

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pancreaticoduodenectomy (PD) is accompanied with high mortality and morbidity rates. There has been a lot of effort over the past century to overcome postoperative complications, and mortality rate has decreased due to improved surgical techniques. However, complications such as postoperative pancreatic fistula (POPF) remain a challenge even in a high-volume center. Diameter of pancreatic duct, texture of pancreas, comorbidity of the patients, and nutritional status, are known as risk factors for POPF [123]. These factors are uncorrectable characteristics of patients; thus the need for investigations for correctable risk factors. Recently, some studies showed that restrictive fluid administration during the intra- and postoperative periods can improve surgical outcomes [456789]. Based on these reports, the Enhanced Recovery After Surgery guidelines for perioperative care for PD also recommended avoidance of fluid overload [10]. However, the lack of the definition of restrictive or liberal administration of fluid among the studies so far reported remains an important problem to be solved.
In addition to these reports, large-scale studies including the reports of the New England Journal of Medicine also underlined the importance of restrictive fluid administration. However, these studies included a wide variety of abdominal surgeries such as urology, gynecology, and colorectal operations [111213]. Unlike the surgeries so far studied in previous reports, PD requires a long surgical time and aggressive lymphadenectomy having a higher risk of bleeding compared to other surgeries. Thus, studies investigating the proper amount of fluid balance focusing on PD exclusively are needed.
From the surgeon’s perspective, intraoperative fluid administration also may be an uncorrectable factor since anesthesiologists are in charge of fluid management during the operation. Furthermore, there are few studies regarding the effect of postoperative fluid balance on the surgical outcome. This study aims to determine the relationship between postoperative fluid balance and surgical outcome after open PD.
METHODS
This study has been approved by the Institutional Review Board of Kyungpook National University Chilgok Hospital (No. KNUCH 2021-07-008). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Patient
We collected data from 172 patients who underwent open PD including pylorus-preserving PD (PPPD), hepatopancreaticoduodenectomy (HPD), and Whipple’s operation from 2015 to 2019 at a single institution, analyzed retrospectively. We excluded any patients who underwent laparoscopic or robotic PD, patients with co-resection of other organs or hemodialysis. Data on intra- and postoperative fluid administration were obtained from anesthesiology and surgical records. For pancreaticojejunostomy, the inverted mattress method invaginating the pancreas stump into the lumen of jejunum in the end-to-side fashion was utilized for all patients. No one received octreotide during perioperative management. Two closed suction drains were placed at hepaticojejunostomy and pancreaticojejunostomy.
Study variables
Characteristics of patients
Data collected on patient demographics are age, sex, body mass index (BMI), comorbidities, and American Society of Anesthesiologist physical status classification. Diagnosis was categorized into pancreas cancer, ampulla of Vater cancer, Bile duct cancer, and duodenal cancer based on pathology report. Cases of surgery with metastases of hepatocellular carcinoma, renal cell carcinoma, and esophageal cancer were classified as others. Surgical types include PPPD, HPD, and Whipple’s operation.
Perioperative parameter
The parameters of intraoperative fluid are the amount (mL/hr/kg) and the type (crystalloid, colloid, and blood) of fluid. Intraoperative fluid balance is calculated as the difference between the total amount of administered fluid and discharge such as estimated blood loss and urine output. We also recorded operative time (minutes). The postoperative period includes from the immediate postoperative period to the 2nd day after surgery. The parameters of postoperative fluid are the amount of administered fluid (mL/kg) and transfusion during the day of surgery, the 1st day, and the 2nd day after surgery respectively. Postoperative fluid balance is calculated as the difference between the administered fluid and output. The output includes the volume of urine, nasogastric tube, and discharge in abdominal drainage tube.
Surgical outcome parameter
POPF, delayed gastric emptying (DGE), and postpancreatic hemorrhage (PPH) follows the definition of the International Study Group Pancreatic Surgery [141516]. In this study, only POPF greater than grade B was classified as a complication after PD. Abdominal abscess is defined as the image study showing localized fluid retention with sign of infection requiring antibiotics or drainage procedure. We diagnosed wound infection when wound accompanied erythema, secretion, or need of re-suture. Through checking drain color or bilirubin level in the drain, bile leak is categorized. Cardiopulmonary complications include myocardial infarction, arrhythmia, pneumonia, pulmonary thromboembolism and, pleural effusion requiring intervention procedure. The other surgical outcome parameters are Clavien-Dindo classification [17] and hospitalization-day.
Statistical analysis
The statistical analysis of the study was performed using IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA). To compare the effect of postoperative fluid balance on surgical outcome, we divided it into 2 groups; high group and low group by median value. In each group, the Student t-test and Mann-Whitney U-test were used to compare continuous parameters, while categorical variables were tested with the chi-square test and Fisher exact test. An additional analysis was performed to identify factors associated with POPF. A logistic regression analysis was used with variables that show difference between POPF group and non-POPF group. High BMI and male sex variables known to be associated with POPF [12] were also used in the univariate analysis. Significant parameters (P < 0.1) in univariate analysis were added to a multivariate analysis to determine risk factors for POPF. Results are reported as odds ratio (OR) and 95% confidence intervals (CIs) of statistical significance was accepted at a level of P < 0.05.
RESULTS
Demographic and clinical features of the entire patients
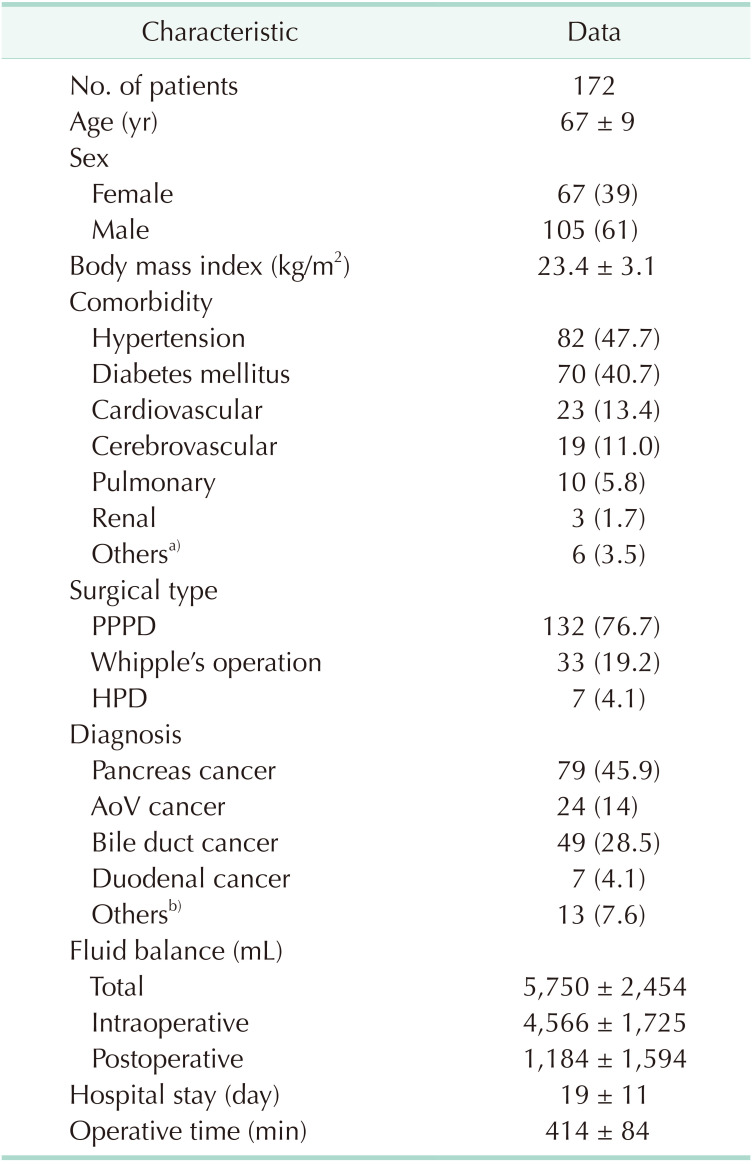
One hundred seventy-two patients were registered in this study and demographic characteristics of the patients are shown in Table 1. Mean age was 67 ± 9 years and 105 patients (61.0%) were male. One hundred thirty-two patients (76.7%) underwent PPPD, 33 patients (19.2%) underwent Whipple’s operation, and 7 patients underwent HPD. The most common diseases were pancreatic cancer (n = 79, 45.9%), followed by bile duct cancer (n = 49, 28.5%), ampullary cancer (n = 24, 14%), and duodenal cancer (n = 7, 4.1%). The mean volume of total fluid balance was 5,750 ± 2,454 mL. The average amount of intra- and postoperative fluid balance were 4,566 ± 1,725 mL and 1,184 ± 1,594mL, respectively. The patients were hospitalized for an average of 19 ± 11 days. Mean operative time was 414 ± 84 minutes.
Comparison of clinical features between high- and low-balance groups
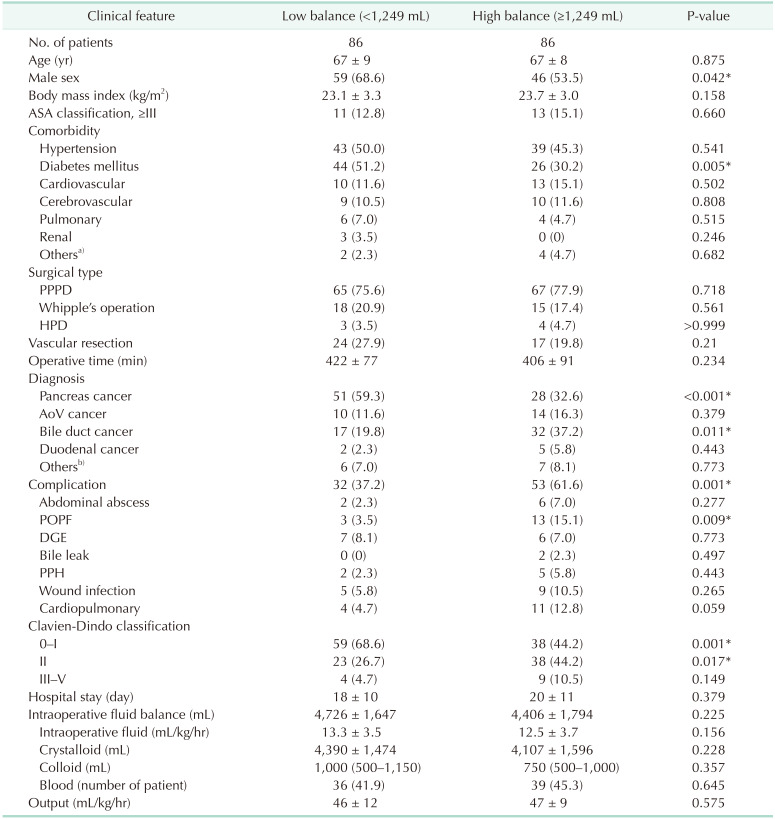
We divided the patients into 2 groups, high-balance and low-balance groups according to the amount of fluid balance until 2 days after surgery (Table 2). The low-balance group had more male (n = 59, 68.6% vs. n = 46, 53.5%; P = 0.042) and diabetes mellitus patients (n = 44, 51.2% vs. n = 26, 30.2%; P = 0.005). High-balance group has a higher number of complications in total (n = 53, 61.6% vs. n = 32, 37.2%; P = 0.001). Especially, the incidence of POPF rate was higher in high-balance group (n = 13, 15.1% vs. n = 3, 3.5%; P = 0.009). The patients in high-balance group also had more grade 2 of Clavien-Dindo classification complications (n = 38, 44.2% vs. n = 23, 26.7%; P = 0.017). In the intraoperative parameters, all variables including rate of fluid administration, type of fluid, and transfusion did not differ between the 2 groups.
Comparison of clinical features between patients with POPF and without POPF
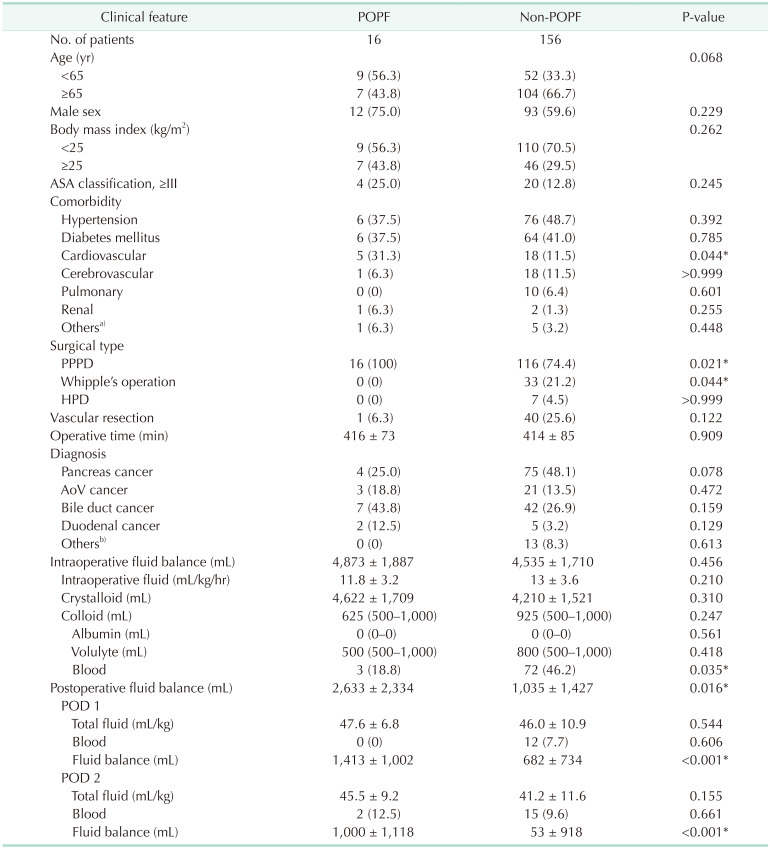
The incidence of POPF was 9.3% (n = 16). The patients with POPF were accompanied by more cardiovascular disease (P = 0.044). All patients with POPF underwent PPPD (P = 0.021). The postoperative fluid balance was associated with the presence of POPF (P = 0.016) (Table 3).
The risk factors associated with POPF by multivariate analysis
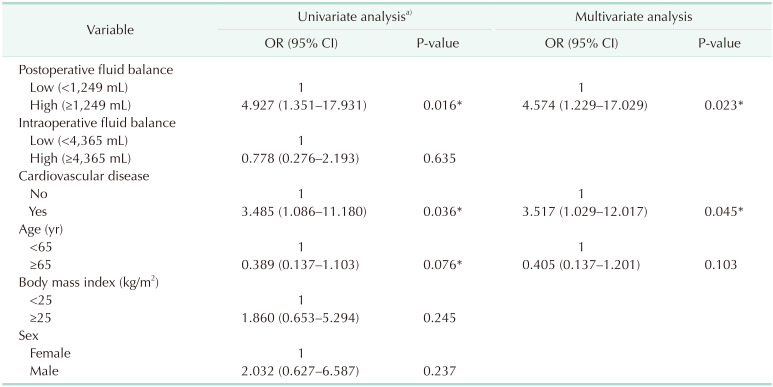
Using the median value of intra- and postoperative fluid balance as a criterion, the patients were divided into high and low groups (Table 4). Although no significant difference of values was shown in comparison between the patients with and without POPF, BMI, and male sex variables which are reported to be associated with POPF in other studies [12] were also performed in the univariate analysis.
On univariate analysis, high postoperative fluid balance, age under 65, and the presence of cardiovascular disease were associated with POPF (P < 0.1).
These factors were analyzed in multiple logistic regression models. On multivariate analysis, high postoperative fluid balance was identified as a risk factor for POPF (OR, 4.574; 95% CI, 1.229–17.029; P = 0.023). The presence of cardiovascular disease also had an increased rate of POPF (OR, 3.517; 95% CI, 1.209–12.017; P = 0.045). However, age was not related to the occurrence of POPF.
DISCUSSION
PD is major abdominal surgery with considerable risk of mortalities and morbidities. There have been many attempts to minimize postoperative complications. However, most efforts were limited to surgical techniques such as methods of anastomosis [1819]. In an era when surgical skills have advanced, it is necessary to find other factors that may affect surgical outcome. One of the crucial complications after PD is POPF, which can be antecedent for DGE or PPH. Risk factors of POPF were known as diameter of pancreatic duct, texture of pancreas, sex, BMI [12] and these causes are uncorrectable characteristics in patients. It is important to identify other correctable factors that affect postoperative complications and modify postoperative management. Recently, various studies reported fluid administrations are associated with surgical outcome in abdominal surgery [111213]. The basis for the idea that fluid can be related to surgical outcome is that fluid overload may cause pulmonary edema and the consequent deoxygenation of tissues can delay wound healing. In the same mechanism, fluid overload also can cause bowel edema which can cause disruption of intestinal anastomosis. On the other hand, fluid restriction can reduce tissue perfusion, which may lead to ischemia of the anastomosis. In RELIEF (REstrictive Versus LIbEral Fluid Therapy in Major Abdominal Surgery) clinical trial [12], the study compared surgical outcomes between restrictive and liberal fluid regimen during and up to 24 hours after the surgery. There were no differences except the occurrence of acute kidney injury. A drawback of this study is that this trial included a wide variety of esophageal, gastric, hepatobiliary, and colorectal, urologic, gynecologic surgery. Generally, it is well known that hepatobiliary pancreatic surgery has a higher risk of bleeding than other abdominal surgeries because it requires a long operation time and aggressive lymphadenectomy. Therefore, research on specific organs is needed to determine the exact effect of fluid on organ-specific surgical outcomes. Additionally, both laparoscopic and open surgery were registered in this study. In cases of open surgery, there is a lot of evaporation of body fluid, which increases the insensible loss of fluid compared to laparoscopic approach.
Shen et al. [11] reported meta-analysis on comparison of restrictive or liberal fluid regimen. The 16 studies included in this analysis compared the surgical complications between 2 groups during operation day or 24 hours after surgery of different abdominal organ resections. The meta-analysis showed that there was no significant difference in the rate of postoperative complications between the 2 groups. However, they reported that when analyzing subgroups divided based on weight gain, the complications increased in higher the weight gain subgroup of restrictive fluid. In clinical practice, even if same amount of fluid is administered, the accumulated fluid status can be different. It could be interpreted that fluid balance may be more important than how much the fluid is administered. These reports that studied the relationship between fluid management and surgical outcome have several confusing points. First, since the definition of restrictive fluids varies in each institution, a restrictive fluid group classified in one study can be defined as a liberal fluid group in another. Furthermore, each study investigated the duration of fluid administration differently. Most studies have focused on the intraoperative period or up to 24 hours after surgery. Our study is a retrospective study of patients with open PD only. We investigated fluid balance from the immediate postoperative period to 2 days after surgery. Anesthesiologists are in charge of intraoperative fluid administration and it is difficult for surgeons to make decisions regarding fluid management during surgery. In addition, since several anesthesiologists make subjective decisions as to estimated blood loss during surgery, there is a high possibility of bias. Thus, we considered intraoperative fluid management as also an uncorrectable factor as with characteristics of patients. Our study found that higher postoperative fluid balance has more complications, especially POPF. In view of the Clavien-Dindo classification, only grade 2 complications were associated with the high balance of fluid. However, grade 3 to 5 complications were not associated with postoperative fluid balance. The variable of intraoperative fluid including volume, type, and balance state had no difference between POPF and non-POPF. Multivariate analysis revealed the high postoperative fluid balance and the presence of cardiovascular disease are risk factors of POPF. The possible mechanism of the association between cardiovascular disease and POPF may be that the patient with cardiovascular disease may have fluid overloading due to inadequate cardiac output, which may cause POPF. The wound healing stage of intestinal anastomosis consists of inflammatory phase, proliferative phase, and remodeling phase. In early postoperative period, inflammatory phase may be prevalent. In this period, anastomosis strength determined by preexisting collagen in the submucosa layer may be weak. Intestinal anastomoses strength will remain weak for 2–3 days until new collagen is synthesized after surgery [20]. Thus, the possibility of wound failure increases, and fluid overload can exacerbate this risk through swelling of the submucosal layer. Since the third day after surgery is usually the diuretic phase and most patients are already on a diet, from this time intravascular fluid administration is reduced. This is the reason we selected the period of investigation from postoperation to 2 days after surgery. Among studies aimed at identifying a relationship between intraoperative fluid administration and postoperative outcomes, some reports showed association [4679] while others did not [212223]. The reason for these different results may be related with the fact that anastomosis healing takes place over a postoperative period, not at any point during the surgery. Therefore, we may conclude that postoperative fluid management is important for better surgical outcome. The limitation of this study is that it is a retrospective study and included a relatively small number of patients. Additionally, the number of postoperative complications is small. Despite these limitations, our study showed that high postoperative fluid balance increased the incidence of POPF. However, further randomized prospective controlled studies to investigate the proper amount of fluid balance are required.
In conclusion, high postoperative fluid balance and the presence of cardiovascular disease are associated with POPF. Thus, efforts are required to avoid volume overloading due to high fluid balance in postoperative management.
 XML Download
XML Download