

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Currently, the standard treatment of locally advanced rectal cancer consists of neoadjuvant chemoradiotherapy and total mesorectal excision (TME) [1]. About 30% of patients develop treatment failure after this multidisciplinary approach [12]. Immune checkpoint inhibitors, such as programmed death 1 (PD-1)/programmed death-ligand 1 (PD-L1) antibodies, have recently been incorporated in treatment regimens for some gastrointestinal malignancies including locally advanced rectal cancer [34]. A meta-analysis of PD-L1 indicated that PD-L1 did not appear useful as a prognostic marker for rectal cancer [5]. As the combined positive score (CPS) is adopted for gastric and gastroesophageal junction cancer, the role of CPS for rectal cancer should be evaluated.
Systemic inflammation including elevated serum proinflammatory cytokines and acute-phase proteins levels is an indicator of poor prognosis for rectal cancer. Many markers of systemic inflammation include ratios, or scores of acute-phase proteins or circulating white cells, such as Glasgow prognostic score (GPS) determined by serum CRP and albumin [67]. In tumor microenvironments, immune cells could produce cytokines and chemokines. However, the relationship between local immune response and systemic inflammation is controversial [6]. During the course of azoxymethane (AOM)/dextran sulfate sodium (DSS)-induced colitis and colitis-associated colorectal cancer, upregulation of PD-L1 throughout the AOM/DSS regime was observed and upregulation of PD-1 expression on mucosal T-cell subsets of the colon and the ileum correlated with disease progression [8]. The aim of the present study was to investigate the association of GPS, CPS, and clinicopathological characteristics of locally advanced rectal cancer.
Go to : 
METHODS
This study was approved by the independent ethics committee of Zhejiang Cancer Hospital (No. IRB-2020-15). It was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Patients
Between February 2012 and February 2018, 108 patients with locally advanced rectal cancer treated by neoadjuvant chemoradiotherapy and TME were retrospectively evaluated. Of these 108 patients, 5 were excluded from the present analysis for limited rectal biopsy specimens. Pelvic intensity-modulated radiotherapy (IMRT) consisted of 45–50.4 gray (Gy) in 25–28 fractions at 1.8–2.0 Gy per daily fraction. Capecitabine or capecitabine plus oxaliplatin was given concurrently with pelvic IMRT excluding 2 old-age patients. TME was performed 6 to 8 weeks after completion of neoadjuvant chemoradiotherapy. Adjuvant capecitabine-based chemotherapy was used at the discretion of the attending physicians of the individual patients. All patients were staged by the 8th edition of the American Joint Committee on Cancer (AJCC) staging system. The system is used to grade tumor response after neoadjuvant chemoradiotherapy as recommended by the AJCC Cancer Staging Manual, 8th edition.
Definition of Glasgow prognostic score
Blood samples were drawn and assayed within 2 weeks before neoadjuvant chemoradiotherapy. Based on a previous study, the GPS was determined as follows: patients with neither elevated CRP level (>10 mg/dL) nor hypoalbuminemia (<3.5 g/dL) were classified as a score of 0, and patients developing 1 or both of these blood chemistry abnormalities were classified as a score of 1 or 2, respectively.
Immunohistochemistry
Immunohistochemistry (IHC) of 5-µm sections from formalin-fixed paraffin-embedded tissue of rectal biopsy specimens was performed with PD-L1 (Clone MIH1, dilution of 1:50; eBioscience, San Diego, CA, USA). H&E sections were also reviewed for the presence of tumors. Each section was evaluated by 2 experienced pathologists according to the CPS (PD-L1-stained tumor cells and immune cells/total number of viable tumor cells × 100) in rectal biopsy specimens prior to neoadjuvant chemoradiotherapy [9].
Statistical analysis
Statistical analysis was carried out using IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA). The disease-free survival (DFS) and overall survival (OS) were measured from the 1st day of neoadjuvant chemoradiotherapy to the date of the event and were estimated by use of the Kaplan-Meier method. The chi-square test, t-test, and Fisher exact tests were used to compare the differences between the GPS-low and the GPS-high group. Multivariate analyses with the Cox proportional hazards model were used to test independent significance by using backward elimination of insignificant explanatory variables. Host factors (age and sex) were included as covariates in all tests. Statistical tests were based on a two-sided significance level. A P-value of <0.05 indicated statistical significance.
Go to :
RESULTS
General information
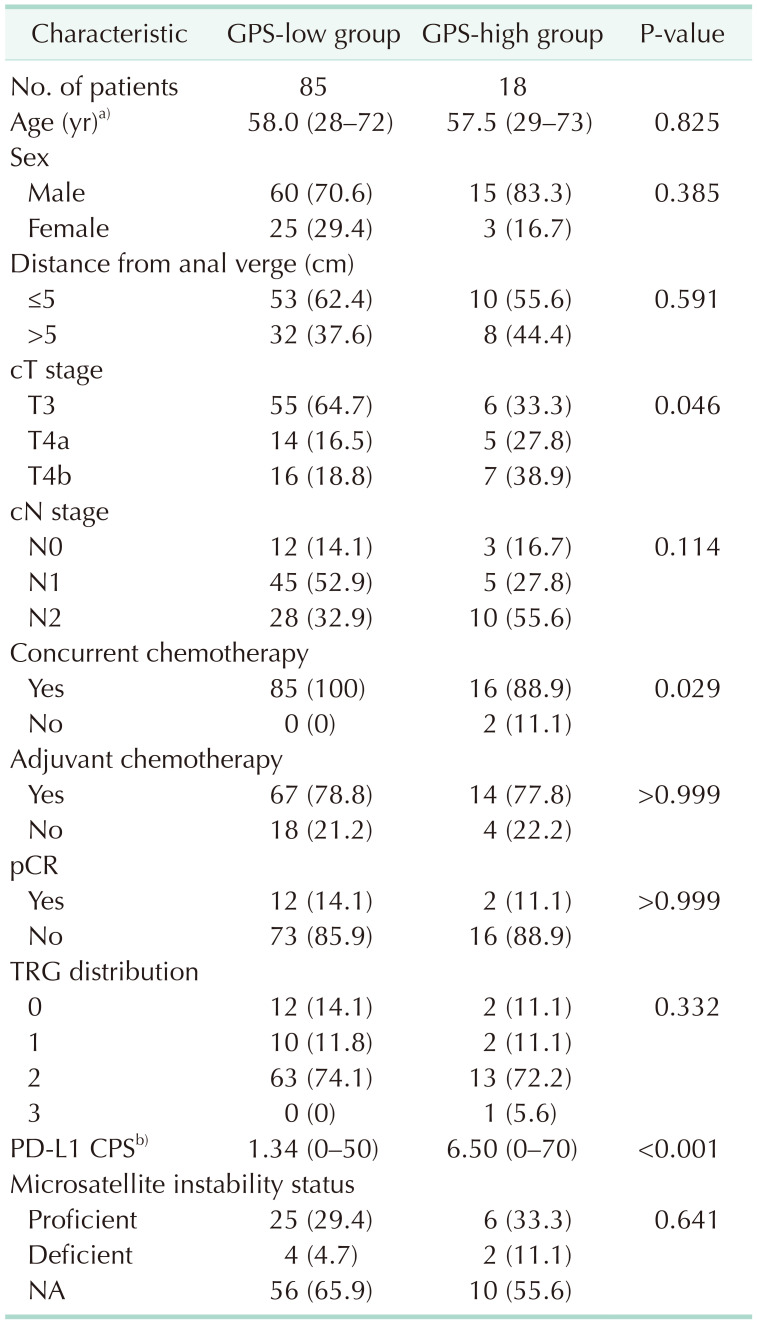
A total of 103 locally advanced rectal cancer patients were included. According to the classification of the GPS, 85 (82.5%), 13 (12.6%), and 5 patients (4.9%) were classified as having a score of 0, 1, and 2, respectively. Patients were classified into the GPS-low group (GPS of 0, n = 85) and GPS-high group (GPS of 1 or 2, n = 18) with an area under the curve of 0.582 for OS. The details of the microsatellite instabilities for 66 patients (64.1%) were not available. For the 37 patients with data of microsatellite instabilities status, no significant difference was observed in terms of microsatellite instability status between the GPS-high and GPS-low groups (P = 0.591). The clinical characteristics of the patients in the GPS-low and GPS-high groups are listed in Table 1.
Association between Glasgow prognostic score and combined positive score
The mean PD-L1 CPS of the whole group was 2.24 (range, 0–70). The representative IHC staining of PD-L1 in locally advanced rectal cancer biopsies was shown in Fig. 1. The PD-L1 CPS of the GPS-high group was higher than the GPS-low group (P < 0.001). Pathological complete response (pCR) rate was observed in 14 patients (13.6%) after neoadjuvant chemoradiotherapy. The pCR rates of the GPS-low and GPS-high groups were 14.1% and 11.1%, respectively (P > 0.999). The pCR rates of patients with PD-L1 CPS of 0 and >0 were 17.5% (10 of 57) and 12.5% (4 of 32), respectively (P = 0.766).
Prognostic significance of Glasgow prognostic score and combined positive score
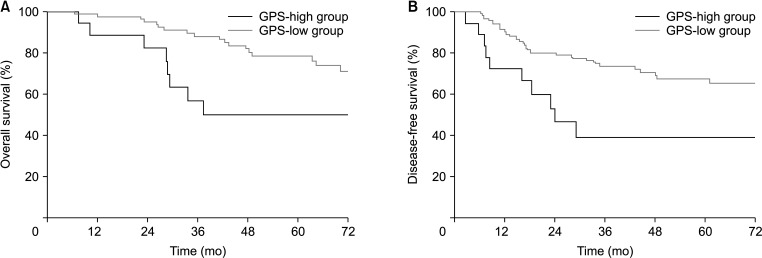
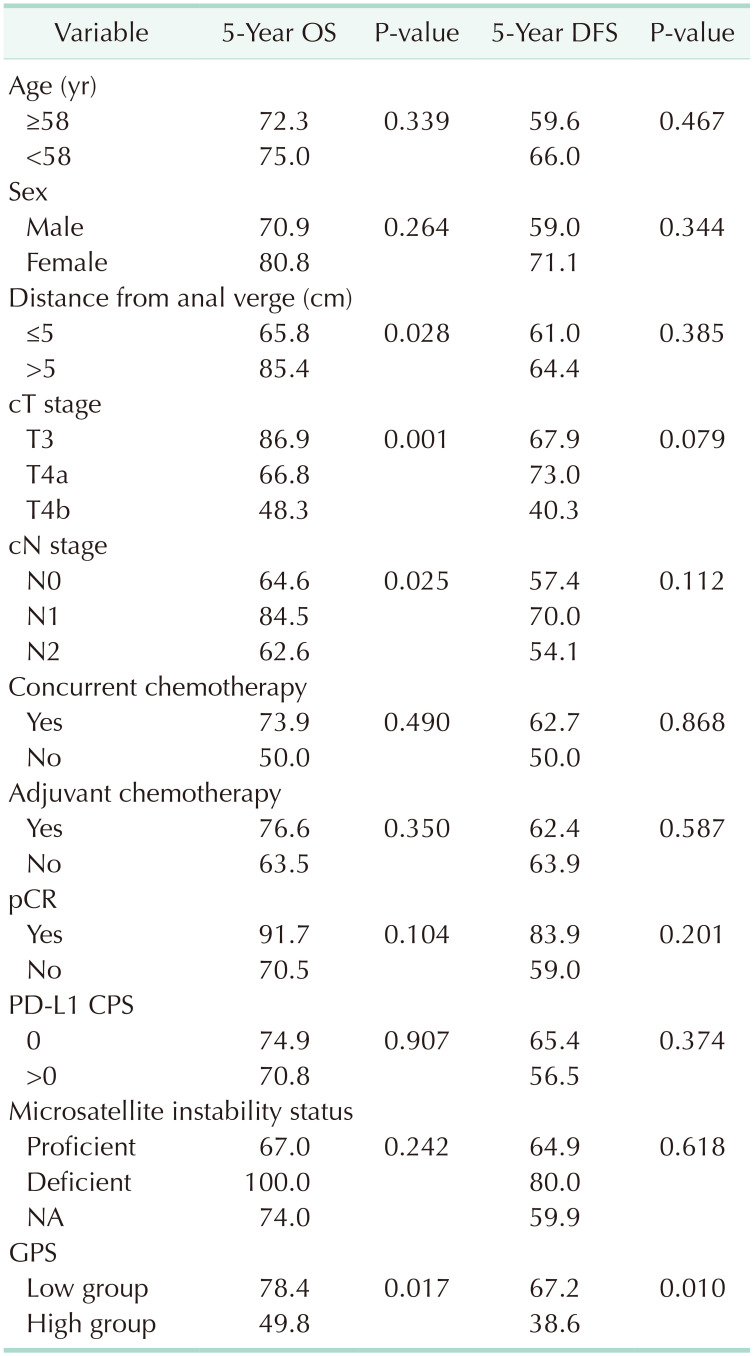
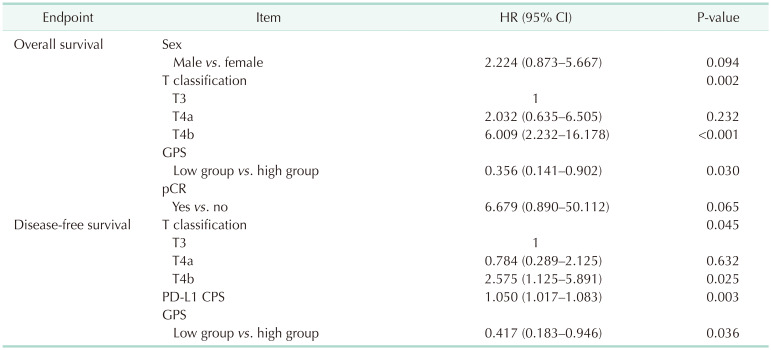
The median follow-up time was 64.5 months (range, 3.5–109.8 months). The value of various potential prognostic factors including age, sex, distance from anal verge, clinical (c) T stage, cN stage, concurrent chemotherapy, adjuvant chemotherapy, pCR, PD-L1 CPS, microsatellite instability status, and GPS (low group vs. high group) on predicting DFS and OS were evaluated. The 5-year OS rate in the GPS-low group was higher than the patients in the GPS-high group (78.4% vs. 49.8%, P = 0.017). The 5-year DFS rate in the GPS-low group was higher than the patients in the GPS-high group (67.2% vs. 38.6%, P = 0.010) (Fig. 1). In this study, the CPS of 0, 1–10, and ≥10 were observed in 56 (54.4%), 53 (51.5%), and 4 patients (3.9%), respectively (Fig. 2). No statistically significant difference was observed in terms of DFS or OS between the patients with PD-L1 CPS of 0 and >0 (P > 0.050). Multivariate analysis by Cox proportional hazards model indicated that T classification and GPS were associated with OS and DFS. Furthermore, PD-L1 CPS was associated with DFS (hazard ratio [HR], 1.050; 95% confidence interval [CI], 1.017–1.083; P = 0.003). The outcomes of univariate analysis and multivariate analysis are reported in Tables 2 and 3.
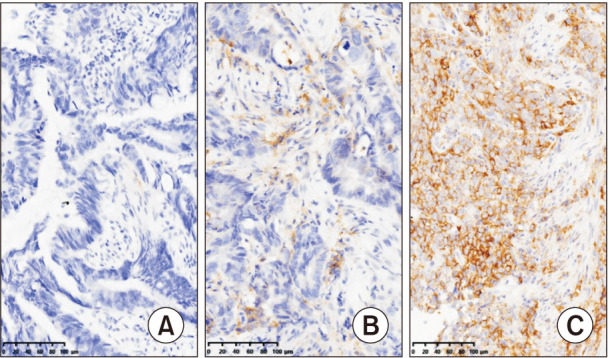 | Fig. 2Representative immunohistochemistry staining of programmed death-ligand 1 combined positive score with 0 (A), 1–10 (B), and ≥10 (C) in locally advanced rectal cancer biopsies (original magnification, ×200).
|
Go to :
DISCUSSION
In the present study, the relationship between GPS and PD-L1 CPS and survival of locally advanced rectal cancer patients treated by neoadjuvant chemoradiotherapy and TME was evaluated. We found that the PD-L1 CPS of the GPS-high group was higher than the GPS-low group and GPS and PD-L1 CPS were associated with the prognosis of locally advanced rectal cancer.
GPS determined by serum CRP and albumin is considered a hallmark of inflammatory response in the tumor environment. In 2007, McMillan et al. [10] firstly reported that the baseline GPS could predict overall and cancer-specific survival of patients with colon and rectal cancer receiving surgery. In their study, 123 patients (38.9%) with rectal cancer were included, and the elevated GPS was related to older age but not tumor stage. In another prospectively collected data set of 1,590 patients with colorectal cancer (510 patients with rectal cancer) receiving curative surgery, GPS was a prognostic factor for OS (HR, 2.344; 95% CI, 1.621–3.390; P = 0.001) and DFS (HR, 1.532; 95% CI, 1.030–2.278; P = 0.035) [11]. In the present study, GPS was associated with DFS and OS of locally advanced rectal cancer; the elevated GPS was related to T classification but not age (Table 1).
Based on KEYNOTE-059, KEYNOTE-012, and KEYNOTE-028 studies, a CPS of >1 has been standardized for predicting response to pembrolizumab in gastric and gastroesophageal junction cancer [12]. However, CPS of ≥10 was considered as a biomarker for predicting response to pembrolizumab in the KEYNOTE-059, KEYNOTE-061, and KEYNOTE-062 studies [13]. In the present study, the median PD-L1 CPS of the whole group was 0 (range, 0–70), and no statistically significant difference was observed in terms of DFS or OS between the patients with PD-L1 CPS of 0 and >0 (P > 0.050) by univariate analysis. In multivariate analysis, PD-L1 CPS was adopted as a continuous variable and PD-L1 CPS was observed as a biomarker for DFS. One study of colorectal cancer comparing the PD-L1 expression patterns using 3 primary PD-L1 antibodies (assay 1, MIH1; assay 2, E1L3; and assay 3, 22C3) by IHC indicated that the percentage scorings and positivity rates of the 3 assays differed [14]. In Huemer et al.’s study [9], 72 patients with rectal cancer treated by neoadjuvant chemoradiotherapy were included and the anti-PD-L1 antibody (22C3, SK006; Agilent, Santa Clara, CA, USA) was adopted for PD-L1 staining. PD-L1 CPS prior to neoadjuvant chemoradiotherapy was not associated with pCR or survival, likely due to the limited number of patients included and the different PD-L1 antibodies used [9].
In the study of investigating the relationships between the serum levels of 13 cytokines (interleukin [IL]-1ra, IL-4, IL-6, IL-7, IL-8, IL-9, IL-12, interferon-γ, CXL10, CCL2, CCL4, CCL11, and PDGF-BB) and the densities of 8 types of tumor-infiltrating inflammatory cells (CD1a, CD3, CD8, CD68, CD83, FoxP3, mast cell tryptase and neutrophil elastase) in 147 colorectal cancer patients, elevated serum IL-12 levels were related to the densities of intratumoral neutrophils, peritumoral CD8+ T cells, and intraepithelial CD3+ T cells [15]. However, in another study including 396 stage II colon cancer patients, local (intratumoral chronic inflammatory cell density) and systemic (neutrophil-to-lymphocyte ratio) inflammation was assessed and no significant inverse relationship between local and systemic inflammation was observed [16]. The PD-L1 CPS of the GPS-high group was higher than the GPS-low group in this study. The relationship between immunity and inflammation would deserve further investigation in the era of cancer immunotherapy [17].
There were several limitations in this study including the retrospective nature of the study design; 66 patients (64.1%) with unavailable microsatellite instability status and all the included patients treated at a single center. In addition, no locally advanced rectal cancer patients treated by PD-1/PD-L1 antibodies were included, leaving the prediction value of GPS and PD-L1 CPS uncertain at this moment.
In conclusion, elevated GPS was related to the PD-L1 CPS. GPS and PD-L1 CPS were associated with prognosis of locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy followed by TME.
Go to :
 XML Download
XML Download