

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. COVID-19 has dramatically spread globally, and as of August 18, 2021, over 200 million cases and over 4 million COVID-19-related deaths were confirmed.1 The most common symptoms are fever, cough, fatigue, shortness of breath, and severe acute respiratory distress syndrome (ARDS).2 Until now, the clinical reports of pediatric COVID-19 suggest that the manifestations of pediatric COVID-19 appear to be milder than those of adult cases.3 However, COVID-19 can still become severe in children and adolescents.4
In Korea, there has been only one case report of severe COVID-19 in pediatric patients.5 To the best of our knowledge, severe ARDS in children has not been reported in Korea, especially for the delta variant. Here, we report a severe case of ARDS in which the patient required ventilation.
Go to : 
CASE DESCRIPTION
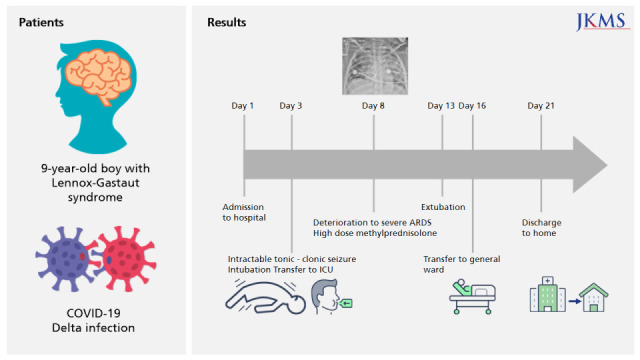
A 9-year-old boy was admitted to our hospital on July 26, 2021, and diagnosed with asymptomatic COVID-19. He was under self-quarantine for 6 days due to close contact with a confirmed case. A reverse-transcriptase quantitative real-time polymerase chain reaction (PCR) assay using a PowerChek™ SARS-CoV-2 S-gene mutation detection kit (version 1, P681; Kogene Biotech, Seoul, Republic of Korea) was used to diagnose the SARS-CoV-2 delta variant. Relevant medication history included anti-epileptic medication for Lennox-Gastaut syndrome, including levetiracetam, lamotrigine, zonisamide, sodium valproate, clobazam, and cannabidiol, beginning at 8 months of age. Even though the patient had partial seizure events about twice a month and a developmental delay, he was able to move on his own and take food orally. No respiratory support was needed before having COVID-19. On admission, there were no COVID-19-associated symptoms, such as fever, cough, sputum, or dyspnea. His body temperature was 36.7°C, the heart rate was 109 bpm, the respiratory rate was 21 breaths per minute, and the saturation of percutaneous oxygen (SpO2) was sustained at ≥ 95% with room air. His height was 130 cm (5th percentile), weight was 35 kg (50th percentile), and the body mass index was 20.7 kg/m2 (75th percentile). The initial laboratory findings were as follows: white blood cell count 12,590/μL, hemoglobin 11.5 g/dL, platelet count 473,000/μL, C-reactive protein (CRP) 2.74 mg/L (range, 0–5), and D-dimer 0.48 mg/L (range, 0–0.5). The results of initial venous blood gas analysis were within the normal ranges (pH 7.40, pCO2 = 40 mmHg, pO2 = 44 mmHg, and HCO3 = 24.8 mmHg). The initial chest X-ray was clear, without any COVID-19 lesions in either lung (Fig. 1A). A rhinovirus was detected on the PCR performed to determine co-infection. Since there was no negative pressure room in our hospital, the sputum culture test could not be performed. No bacteria were detected on the blood culture.
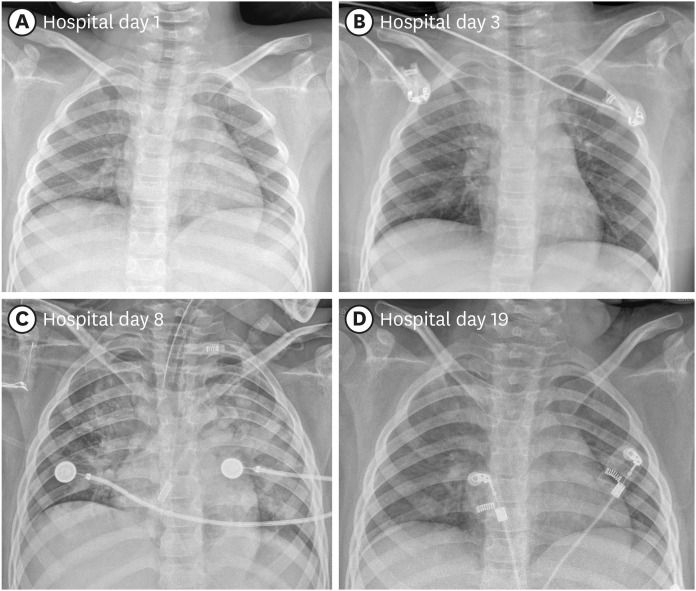 | Fig. 1Chest X-ray images of the patient. (A) Upon admission. (B) Right upper lobe haziness following intractable seizures on post-admission day 3. (C) Increased opacity in both lungs on post-admission day 8 when PaO2/FiO2 decreased to 84.3. (D) Chest X-ray at the time of discharge on post-admission day 19.
|
On post-admission day 3, a high fever of 39.8°C developed with intractable tonic-clonic seizures that lasted for about two hours and persisted despite repeated administration of lorazepam. The SpO2 decreased to 76% despite O2 supplementation of 10 L/min through an O2 reserve mask. The patient was transferred to the COVID intensive care unit following administration of a loading dose of phenytoin and midazolam, along with intubation. Upon intubation, saturation was maintained at ≥ 95% with ventilator care at an FiO2 of 21%; at this time, a newly developed area of increased density was observed on the right upper lobe (Fig. 1B). The ventilator settings on the day of intubation and on the next day, as well as the results of atrial blood gas analysis, are displayed on Table 1. Empirical antibiotics were initiated using piperacillin-tazobactam due to the potential for aspiration pneumonia. The following day, the oxygen requirement increased, and increased haziness was observed on both lung fields, particularly on the right upper lobe. Laboratory findings indicated elevated CRP (120.4 mg/L), and corticosteroids were administered twice (methylprednisolone, 1 mg/kg/dose). Empirical antibiotics were changed to vancomycin and meropenem. Despite the conservative management of COVID-19, oxygenation continued to deteriorate. On the eighth day of admission, PaO2/FiO2 decreased to 84.3 (Table 1), and both lungs exhibited increased consolidation on chest X-ray (Fig. 1C). The laboratory findings at that time were as follows: white blood cell count 7,710/μL, lymphocytes 1,150/μL, hemoglobin 9.1 g/dL, platelet count 209,000/μL, CRP 63.98 mg/L, aspartate aminotransferase 59 IU/L, and alanine aminotransferase 48 IU/L. The patient had persistent, recurrent fever. To improve oxygenation, a high positive end-expiratory pressure (11 mmHg) and low tidal volume (4–6 mL/kg) were set. A short course of methylprednisolone pulse therapy (10 mg/kg/day divided into two doses) was administered for two days and tapered over 11 days, which improved oxygenation with a PaO2/FiO2 of 245 (Table 1). Furthermore, the pneumonic consolidation improved slightly in both lungs. Corticosteroids were tapered, and extubation was successful after 10 days of tracheal intubation. No side effects were reported, including hyperglycemia and hypertension. There was also no other major organ dysfunction. On post-admission day 27, the patient was discharged without O2 requirement, and no remnant lesions were observed in either lung (Fig. 1D).
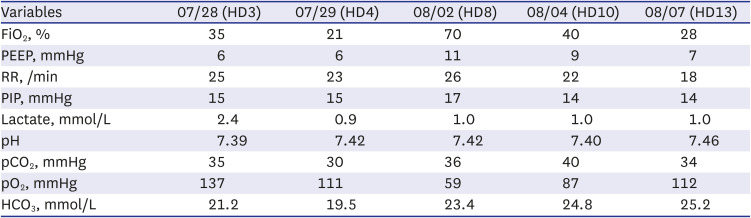
Table 1
The ventilator setting and results of arterial blood gas analysis of the patient throughout the treatment by date
HD = hospital day, PEEP = positive end-expiratory pressure, RR = respiratory rate, PIP = peak inspiratory pressure.
![]()
Ethics statement
The Institutional Review Board (IRB) of Jeonbuk National University Hospital approved this study (IRB No. 2021-09-086). The requirement of informed consent for publishing was renounced.
Go to :
DISCUSSION
Here, we report a case of severe ARDS caused by the SARS-CoV-2 delta variant. Several COVID-19 reports suggest that pediatric patients are less likely to progress to severe or critical disease than adults.67 However, this has changed with the delta variant. In Korea, and as of August 21, 2021, the delta variant was detected in 90.0% of patients with confirmed COVID-19.8 However, since the delta variant developed recently, the clinical features of pediatric patients remain less clear. In that sense, this report serves as a basis for future research on the clinical features of the delta variant in children.
In our patient, high-dose methylprednisolone was effective as hypoxia therapy. This was consistent with reports that methylprednisolone therapy demonstrated superior outcomes than dexamethasone in adults with COVID-19-induced hypoxia.91011 In particular, high-dose methylprednisolone pulse therapy (250–500 mg·day−1) could be effective in patients hospitalized for severe COVID-19.1011 There are little data on glucocorticoid use in children for COVID-19. In the pre-COVID era, it was reported that the use of prolonged low-dose methylprednisolone (at a dose of 1–2 mg/kg/day followed by tapering over 7 days or more) can be effective in reducing the duration of mechanical ventilation and mortality in patients with ARDS.12 Methylprednisolone may be superior to hydrocortisone for the treatment of ARDS in several ways. Methylprednisolone has greater affinity to the glucocorticoid receptor and can penetrate further and for a longer period in the lung tissue. The effectiveness of methylprednisolone treatment in increasing the number of glucocorticoid receptors and improving function in patients with ARDS; the corresponding resolution of pulmonary and system inflammation was also previously reported.13 Our case suggests that low- to medium-dose methylprednisolone therapy (2–5 mg/kg/day) can be effective in pediatric patients with ARDS caused by severe COVID-19. The patient was discharged without oxygen requirements, and we predict that the long-term prognosis of COVID-19 for this patient will be favorable.
How COVID-19 manifests in patients with Lennox-Gastaut syndrome is relatively unknown. Cabezudo-García et al.14 published a cross-sectional observational study demonstrating that patients with active epilepsy may have a higher mortality risk. In a systematic review, exacerbation of underlying neurological symptoms occurred with severe COVID-19,15 while another descriptive analysis of severe COVID-19 in children treated with remdesivir showed that 9% of patients had seizures.16 In our case, the exacerbation of preexisting neurologic symptoms was observed before aggravation of pulmonary symptoms. Mechanical ventilation due to intractable seizures can aggravate the respiratory condition. The effect of SARS-CoV-2 on preexisting neurologic conditions such as intractable epilepsy requires further research.
Go to :
 XML Download
XML Download