

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A healthy parent-child relationship is especially important in families of children with attention deficit hyperactivity disorder (ADHD), because it affects ADHD prognosis with respect to symptom severity, treatment compliance, and impact on comorbidities.12 Parents of children with ADHD must play an active role as auxiliary therapists in pharmacological and behavioral treatments to improve the prognosis of children with ADHD.1 Therefore, good parent-child relationships are essential in families with a child with ADHD and should be investigated further.
Parents with children with ADHD experience higher levels of parenting stress and parent-child conflict than those with typically developing children.34567 This could be because parents of children with ADHD experience a high level of frustration in managing their children’s problematic behaviors, such as less compliance with parents’ requests and demands, increased distraction, demands for attention, and requiring more assistance than typically developing children.8910 Parenting stress negatively influences children through several pathways, including poor monitoring of children’s behaviors and emotions, increased punishment, a less supportive attitude, and increased conflict in parent–child relationships.1112
Parenting stress is also associated with parents’ mental health.613 Parental depression is associated with distorted perceptions and negative cognitions, which makes it difficult for such parents to objectively evaluate their children’s behavior and communicate effectively.14 When parents have anxiety or mood problems, children with ADHD display more impulsivity and hyperactivity than their counterparts with healthy parents.1516 Considering that ADHD is inherited, it is possible that parental ADHD symptoms are contributing factors to parenting stress and negatively affect family functioning.617 Parental ADHD symptoms have been associated with both harsh and lax parenting.18 The negative cycle is apparent in these family relationships, whereby children with ADHD negatively affect their parents’ mental health, and parents’ mental pathology leads to increased conflict with children, the development of negative parent–child interactions, and children’s behavioral problems.313 Therefore, clinicians should aim to accurately assess the mental health of parents of children with ADHD while simultaneously assessing and providing therapy to the children.
Parenting stress and its impacts on mental health in fathers of children with ADHD has been studied, albeit less so than the mental health of mothers of children with ADHD.19202122232425 Compared with the fathers with typically developing children, fathers of children with ADHD have been reported to feel more deficient and have greater dissatisfaction in their role as a parent.6102225 Families of children with ADHD experience a lot of marital conflict, and this in turn can have adverse effects on parental mental health and parenting stress.2627 In turn, parental depression increases marital conflict and negatively affects children’s mental health, either directly or indirectly.2728 Much like the reciprocal relationship between children with ADHD and parental mental health, mothers’ mental health affects fathers’ mental health negatively or positively, and fathers’ mental health also affects mothers’ mental health. In the context of fathers’ increasing participation in parenting, some studies have highlighted the importance of fathers’ mental health in parenting.22 It is thus necessary to examine the relationship between mothers’ and fathers’ mental health, such as depression and anxiety, and their parenting stress.
Parenting stress differs between cultures.2930 For example, one study revealed that Korean mothers reported significantly higher parenting stress but fewer behavioral problems among their children than American mothers.29 Additionally, a cross-cultural study that examined 31 cultures using a child behavior checklist revealed differences in the mean scale scores across cultures.30 However, research is still lacking with regard to the cross-cultural differences that could affect parenting stress. Specifically, few studies have examined fathers’ parenting in East Asian countries; this gap is particularly important to address given the cultural differences in paternal roles in Eastern and Western cultures.293132 The paternal parenting role in South Korea has changed dramatically with modernization and the increasing participation of women in the workforce. The employment rate of married women has increased from 9.3% in the 1960s to 47.7% in 2019.32 However, Confucianism has had significant philosophical and ethical influences on Korean society since the 14th century, including different gender roles for fathers and mothers in parenting.3132 Namely mothers take on most of the parenting responsibilities, and fathers are often emotionally distant from their children and maintain a position of authority and respect. Therefore, maternal and paternal parenting stress associated with raising children with ADHD in South Korea may differ from those observed in Western societies.
Parents of children with ADHD experience more parenting stress than parents with typically developing children, and more parenting stress if the parent has depressive symptoms and/or anxiety. In South Korea, the mother is primarily responsible for child-rearing, so it is expected that mothers of children with ADHD experience more parenting stress than fathers; furthermore, mothers’ mental health may in turn harms fathers’ mental health. Thus, we examined parenting stress and parents’ mental health in mothers and fathers of children with ADHD in South Korea. We hypothesized that 1) children’s ADHD symptoms would be negatively related to maternal and paternal mental health, and 2) parents’ mental health and parenting stress would be reciprocally related.
Go to : 
METHODS
Participants
This cross-sectional study was conducted with children and their parents who visited our outpatient service from January 1, 2018 to December 31, 2019. Children diagnosed with ADHD according to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) and their parents participated in this study.33 Their parents were heterosexual and had been living together after marriage. Children who had a history of head injury, neurological disorder, severe medical disease, or whose primary diagnosis did not have ADHD according to DSM-5 were excluded from this study. Finally, 70 children with ADHD and their parents (70 mothers and 70 fathers) participated in this study. The demographic information of participants is described in the Results section.
Instruments
Korean ADHD Rating Scale-IV (K-ARS-IV)
The K-ARS-IV is an 18-item measure that assesses the ADHD diagnostic criteria of the DSM-IV and was completed by the child’s mother and father to evaluate symptom severity of children with ADHD.34 Each item is rated on a 4-point Likert scale (0–3) according to the frequency of the child’s problematic behavior. It is designed such that the total score of odd-numbered items measures inattention, and the total score of even-numbered items measures hyperactivity-impulsivity. A total score ≥ 19 indicates clinically significant ADHD symptoms.35 In the K-ARS-IV standardized by Jang et al.35 the Cronbach’s alpha was 0.74−1, and the validity was 0.06−0.59. In this study, the Cronbach’s alpha was 0.93.
Child Depression Inventory (CDI)
The CDI was developed by Kovacs.36 It assesses the cognitive, emotional, and behavioral symptoms of childhood and adolescent depression. In the present study, mother and father completed this for children aged 6–10 years, and adolescents aged 11–18 years completed it by themselves. The CDI was used to evaluate depression among children with ADHD. Depression is a common comorbidity of ADHD and can affect the level of parenting stress.3738 The CDI consists of 27 items; each item is rated on a 3-point Likert scale (0–2) based on respondents’ mood state. A total score ≥ 22 indicates a clinically significant depressive symptom.39 In the Korean version of the CDI, standardized by Cho and Lee,39 the Cronbach’s alpha was 0.88, and the correlation was strong, with a test-retest reliability of 0.82. In this study, the Cronbach’s alpha was 0.92.
Adult ADHD Self-Report Scale (ASRS)
The ASRS is a self-report measure that assesses adults’ ADHD symptoms, and was completed by the mother and father of children with ADHD. The ASRS consists of two parts (Parts A and B). Part A is composed of six questions; checking four or more darkly shaded boxes is likely to be the most sensitive predictor of adult ADHD symptoms.40 We assessed ADHD symptoms of parents using Part A. However, all parents checked fewer than four darkly shaded boxes in Part A, which indicated that they were unlikely to have ADHD symptoms. Part B is composed of 12 items; each item is evaluated on a 5-point Likert scale (0–4).41 A combined ASRS score (after adding the scores of parts A and B) higher than 31 is defined as the 50th percentile.42 The Korean version of the ASRS has a good sensitivity and specificity.43 In this study, the Cronbach’s alpha of the ASRS was 0.89 and 0.90 among fathers and mothers respectively.
State-Anxiety Inventory (SAI)/State-Anxiety Inventory for Children (SAI-C)
The SAI, which was developed by Spielberger et al.44 is a self-report test that assesses state anxiety in adults. The SAI is sensitive to transient anxiety in adults. The SAI-C was adapted from the SAI for adults to ensure that the instrument is easily understood by children and adolescents.45 In the present study, mother and father completed the SAI-C on behalf of children aged 6–11 years, and adolescents aged 12–18 years old completed it by themselves. Both the SAI and SAI-C comprise 20 items that are rated on a 4-point Likert scale (1–4) or a 3-point Likert scale (1–3), respectively. Higher total scores indicate higher anxiety levels.4647 The Korean version of the SAI-C was standardized by Cho and Lee40 and its Cronbach’s alpha was 0.88. The Korean version of the SAI was standardized by Han et al.47 and its Cronbach’s alpha was 0.93. In this study, the Cronbach’s alphas of the SAI-C were 0.95. The Cronbach’s alpha of the SAI among fathers and mothers was 0.94 and 0.95 respectively.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a self-report assessment to evaluate and determine the severity of depression in primary mental health clinics.48 The PHQ-9 was used to assess depressive symptom of mothers and fathers, who completed the measure themselves. The PHQ-9 consists of 9 items, which are each rated on a 4-point Likert scale (0–3). A total score ≥ 5 indicates depression.49 In the Korean version of the PHQ-9, the Cronbach’s alpha was 0.85, and the sensitivity and specificity were 0.82 and 0.90, respectively.49 In this study, the Cronbach’s alpha among fathers and mothers was 0.78 and 0.84 respectively.
Parental Stress Scale (PSS)
The PSS is a self-report assessment that evaluates parenting-relevant emotions and perceived role satisfaction, regardless of the sex of the parents or the presence or absence of emotional/behavioral problems in their children.50 In the present study, both mothers and fathers completed the PSS. The PSS consists of 18 items that are rated on a 5-point Likert scale (1–5). Parental role satisfaction (items 1, 2, 5, 6, 7, 8, 17, and 18) are reverse scored. Higher total scores indicate higher levels of parental stress. In this study, the Cronbach’s alpha among fathers and mothers was 0.89 and 0.88 respectively.
Statistical analysis
We used IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA). First, we conducted descriptive statistics to confirm participants’ demographic data, such as children’s sex, age, and mental health; and parents’ age, education, job, marital status, and mental health. Job and education differences between mothers and fathers were confirmed using χ2 tests, and differences in the ASRS, SAI, PHQ-9, and PSS scores between mother and fathers were confirmed using two-sample t-tests. Second, we used Pearson’s product-moment correlation to examine the association between the K-ARS-IV scores of children and the SAI, PHQ-9, and PSS scores of their parents. Finally, we used the SPSS INDIRECT MACRO version 3.4 a multiple regression procedure—to test for the mediation effects of maternal state anxiety (mediation assessment by model 4 in process) and depressive symptoms (moderated mediation assessment by model 14 in process) in the relationship between children’s ADHD symptoms and fathers’ parenting stress.51 We then used the bootstrapping method to test the significance of the indirect effect using 5,000 bootstrap samples and 95% confidence intervals.52 Confidence intervals that did not include zero were considered significant.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of the Soonchunhyang University Seoul Hospital (No. 2017-08-003). All participants voluntarily participated and provided written informed consent.
Go to :
RESULTS
Demographic data of children with ADHD and their parents
Children’s demographic characteristics are shown in Table 1. The mean age of children with ADHD was 10.84 years (standard deviation = 3.59 years), and there were 51 boys (72.9%) and 19 girls (27.1%). The children showed no evidence of clinically significant depressive symptoms and anxiety. Fathers were significantly older and more likely to be employed than mothers. The ADHD symptom severity of all parents fell below 31, indicating that none of the parents had clinically significant adult ADHD. However, mothers showed significantly higher parenting stress than fathers (Table 2).
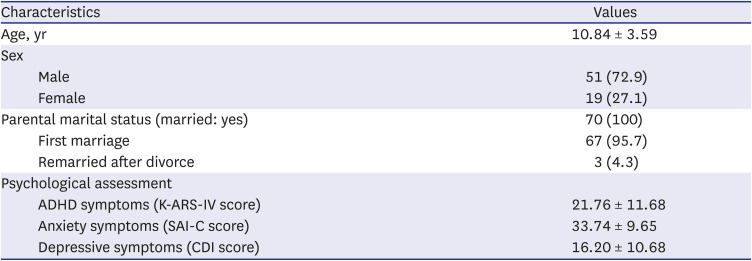
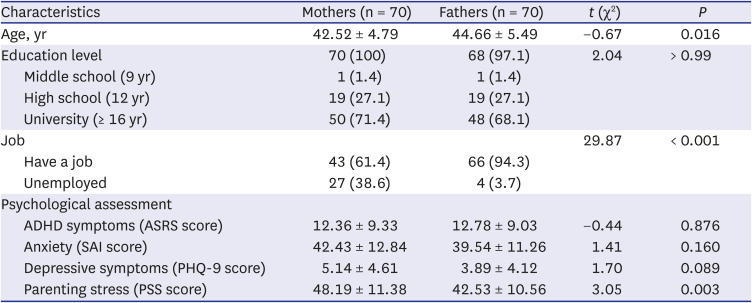
Table 1
Children’s demographic and psychological characteristics (N = 70)
Values are expressed as mean ± standard deviation or number (%).
ADHD = attention deficit hyperactivity disorder, K-ARS-IV = Korean ADHD Rating Scale-IV, SAI-C = State-Anxiety Inventory for Children, CDI = Child Depression Inventory.
![]()
Table 2
Comparisons of characteristics between mothers and fathers of children with ADHD (N = 140)
Values are expressed as mean ± standard deviation or number (%).
ADHD = attention deficit hyperactivity disorder, ASRS = Adult ADHD Self-Report Scale, SAI = State-Anxiety Inventory, PHQ-9 = Patient Health Questionnaire-9, PSS = Parental Stress Scale.
*P < 0.05, **P < 0.01.
![]()
Correlation analyses of ADHD symptoms of children and parental mental health and parenting stress
We used Pearson’s product-moment correlation to examine the association between children’s ADHD symptoms (K-ARS-IV scores), and parents’ anxiety (SAI scores), depressive symptom (PHQ-9 scores), and parental stress (PSS scores).
Table 3 displays the bivariate correlations of the variables included in the hypothetical model. First, children’s ADHD symptoms had a weak positive linear correlation with mothers’ anxiety. Children’s ADHD symptom scores were not correlated with mothers’ depressive symptoms or parenting stress or with fathers’ anxiety, depressive symptoms, or parenting stress. Second, mothers’ anxiety displayed a strong positive linear correlation with mothers’ parenting stress and depressive symptoms as well as a weak positive linear relationship with fathers’ parenting stress. However, mothers’ anxiety was not correlated with fathers’ anxiety and depressive symptoms. Fathers’ anxiety displayed a strong positive linear correlation with fathers’ depressive symptoms and a moderate positive linear correlation with fathers’ parenting stress.

Table 3
Correlation coefficients between the study variables (N = 210)
![]()
Moderated mediation models examining the relationship between ADHD symptoms of children, maternal anxiety, and paternal parenting stress
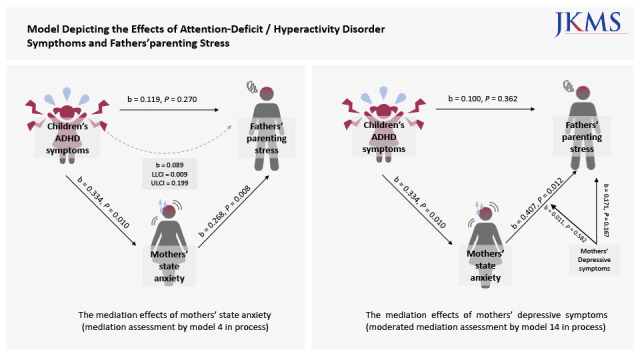
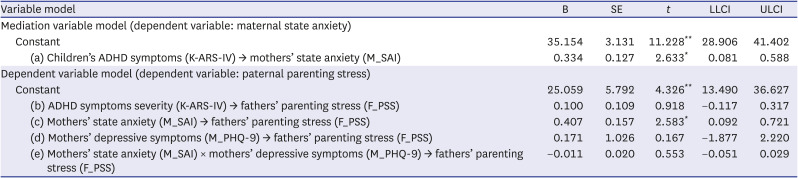
As shown in Table 4, the indirect effect analysis showed that maternal state anxiety fully mediated the effects of children’s ADHD symptoms on paternal parenting stress, whereby paths (a) and (c) were both significant; however, Path (b) was not significant. In the bootstrap analysis, the indirect effects were significant. In other words, although children’s ADHD symptoms had no direct effect on paternal parenting stress, they might increase mothers’ state anxiety, which contributes to fathers’ parenting stress (Fig. 1).
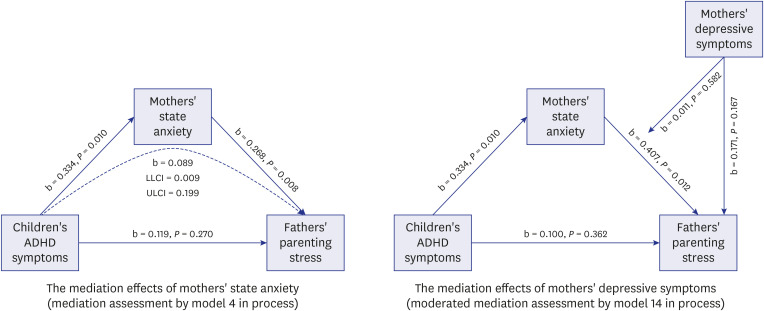 | Fig. 1Model depicting the effects of ADHD symptoms and fathers’ parenting stress.ADHD = attention deficit hyperactivity disorder.
*P < 0.05, **P < 0.01.
|
Table 4
Bootstrapping results of the mediation model examining the effects of maternal state anxiety on the relationship between adolescents’ ADHD symptoms and fathers’ parenting stress and the moderated mediation model of maternal depressive symptoms (N = 210)
SE = standard error, LLCI = lower limit within 95% confidence interval of boot indirect effect, ULCI = upper limit within 95% confidence interval of boot indirect effect, K-ARS-IV = Korean ADHD Rating Scale-IV, SAI = State-Anxiety Inventory, PHQ-9 = Patient Health Questionnaire-9, PSS = Parental Stress Scale, M = mothers, F = fathers.
*P < 0.05, **P < 0.01.
![]()
The interaction effects of maternal state anxiety and maternal depressive symptoms were not significantly related to paternal parenting stress, and the moderating effect of maternal depressive symptoms on the relationship between maternal state anxiety and paternal parenting stress was not significant (Table 4). However, as shown in Table 5, when examining the conditional indirect effects (children’s ADHD symptoms → maternal state anxiety → paternal parenting stress) of maternal depressive symptoms on maternal state anxiety, the maternal depression score was significant, at 4 and 10 points. Therefore, the conditional indirect effects of mothers’ depression were significant when the maternal depression score was > 4.

Table 5
Mathers’ depressive symptoms for conditional indirect effects of children’s ADHD symptoms on fathers’ parenting stress
| Mothers’ depressive symptoms (M_PHQ9) | Effect | Boot SE | LLCI | ULCI |
|---|---|---|---|---|
| 0 | 0.136 | 0.085 | −0.007 | 0.324 |
| 4 | 0.121 | 0.064 | 0.010 | 0.260 |
| 10 | 0.099 | 0.055 | 0.002 | 0.216 |
SE = standard error, LLCI = lower limit within 95% confidence interval of boot indirect effect, ULCI = upper limit within 95% confidence interval of boot indirect effect, PHQ-9 = Patient Health Questionnaire-9, M = mothers.
![]()
Go to :
DISCUSSION
In this study, we examined the relationship between ADHD symptoms of children and the mental health of their parents in South Korea. ADHD symptoms of children were significantly related to maternal anxiety, but not with paternal mental health. Maternal anxiety was significantly related to paternal parenting stress. The key results of this study are as follows: 1) mothers of children with ADHD experienced more parenting stress than fathers, 2) children’s ADHD symptoms were significantly positively correlated with their mothers’ state anxiety, and 3) the mediation model showed that maternal state anxiety fully mediated the path from children’s ADHD symptoms to paternal parenting stress.
One noteworthy finding of the present study is that mothers of children with ADHD experienced more parenting stress than fathers. While most previous parenting stress studies have only evaluated mothers of children with ADHD,6 our results support those of previous studies that have compared parenting stress between mothers and fathers.8535455 Mothers might experience more parenting stress than fathers because they have a greater responsibility for raising children,5455 which is also reportedly the case for dual-income couples.53 However, fathers of children with ADHD have been reported to experience greater role dissatisfaction than fathers with typically developing children.56 Parenting is generally affected by marital relationships; however, the quality of paternal parenting is more affected by marital relationships than is the quality of maternal parenting.115657 In addition, mothers’ state anxiety is related to maternal depression, and maternal depression is known to increase marital conflict.58 Future research should examine the relationship between these factors by examining whether marital conflict and marital life satisfaction can affect parenting stress of fathers and mothers.
Children’s ADHD symptoms were significantly positively correlated with mothers’ state anxiety. Previous studies have consistently reported similar results—that having children with ADHD is associated with an increased incidence of maternal anxiety.245960 Children with ADHD display more noncompliance and inappropriate behaviors than typically developing children.61 Mothers of children with ADHD must exert a great deal of effort to correct their children’s problem behaviors and compensate for their lack of emotion self-regulation.1961 Eventually, these mothers may experience a decrease in parental efficacy, an increase in psychological burden, and heightened levels of anxiety and stress. Previous studies have reported raising children with ADHD is related to depression in mothers;61321 however, we did not find this result. In this study, the mean K-ARS-IV score, a measure of severity of ADHD in children, was slightly higher than the clinically significant cut-off score. Thus, the milder severity of children’s symptoms may explain our contrasting results. To accurately identify the factors, a systematic study with a larger sample size is required.
The mediation model showed that mothers’ state anxiety fully mediated the path from children’s ADHD symptoms to fathers’ parenting stress. The moderated mediation effect of maternal depressive symptoms on the relationship between maternal state anxiety and paternal parenting stress was non-significant; however, the conditional indirect effect of depressive symptoms was significant, at PHQ-9 score more than 4. This bidirectionality indicates that paternal parenting stress is affected by mothers’ mental health. It is possible that maternal anxiety increases paternal parenting stress through various pathways. First, it could be related to social support. Social support is a protective factor for the mental health of parents of children with ADHD, as it leads to greater maternal satisfaction, lower maternal stress, and reduced marital conflict.1025 However, parents of children with ADHD participate less in social activities, and have fewer interactions with extended family members, than do other parents.62 Mothers of children with ADHD might look to their spouses for social support, which could explain why fathers’ parenting stress was affected through maternal anxiety and depressive symptoms. Second, it is possible that maternal anxiety caused marital conflict to increase, which increased fathers’ parenting stress.115657 Third, cross-cultural differences may exist. As noted, Korean mothers may face increased psychological burden owing to the social stigma related to rearing children with a disability, as well as their increased responsibility of care under the Confucian tradition.2963 Additionally, it is possible that Korean fathers feel less responsible for parenting than their Western counterparts; thus, they may have been more affected by the mothers’ anxiety than the symptoms of their children with ADHD.
The present study has some limitations. First, this was a cross-sectional study; therefore, we cannot confirm causal relationships. Second, tool objectivity is lacking since all mental health evaluations were self-reported. In particular, the total score of the K-ARS-IV may vary depending on who among the parents evaluated it. Therefore, caution is required in interpreting the results. Third, ADHD symptoms, anxiety, and depressive symptoms among the participants were typically mild; therefore, the results cannot be generalized to those with more severe symptoms. Fourth, sample representativeness is lacking because of selection bias. Participants were limited to those recruited at one hospital in South Korea. Fifth, there is a lack of consideration for other intrafamilial factors that can affect parenting stress, such as the number of children raised, other comorbidities of children, and social economic status. In future studies, these factors should be supplemented. Additionally, to clearly understand the characteristics of parenting stress for parents of children with ADHD in South Korea, future work should directly compare parenting stress of parents of children with ADHD in other countries.
Despite these limitations, our results offer important insights on the mediation effect of maternal state anxiety on the relationship between the symptoms of children with ADHD and paternal parenting stress. This study confirmed the importance of the mental health of mothers of children with ADHD and the interaction with familial health. Assessment and treatment of children with ADHD should include not only the children, but also their parents. These family-based interventions could be an effective strategy for ADHD treatment. Prospective follow-up studies are necessary to confirm the causal relationships and additional related factors concerning the mental health of mothers and fathers of children with ADHD.
Go to :
 XML Download
XML Download