. Frequent AEs were dyspepsia, nausea, osteopenia, hepatic steatosis, and viral upper respiratory tract infection. Most AEs were mild to moderate in severity. Serious AEs occurred in 4 patients (2 patients in the DA-2802 group and 2 patients in the Viread® group). One case of dacryocystitis and one case of spinal column stenosis occurred in the DA-2802 group. One case of clavicular fracture and one case of pericarditis constrictive occurred in the Viread® group. Those serious AEs were not related to the study drug. They were improved by proper management and did not need discontinuation of the study drug. ALT flare during treatment occurred in 1 patient in the Viread® group. The ALT increased from 169 at baseline to 401 U/L at week 3, but decreased to normal level at week 12 without discontinuation of the study drug.
Table 2
Clinical adverse events and laboratory abnormalities
DISCUSSION
TDF has strong effect on natural course of patients with CHB by inhibiting HBV replication. It can normalize ALT, increase HBeAg or HBsAg loss, and improve histologic features.91415 Furthermore, it can improve survival and quality of life by preventing disease progression and HCC development.91617 In the full analysis set, DA-2802 reduced serum HBV DNA level similar to Viread® after dosing. In addition, DA-2802 increased the proportion of patients with undetectable HBV DNA at week 24 and 48. It was comparable to Viread®. DA-2802 also increased the proportion of patients who showed loss of HBeAg at week 48 similar to Viread®. Although the duration of time was not enough to investigate HBsAg loss, DA-2802 is anticipated to have the same effect as Viread®.
A total of 111 patients who completed the present study were analyzed for per protocol analysis (PPA, DA-2802 group: 60 patients; Viread® group: 51 patients) to aid the result of full analysis set (data not shown). The change of HBV DNA level was −5.11 ± 1.40 log10 copies/mL in the DA-2802 group. The change of HBV DNA level was −5.27 ± 1.22 log10 copies/mL in the Viread® group. Proportions of undetectable HBV DNA at week 24 and 48 were 55.0% and 80.0% in the DA-2802 group and 54.9% and 82.4% in the Viread® group, respectively. Proportions of ALT normalization at week 24 and 48 were 66.7% and 75.0% in the DA-2802 group and 62.7% and 76.5% in the Viread® group, respectively. The rate of HBeAg loss at week 48 was 8.3% (3/36) in the DA-2802 group and 9.4% (3/32) in the Viread® group. The rate of HBeAg seroconversion at week 48 was 5.6% (2/36) in the DA-2802 group and 6.3% (2/32) in the Viread® group. This PPA showed the same results with the full analysis set in terms of primary and secondary efficacy end points. In the aspect of other clinical responses such as histologic improvement, preventing disease progression and HCC development, DA-2802 is anticipated to have the same long-term effects as Viread®. However, further long-term studies are needed to clarify those issues.
The ULN of serum ALT has been considered to be 40 U/L.18 However, this level was set before the finding of hepatitis C virus and understanding of nonalcoholic fatty liver disease.1920 Accordingly, several reports have suggested that the ULN for serum ALT should be adjusted to 30–34 U/L for male and 19–25 U/L for female.21222324 In addition, an expert panel recommended that a serum ALT level lower than 40 U/L should be used for decision making to treat patients with CHB.25 As a matter of fact, American Association for the Study of Liver Disease (AASLD) recommended that ULN of ALT is 35 U/L for men and 25 U/L for women.10 Although the present study used the ULN of ALT in each clinical trial institutions, we further analyzed the ULN of ALT according to AASLD guideline (data not shown). Proportions of ALT normalization at week 24 and 48 were 39.3% and 55.7% in the DA-2802 group and 43.3% and 53.3% in the Viread® group, respectively. There was no difference in the proportion of ALT normalization at week 24 and 48 between the two groups.
The development of drug resistance mutations is one of the major problems during long-term therapy with NAs. Although a few cases of resistance mutants for TDF have been reported,2627 significant resistance mutation after 7 years of treatment has not been identified.1428 DA-2802 showed no resistant mutation during treatment. Although one patient in the DA-2802 group showed breakthrough, the cause of breakthrough might be due to compliance. In addition, genotyping to detect substitutions of polymerase-reverse transcriptase showed no genotypic substitution among patients who had HBV DNA > 400 copies/mL at week 48.
TDF can induce some problems in glomerular kidney function. Increase of serum creatinine level and decline of eGFR have been reported in patients treated with TDF.91629 Therefore, European Association for the Study of the Liver (EASL) guideline recommends that all CHB patients treated with TDF therapy should be monitored to watch out for adverse renal effects with serum creatinine and eGFR. In addition, patients who develop eGFR < 60 mL/min need close renal monitoring. Furthermore, patients with renal alteration such as eGFR < 60 mL/min or albuminuria > 30 mg or hemodialysis should select other NAs over TDF.9 DA-2802 also increased serum creatinine level and decreased eGFR like as Viread®. Therefore, serum creatinine level and eGFR should be monitored in patients treated with DA-2802.
TDF can induce another problem of tubular kidney function that decreases serum phosphate level and bone mineral density.916283031 Cases of Fanconi syndrome have been reported after treatment with TDF.3233 In addition, declines in bone mineral density at the hip and spine have been reported in patients treated with TDF.31 EASL guideline recommends that serum phosphate level should be closely monitored if patients show serum phosphate level < 2 mg/dL. Furthermore, patients with possible bone disease such as chronic steroid use or use of other medication that can worsen bone density, a history of fragility fracture, osteoporosis, and low phosphate (< 2.5 mg/dL) should select other NAs over TDF.9 Both DA-2802 and Viread® did not decrease serum phosphate levels in the present study. However, DA-2802 decreased bone mineral density at the hip and spine after only 48 weeks of treatment like as Viread®. Although serum phosphate level was not decreased in the DA-2802 group and Viread® group, bone mineral density was deteriorated in both groups. Therefore, bone mineral density should be monitored in patients treated with DA-2802.
DA-2802 was well tolerated in patients with CHB up to week 48 without discontinuation of medication due to adverse effects. There were no severe AEs associated with DA-2802. However, there are still concerns about the deterioration of renal function and the decrease of bone mineral density after treatment with DA-2802, similar to those after treatment with TDF.
The present study had a few limitations. First, the present study had a short-term administration of DA-2802. To investigate the long-term effect of DA-2802, further studies, including post marketing survey, are needed. Second, short term administration of DA-2802 was not enough to investigate its AEs on kidney and bone. Therefore, markers for renal dysfunction and demineralization of bone should be checked regularly for long-term periods in future studies. In addition, new guidelines that clearly guide physicians to avoid or stop the medication are needed.
In conclusion, results of the present study demonstrate that DA-2802 is not inferior to Viread® in terms of efficacy or safety. Therefore, DA-2802 can be used in the same way as TDF for patients with CHB.
 XML Download
XML Download