

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
When properly diagnosed and treated, clinically apparent pulmonary embolism (PE) is an uncommon cause of death, and the PE recurs in only a small minority of patients. Most deaths are related to underlying diseases such as cancer, congestive heart failure, or chronic lung disease. In PE patients with such underlying disease(s), they show higher risk of death than did other patients with PE. And in such patients the deaths occur within one year after the attack of PE.1
It has been known that residual thrombi and microscopic vasculopathy after the attack(s) of acute PE lead to chronic thromboembolic pulmonary hypertension (CTEPH). However, the incidence of CTEPH after acute PE and associated risk factors for CTEPH developments are not well documented. The purpose of this pictorial essay was to demonstrate serial computed tomography pulmonary angiography (CTPA) features in patients with acute massive and submassive PE and to disclose acute CTPA and clinical features that are related to the prediction of oncoming CTEPH.
Go to : 
IMAGING OF ACUTE AND CHRONIC PE AND DEEP VEIN THROMBOSIS (DVT)
Currently, the most commonly used first-choice imaging examination in patients with suspected PE is CTPA as thrombi in the vessels can be visualized directly on CTPA (Fig. 1).234 However, clots in the small vessels (e.g., subsegmental branch) are sometimes difficult to visualize on CTPA. The CTPA can be a part of triple-rule-out (TRO) imaging technique where a cost-effective evaluation of the coronary arteries, aorta, pulmonary arteries and adjacent intrathoracic structures for the patient with acute chest pain can be accomplished (Fig. 2). TRO CT is most appropriate for the patient who is presumed to be at low-to-intermediate risk for acute coronary syndrome and whose symptoms may also be caused by acute abnormal conditions of the aorta or pulmonary artery.5 Technically, the heart is positioned at the center of the gantry to maximize resolution. Z-axis coverage starts 1–2 cm above the aortic arch and extends through heart base. Cranio-caudal direction acquisition is preferred. Standard scan parameters include mean effective mAs of 200 and 120 kVp.5 Artificial intelligence (AI) for the detection of PE endorses high degree of diagnostic accuracy for the detection of PE on CTPA.67 According to a study, the AI algorithm allows 93% sensitivity and 96% specificity on a per-exam basis for the identification of PE. On a per-lesion basis, 1,174 of 1,352 (89%) findings marked as embolus were true emboli.6 Thus, sensitivity and specificity are balanced and therefore the AI for automated PE detection could become a clinically useful diagnostic adjunct.
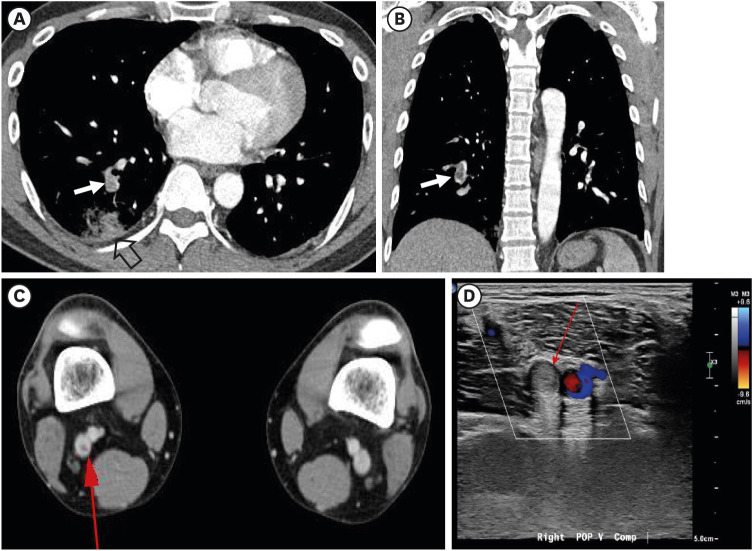
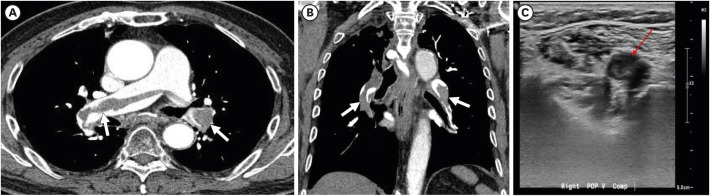 | Fig. 1Acute pulmonary embolism in a 79-year-old man who has deep vein thrombosis. (A) Transverse image of enhanced CT scan obtained at level of bronchus intermedius demonstrates filling defects in a linear manner in proximal right pulmonary and interlobar artery and also in proximal left lower lobar arteries (arrows). (B) Coronal reformatted image depicts filling defects (arrows) in right interlobar and lower lobar and left lower lobar arteries with so-called railway-track sign. (C) Ultrasonography obtained at right popliteal vein discloses isoechoic recently-developed deep vein thrombosis (thin red arrow).
|
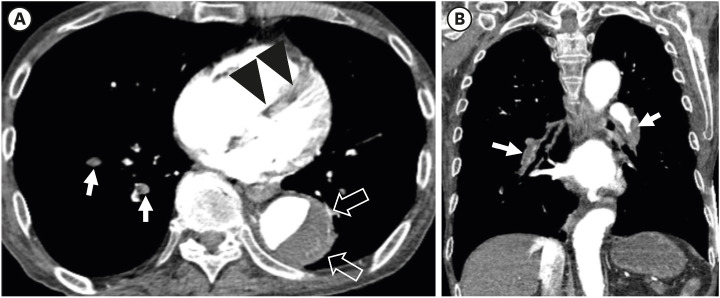 | Fig. 2Triple-rule-out technique showing acute massive pulmonary embolism and aortic dissection simultaneously in a 73-year-old man. (A) Transverse image of enhanced CT scan obtained at level segmental bronchi of lower lobes demonstrates filling defects in a linear manner in segmental right lower lobar arteries (arrows). Also note flattening of interventricular septum (arrowheads) reflecting the presence of right ventricular strain, and aortic dissection (open arrows) in descending thoracic aorta. (B) Coronal reformatted image depicts filling defects (arrows) in right lower lobar and proximal left lower lobar arteries. Note both lower lobar arteries are completely occluded with emboli. Patient showed hypotension and died of the disease. Laboratory test results were as follows: ProBNP, 2,261 pg/mL (normal, 125–450 pg/mL) and Troponin-I, 0.0839 ng/mL (normal, below 0.04 ng/mL). Initially, the mortality risk was classified into high group in this patient.
|
For the screening of CTEPH among patients with acute PE, radionuclide ventilation/perfusion scintigraphy (V/Q scintigraphy) is currently considered the technique of choice (Figs. 3 and 4).8910 Tunariu et al.9 reported that the sensitivity of V/Q scintigraphy, as well as the diagnostic specificity for CTEPH, is higher than that of CTPA.
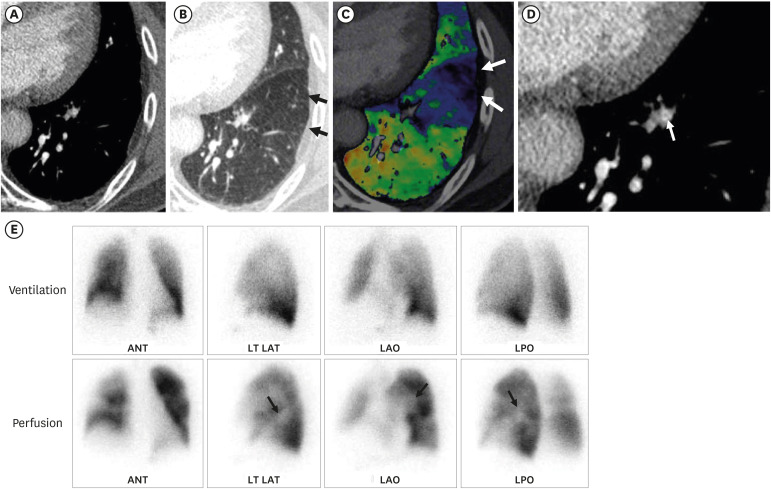 | Fig. 3Segmental pulmonary embolism detected with dual-energy CT in a 67-year-old man with chronic thromboembolic pulmonary hypertension. (A) Transverse image of CT scan obtained at level of left ventricle shows no identifiable filling defect in left lower lobe. (B, C) Lung window (B) and color-coded (C) images of CT scan obtained at same level to (A) demonstrate mosaic attenuation of triangular shape (arrows in B) and perfusion defect on color-coded image (arrows in C) within same pulmonary segment to (A), suggesting possible presence of segmental embolism. (D) After reviewing CT pulmonary angiography and color-coded iodine map images, presence of segmental pulmonary embolism was considered in retrospect especially on magnified view of transverse image showing partially occlusive thrombi as intraluminal “bands” within anterior basal segmental artery of the left lower pulmonary artery (arrow). (E) Corresponding ventilation (upper row) and perfusion (lower row) scintigraphy with multiplanar imaging (from left to right: anterior, left lateral, left anterior oblique and left posterior oblique views) showing V/Q mismatch (perfusion defects) within left lower lobe (arrows).CT = computed tomography, ANT = anterior, LT LAT = left lateral, LAO = left anterior oblique, LPO = left posterior oblique.
|
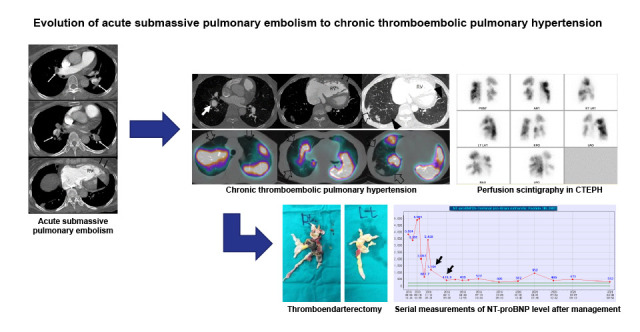
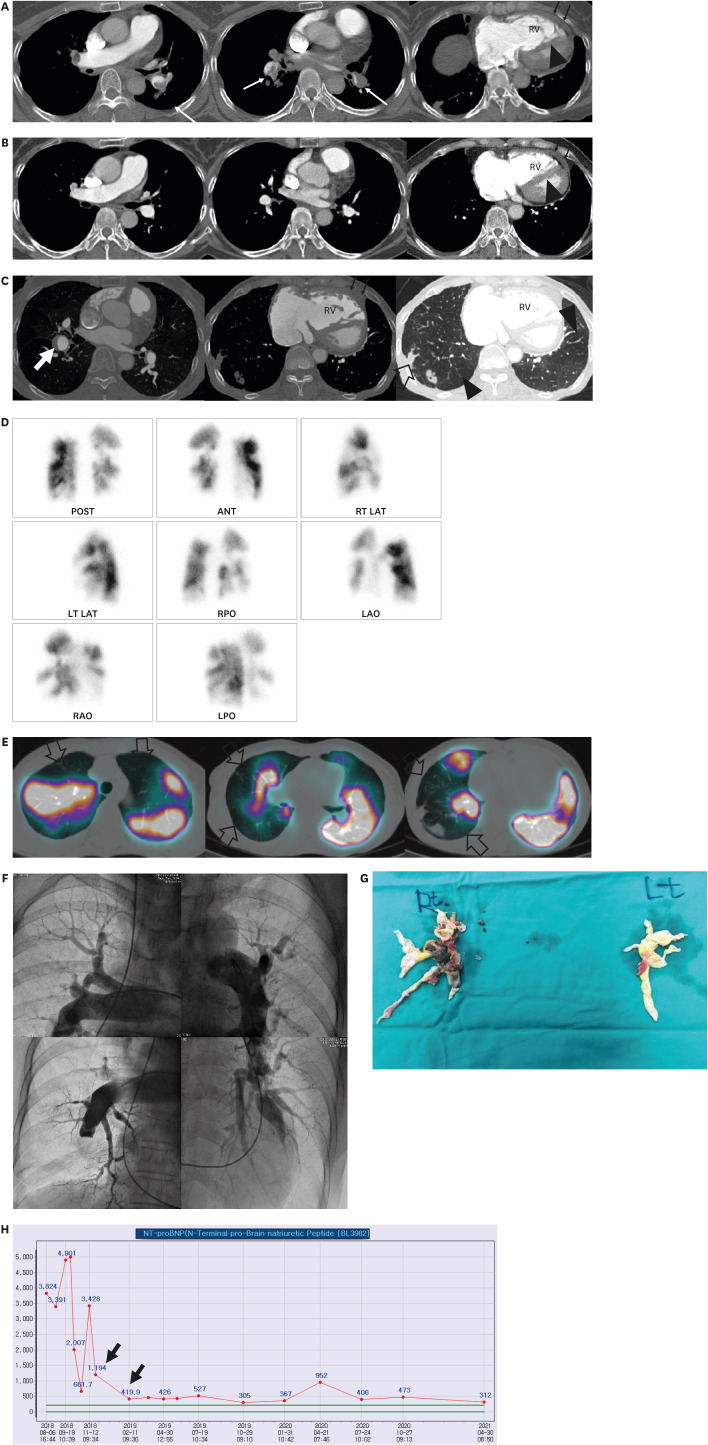 | Fig. 4Evolution of acute submassive pulmonary embolism to chronic thromboembolic pulmonary hypertension in a 70-year-old woman. (A) Consecutive transverse enhanced CT scans obtained in January 2012 show filling defects (arrows) in bilateral pulmonary arteries and their branches. Please note occlusive defect in left lower lobar artery (arrow in second Fig.). Also note larger RV than LV (RV/LV ratio, 1.20), flattening of interventricular septum (arrowhead) and thickened RV free wall (thin arrows, measuring up to 7 mm). Short axis of RV is measured from inner wall to inner wall where tricuspid valve is scanned, whereas short axis of left ventricle is measured from inner wall to inner wall where mitral valve is scanned. Among related factors of oncoming CTEPH, the patient showed RV dysfunction with RV/LV ratio greater than 1.0 when diagnosed with acute PE. (B) CT scans obtained in March 2012 demonstrate that all emboli have resolved completely. But please note again enlarged RV, thickened RV free wall (thin arrows), and flattened interventricular septum (arrowhead). (C) Mixed lung and mediastinal window images obtained in August 2018 depict evolution into chronic thromboembolic pulmonary hypertension. Please note enlarged lobar and segmental pulmonary arteries, unusually tortuous branch arteries, eccentric embolus in right lower lobar artery (arrow), large areas (arrowheads) of mosaic perfusion, and pulmonary infarction areas (open arrow). Also note enlarged RV and its thickened anterior free wall (thin arrows), and flattened interventricular septum. (D) Perfusion scintigraphy with multiplanar imaging obtained at similar time to (C) displays multifocal areas of perfusion defects in both lungs, typical features that can be seen in chronic thromboembolic pulmonary hypertension. (E) Dual-energy CT and its color-coded perfusion map images obtained in August 2018 before thromboendarterectomy clearly show multifocal areas of perfusion defects (open arrows) in both lungs, features well matched with prior perfusion scintigraphy (D). (F) Digital subtraction angiography obtained in August 2018 before thromboendarterectomy demonstrates pruned-tree appearance of pulmonary vasculature and multifocal areas of non-perfused lung areas. (G) Gross pathologic specimens depict pulmonary thromboendarterectomy byproducts which had filled pulmonary vessels heading toward non-perfused lung areas. (H) Serial measurements of NT-proBNP level before and after thromboendarterectomy display sharp decline (arrows) of its level after surgical procedures.RV = right ventricle, POST = posterior, ANT = anterior, RT LAT right lateral, LT LAT = left lateral, RPO = right posterior oblique, LAO = left anterior oblique, RAO = right anterior oblique, LPO = left posterior oblique, NT-proBNP = N-terminal pro-brain natriuretic peptide, CT = computed tomography.
|
The introduction of dual-energy CT (DECT) has allowed radiologists to generate functional images as well as traditional anatomic images.1112 With the recent advent of the DECT technique, the ability to obtain color-coded iodine perfusion map of the lung may allow us to evaluate perfusion changes in the lungs and further supports the role of pulmonary CTPA (Figs. 3 and 4).13141516 Hong et al.11 pieced together the diagnostic values of DECT for the detection of acute and chronic PE and the results are as follows: sensitivity and specificity for acute PE range from 60% to 90% and 88% to 99%, respectively, for acute PE; and those for chronic PE range from 96% to 100% and 76% to 96%, respectively, for chronic PE, when using SPECT or scintigraphy as a reference standard. It is also interesting that in terms of radiation dose, according to the same summary from Hong et al.,11 DECT does not add radiation dose, when compared with conventional CT. It has been reported in prior study that DECT is associated with higher radiation exposure than single-energy CT.17
Doppler and color Doppler ultrasonography has been regarded as a gold standard for the diagnosis of DVT (Figs. 1 and 5). Following the pulmonary examination, the inferior vena cava and the iliac, femoral, and popliteal veins can be studied with CT without additional intravenous contrast administration. Indirect CT venography (CTV) after CTPA simplifies and shortens venous thromboembolism work-up (Fig. 5). Initial studies indicate that CTV is comparable to ultrasound in the evaluation of femoral and/or popliteal DVT. CTV has the advantage of evaluating the iliac veins and inferior vena cava, namely vessels poorly seen on sonography and venography. Combining CTV with CTPA increases confidence in deferring treatment when results for both the pulmonary arteries and leg veins are negative, and increases the diagnosis of venous thromboembolism by 25% over CTPA alone.1819 It should be considered, however, that CT technique such as dual-energy spectral imaging and/or adaptive statistical iterative reconstruction could be adopted to mitigate patient radiation dose for combined CTV and CTPA.2021
 | Fig. 5Acute pulmonary embolism and deep vein thrombosis detected with CT pulmonary angiography and indirect CT venography, respectively, in a 38-year-old man complaining of right flank pain. (A) Enhanced transverse CT scan obtained at level of segmental arteries shows a filling defect (arrow) in right posterior basal segmental artery. Also note segmental consolidation (open arrow) representing bland infarction in posterior basal segment of right lower lobe, related to embolism. (B) Coronal reformatted image also demonstrates filling defect (arrow) in posterior basal segmental artery. (C) Indirect CT venography obtained two minutes after contrast medium injection demonstrate filling defect (thin arrow) in right popliteal vein. (D) Color-Doppler ultrasonography depicts deep vein thrombosis (thin arrow) in right popliteal vein.CT = computed tomography.
|
Go to :
MASSIVE AND SUBMASSIVE PE AND RELATIONSHIP WITH CLINICAL OUTCOME
According to a guidance document issued by the American Heart Association in 2011, the terms of massive (mortality of 25–65%), submassive (mortality of 3%), and low-risk (mortality of < 1%) PE were defined on patient mortality likelihood.22
Massive PE refers to the event in which the patient has sustained systemic hypotension (< 90 mmHg systolic, for > 15 minutes) and bradycardia with signs of shock or being pulseless (Fig. 2), whereas submassive PE refers to the condition where despite of the absence of systemic hypotension the patient has the evidence of myocardial necrosis or right ventricular (RV) dysfunction with the PE (Fig. 6).23 It should be noted that in patient prognosis (mortality) stratification, no mention has been present on clot burden or location (which can be determined on CTPA).23
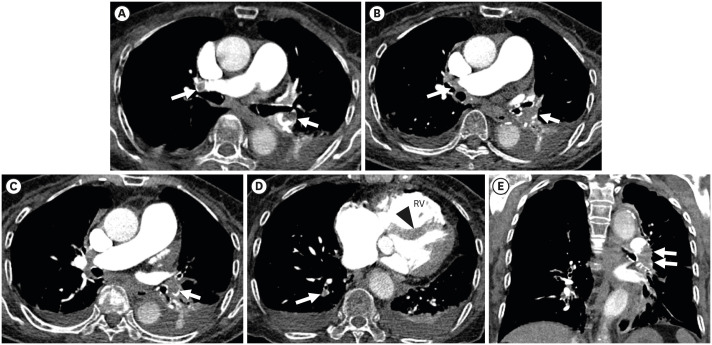 | Fig. 6Submassive and acute pulmonary embolism in an 87-year-old woman complaining of dyspnea. (A) Transverse image of enhanced CT scans obtained at level of upper lobar bronchus demonstrates filling defects in a linear manner in right proximal interlobar artery and left lower lobar artery (arrow). (B) CT scan obtained at cardiac ventricular level depicts leftward bowing (arrowhead) of interventricular septum suggesting presence of right ventricular strain. Also note enlarged RV. Pulmonary embolism is also present in posterior basal segmental artery (arrow). Pleural effusions are associated bilaterally (C, D). (E) Coronal reformatted image discloses filling defect (arrows) occluding left lower lobar artery. Laboratory test results were as follows: ProBNP, 6,758 pg/mL (normal, 125–450 pg/mL) and Troponin-I, 0.2495 ng/mL (normal, below 0.04 ng/mL). Initial vital signs were stable except peripheral and arterial oxygen saturation were slightly lower. The patient underwent echocardiography and it showed moderate to severe RV dysfunction. The mortality risk was classified into intermediate group.RV = right ventricle, CT = computed tomography.
|
Acute PE attack and embolic vascular obstruction of a significant extent of pulmonary circulation (usually more than 30%) leads to pulmonary vascular resistance and consequent acute pulmonary artery hypertension. This pulmonary vascular obstruction is further worsened by the release of vasoactive agents from plasma, platelets, or tissue and reflex pulmonary artery vasoconstriction, and thus resulting in systemic arterial hypotension.24
RV compensation and increased contractile performance are needed for RV outflow obstruction. The compensation requires further an increase in work transmission from the RV to its vascular bed; that transmission necessitates a greater myocardial oxygen requirement and a reduction of RV mechanical efficiency. RV dilatation and resultant pericardial constraint elicit bowing of the interventricular septum (IVS) toward the left ventricle (LV),25 resulting in a decreased LV preload; subsequently decreased LV output and decreased systemic arterial pressure may result in a downward vicious cycle of compromised coronary perfusion, increasing ventricular hypoxemia and RV dysfunction, and eventually cardiogenic shock and RV infarction and finally circulatory collapse (Fig. 7).26
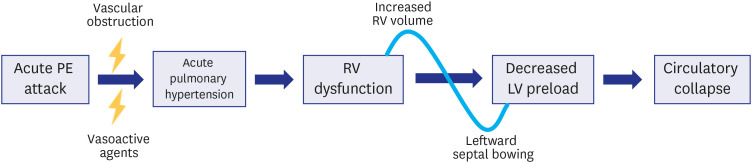 | Fig. 7Diagram explaining cascade events from acute massive pulmonary embolism to systemic hypotension and circulatory collapse. With massive emboli, vascular obstruction and related vasoactive agents cause acute pulmonary hypertension which leads to morphologic changes of right ventricular volume and leftward interventricular septal bowing and right ventricular dysfunction. Decreased venous return due to right ventricular dysfunction and decreased left ventricular volume related to interventricular septal bowing elicit decreased left ventricular preload and resultant circulatory collapse (Modified from reference 26: Ghaye et al. Radiographics 2006; 26: 23-39).PE = pulmonary embolism, RV = right ventricle, LV = left ventricle.
|
In acute PE, circulatory failure and systemic hypotension are important for predicting poor prognosis. However, hemodynamically unstable PE accounts for only a minority of all PE presentations. Other clinical predictors such as age > 70 years, coexisting congestive heart failure, or chronic obstructive pulmonary disease are also regarded as bad prognosis factors. This is because such pre-existing cardiopulmonary dysfunctions impairs RV adaptability to abrupt afterload increase.2426
Go to :
PROGNOSTIC FACTOR EVALUATION IN ACUTE PE
Echocardiography, CTPA, brain natriuretic peptide (BNP), N-terminal pro-brain natriuretic peptide (NT-proBNP), Troponin I, Troponin T, and heart-type fatty acid protein (H-FABP) are evaluated for predicting early mortality. By the use of test results, mortality risk can be classified into high-, intermediate- and low-risk groups. The main parameters and scores were determined by 1) the presence of shock or hypotension, 2) PE severity index,27 3) signs of RV dysfunction on an imaging test, and 4) cardiac laboratory biomarkers (Figs. 2, 4, and 6).28
Go to :
IDENTIFICATION AND CLINICAL SIGNIFICANCE OF ISOLATED SUBSEGMENTAL PE
Helical CT and DECT are more efficient in the detection of subsegmental PE.29 Patients with isolated subsegmental PE appear to have a more benign clinical course than those with segmental or more proximal PE; the patients with subsegmental PE have lesser associated DVT, less frequent dyspnea, and low clinical probability of PE. Therefore, the necessity to treat patients with isolated subsegmental PE is uncertain. However, small peripheral PE may prove clinically relevant in cases of diminished cardiorespiratory reserve. Currently no data are available on the long-term consequences of such events, especially on the occurrence of chronic pulmonary hypertension. As mentioned above, patients with isolated subsegmental PE are unlikely to have an associated DVT. Therefore, in patients with subsegmental PE, rather than directly commencing anticoagulation therapy, clinical surveillance might be a way of benefit in management. This approach is currently assessed in an ongoing prospective cohort study.3031
Go to :
DVT AND PE
Acute PE patients with co-existing DVT are more serious clinically than those without a DVT. An acute picture may be present in the chronic background in a significant proportion of patients with PE with co-existing DVT. Moreover, in the presence of DVT, PE appears to be more central (Fig. 1).32
Go to :
PATHOGENIC MECHANISM OF CTEPH AND ITS CT DIAGNOSTIC CRITERIA
Acute PE usually resolve within months. Occasionally, the thrombi change into fibrous vascular obstruction and results in occlusion of the thrombosed veins. Alias et al.,33 in a mouse model, suggested that endothelial cell-specific deletion of vascular endothelial growth factor 2/kinase insert domain protein receptor (VEGF-R2/kdr) causes the mitigation of thrombus vessel formation and misguides thrombus resolution. Medical conditions compromising early thrombus angiogenesis may facilitate the development of CTEPH.
On imaging studies, parenchymal features such as mosaic attenuation, asymmetric pulmonary arterial size (Figs. 4 and 8), and pulmonary infarcts are commonly observed. Combined with right-sided heart chamber enlargement and particularly with evidence of PE on pulmonary arterial branches on enhanced scans, the CTPA features can be specific in the diagnosis of the CTEPH, In addition, bronchial artery hypertrophy and collateral vessel development can be seen.34 Unusual enlargement of bilateral pulmonary arteries can also be seen on chest radiograph and digital subtraction angiography (Fig. 8).
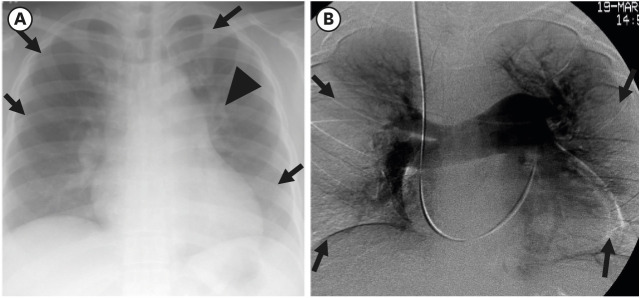 | Fig. 8Chest radiographic and DSA pulmonary angiography explaining unusual pulmonary vascularity and asymmetric pulmonary hypoperfusion in a 58-year-old woman having chronic thromboembolic pulmonary hypertension. (A) Chest radiograph shows enlarged bilateral hila and unusually tortuous and prominent left upper lobar arteries (arrowheads). Also note pulmonary oligemia in right upper and middle lung zone and left upper and lower lung zones (arrows). Cardiomegaly is also seen with right ventricular enlargement (elevated left lower cardiac border). (B) DSA pulmonary angiography depicts absent pulmonary perfusion (arrows) in bilateral middle and lower lung zones owing to vascular occlusion with chronic emboli.DSA = digital subtraction angiographic.
|
Go to :
MEASUREMENTS OF CARDIAC CHAMBERS FOR PROGNOSIS OF ACUTE AND CHRONIC PE
The RV is a thin-walled chamber having a smaller diameter than the LV. With increasing pulmonary artery pressure, the RV begins to be hypertrophied in order to maintain stroke volume and cardiac output. It becomes eventually dilated and fails to function properly. The increased RV muscle mass can be measured on CT at middle ventricular level. The normal thickness of the RV free wall is 4 mm or less. When the thickness is 6 mm or more (Fig. 4A-C), the sensitivity and specificity for the presence of pulmonary hypertension is 81% and 92%, respectively.3536
With increasing RV chamber related to RV strain and pulmonary hypertension, the RV/LV luminal diameter starts to increase. RV dilatation is regarded to be present when the RV/LV ratio is greater than 1:1 with a sensitivity and a specificity of shared 86%.35 Short axis of the RV is measured from inner wall to inner wall where tricuspid valve is scanned (typically in the basal third of the RV), whereas short axis of the LV is measured from inner wall to inner wall where mitral valve is scanned (typically in the basal third of the LV).
In healthy subjects, the IVS has a right-sided convexity. With increase in RV strain, the right-sided convexity becomes to be flattened or finally to be reversed with left-sided convexity. Once the leftwardly bowed IVS impedes on LV, cardiac output becomes compromised. Patients with a main pulmonary arterial pressure of > 30 mmHg appear to have leftward bowing of the IVS (Fig. 7).37
Go to :
QUANTIFICATION OF PE EXTENT ON IMAGING STUDIES
Initially devised as angiographic severity indices (Miller and Walsch scoring) for comparison of the PE resolution speed on heparin or fibrinolytic therapy, the modified Miller and Walsh scoring systems have been adopted for CTPA. The modified scoring systems provide excellent correlation between the two scoring systems and a good interobserver agreement.2638 Unlikely from the modified Miller and Walsh scoring system, Qanadli et al.39 and Mastora et al.,40 respectively, designed PE scoring system where partial and complete obstructions of segmental arteries with PE were scored differently from each other (Fig. 9).
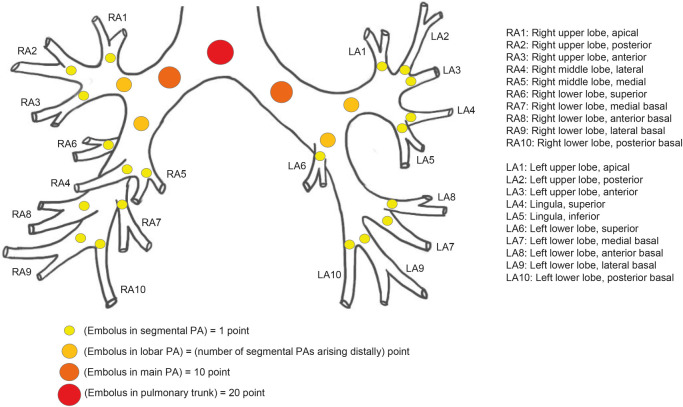 | Fig. 9Schematic diagram of Qanadli scoring system of acute pulmonary embolism. To quantify arterial obstruction in pulmonary embolism (percentage of vascular obstruction on CT scans), Qanadli et al. proposed new CT index using following simple formula; Σ(n · d) / 40 × 100), where n is value of proximal thrombus in pulmonary arterial tree equal to number of segmental branches arising distally (minimum, 1; maximum, 20). And d is a kind of weighing factor depending on degree of obstruction (no thrombus, 0; partially occluded, 1; total occlusion, 2). For example, when pulmonary trunk is completely occluded, the score is 40 (maximum score; 20 point by weighing factor 2) and it is like complete occlusion of bilateral main pulmonary artery (10 point by weighing factor 2 by two main arteries). Right upper lobar artery supplies three segmental arteries, whereas left upper lobar artery supplies five segmental arteries. In contrast, right lower lobar artery covers seven segmental arteries, whereas left lower lobar artery covers five segmental arteries (Schema drawn in consideration of descriptive text from reference 39: Qanadli et al. AJR Am J Roentgenol 2001; 176: 1415-1420).RA = right atrial, LA = left atrial, PA = pulmonary artery, CT = computed tomography.
|
In several studies, the clot load measured by the use of Qanadli and colleagues’ method showed positive correlation with patients’ death4142 or hemodynamic severity.43 In contrast, Ghaye et al.44 and Araoz et al.45 reported that pulmonary artery (PA) clot load scores are poor predictor of mortality in patients with acute PE. While PA clot load scores can be an indicator of the severity of the current episode of PE or treatment effectiveness, they may not be used directly as an indicator of RV failure or death of the patients. Therefore, pulmonary vascular resistance may not be determined only with mechanical obstruction of the pulmonary arteries and their branches by intravascular clot loads, but also with vasoactive amines (released from plasma, platelets or tissue), reflex PA vasoconstriction, and systemic arterial hypoxemia occurring during acute PE.444647
Go to :
FREQUENCY OF ACUTE PE EVOLUTION TO CTEPH CORRELATED WITH INITIAL CLINICAL AND CTPA FEATURES
It has been known that residual thrombi and microscopic vasculopathy after the attack(s) of acute PE lead to CTEPH in 0.6% to 4.4% of acute PE patients (Fig. 10).4849 However, the real chronic CTEPH incidence after the episode of acute PE is not exactly known. According to a study, the incidence of CTEPH observed one year after the first episode of acute massive or submassive PE was approximately 6.9%.50 In other study, the cumulative two-year incidence of CTEPH was 8.6% (25/290 patients).51 In a Korean study, the incidence of CTEPH after acute PE was 6.1% (15/246 patients).52
 | Fig. 10Repeated attacks of acute pulmonary embolism without evolving into chronic thromboembolic pulmonary hypertension in a 72-year-old woman. (A, B) Transverse images of enhanced CT scans obtained at levels of bronchus intermedius (A) and right middle lobar bronchus take-off (B), respectively, and in January 2012, demonstrate filling defects in right proximal interlobar artery (arrow in A) and in bilateral lower lobar arteries (arrows in B). (C) Coronal reformatted image depicts filling defects in bilateral lower lobar arteries with railway-track sign (arrows). (D, E) Transverse images of enhanced CT scans obtained at levels of left inferior pulmonary vein (A) and subsegmental bronchi (B), respectively, and in November 2018, disclose filling defects in posterolateral basal trunk of right lower lobar pulmonary artery and anteromedial segmental artery of left lower lobe (arrows in D) and posterior basal segmental artery of right lower lobe and anteromedial basal segmental artery of left lower lobe (arrows in E). Between repeated attacks of pulmonary embolism, complete dissolution of emboli has been achieved with embolotherapy. Please note that even with repeated attacks of acute pulmonary embolism, chronic thromboembolic pulmonary hypertension features could not be seen on this follow-up CT. Chronic thromboembolic pulmonary hypertension has not occurred yet as of September 2021. None of the related clinical and CTPA features was related to the evolution to chronic thromboembolic pulmonary hypertension after acute embolic attack. Patient had no deep vein thrombosis; RV/LV ratio was lesser than 1.0 on CTPA; normal RV function on echocardiography; and absence of mosaic attenuation or lung infarction on CTPA.CT = computed tomography, CTPA = CT pulmonary angiography, RV = right ventricle, LV = left ventricle.
|
Large RV diameter with RV/LV ratio greater than 1.0, high baseline pulmonary arterial pressure and RV dysfunction were independent predictors of oncoming CTEPH (Fig. 4).51
On a CTPA-based study, the presence of an occlusive clot on initial imaging is associated with an increased probability of CTEPH development (Fig. 4). The presence of mosaic attenuation or lung infarction may also help predict CTEPH development.53 Acute PE patients with co-existing DVT are more serious clinically than those without DVT.32 Recurrent DVT or unprovoked PE was significantly associated with a higher risk of CTEPH, with odds ratios of 3.2 (95% CI, 1.7–5.9) and 4.1 (95% CI, 2.1–8.2), respectively.54
Go to :
MANAGEMENT OF ACUTE PE AND CTEPH
More aggressive treatment including systemic thrombolysis, catheter-directed therapy, and/or surgical embolectomy is warranted to rapidly restore pulmonary blood flow and prevent death. The decision to escalate therapy for submassive PE is controversial; data thus far have been generated most prominently for systemic thrombolysis and to a lesser extent for catheter-directed thrombolysis.23
In addition to indefinite anticoagulation, pulmonary endarterectomy (PEA) is the treatment of choice for CTEPH in patients who are considered operative candidates by having obstructing lesions in the main, lobar, segmental, and subsegmental arteries (Figs. 4 and 11).55 In approximately half of patients with CTEPH whose pulmonary vascular resistance is disproportionate to degree of vascular obstruction on CTPA may disclose severe distal microvasculopathy and regarded as ineligible for the surgery (Fig. 11).49
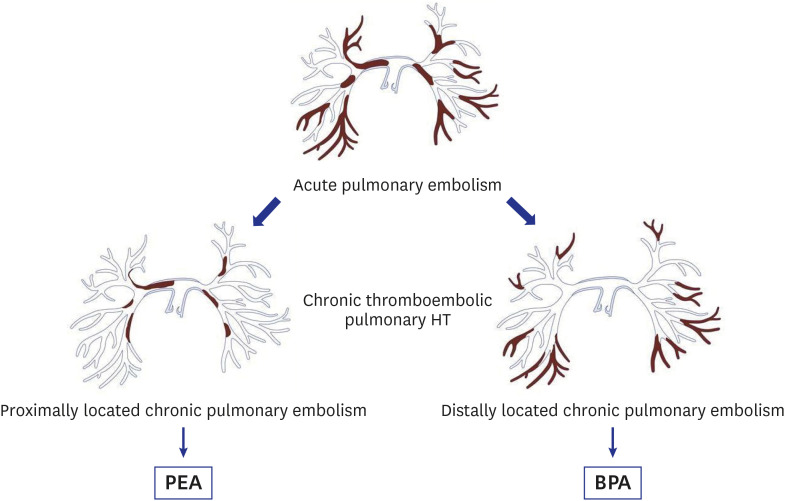 | Fig. 11Flowsheet for management of chronic thromboembolic pulmonary hypertension.When occlusive lesions are located centrally and patient condition is acceptable for surgery, PEA is performed. When occlusive lesions are mainly located peripherally, BPA is considered management method.
HT = hypertension, PEA = pulmonary endarterectomy, BPA = balloon pulmonary angioplasty.
|
Balloon pulmonary angioplasty (BPA) is an alternative therapy for patients with inoperable CTEPH.5657 By reviewing 500 consecutive procedures of BPA from 97 patients, the lesion distribution and characteristics evaluated were as follows: type A, ring-like stenosis lesion; type B, web lesion; type C, subtotal lesion; type D, total occlusion lesion; and type E, tortuous lesion.58 The success rate was higher, and the complication rate was lower, in ring-like stenosis and web lesions (Figs. 12 and 13). The total occlusion lesions had the lowest success rate. Tortuous lesions were associated with a high complication rate.
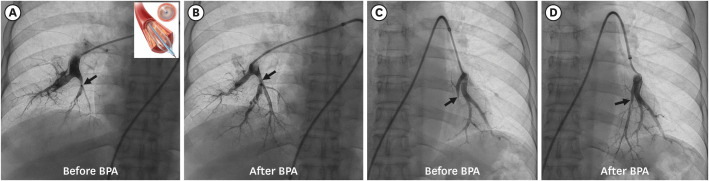 | Fig. 12Successful BPA for chronic thromboembolic pulmonary hypertension in a 71-year-old woman. (A) Right basal trunk pulmonary angiography shows web-like narrowing (arrow) of medial basal segmental artery of right lower lobe. Inset: balloon angioplasty device. (B) Follow-up angiography after angioplasty demonstrates narrowed segment is dilated with maintained arterial lumen (arrow). (C) Left basal trunk pulmonary angiography shows near complete occlusion (arrow) of medial basal branch artery of left lower lobe. (D) Follow-up angiography after angioplasty demonstrates occluded segmental lumen is penetrated and opened (arrow).BPA = balloon pulmonary angioplasty.
|
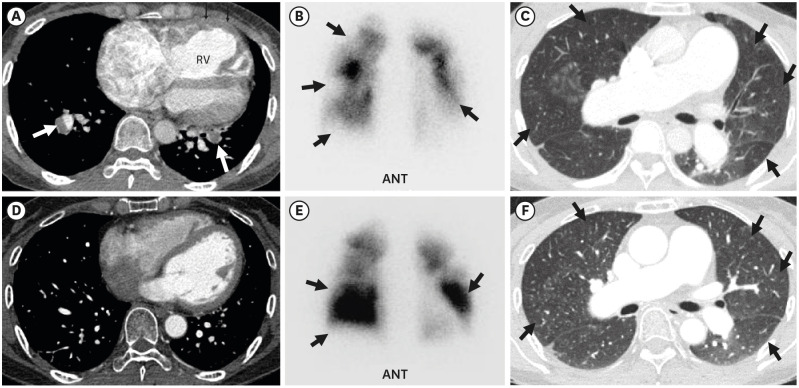 | Fig. 13Imaging features before and after balloon pulmonary angioplasty in a 56-year-old woman having chronic thromboembolic pulmonary hypertension. (A) Transverse image of enhanced CT scan obtained at basal segmental pulmonary artery level shows filling defects (arrows) in basal segmental arteries. Also note flattening of interventricular septum, RV enlargement, and RV wall thickening (small arrows). (B) Anterior view of perfusion scintigraphy demonstrates multiple areas (arrows)of perfusion defects in both lungs. (C) Lung window of CT scan obtained at distal main bronchus level depicts multiple areas (arrows) of perfusion deficiency and/or oligemia. Please compare lung attenuation and vascularity of this image with those of (F) (after balloon angioplasty). (D) Follow-up CT scan obtained at similar level to (A) shows reversal of interventricular septal morphology with normal right-sided bowing. Also note absence of filling defect in segmental pulmonary arteries. (E) Anterior view of follow-up perfusion scintigraphy after balloon angioplasty demonstrates perfusion improvement (arrows) particularly in lower lung zones. (F) Lung window of follow-up CT scan obtained at similar level to (C) and after balloon angioplasty depicts improved perfusion and vascularity (arrows) in bilateral lungs. Please compare perfusion and vascularity with those of (C).ANT = anterior, RV = right ventricle, CT = computed tomography.
|
Go to :
CONCLUSION
In acute PE, circulatory failure and systemic hypotension are clinically important for predicting poor prognosis. However, hemodynamically unstable PE accounts only a minority of all PE presentations. Even though PA clot load scores can be an indicator of the severity of the current episode of PE or treatment effectiveness, they may not be used directly as an indicator of RV failure or death of the patients. Other clinical predictors such as age > 70 years, coexisting congestive heart failure, or chronic obstructive pulmonary disease are also regarded as bad prognosis factors. Large RV diameter with RV/LV ratio greater than 1.0 and/or occlusive clot and pulmonary infarction on initial CTPA, and high baseline pulmonary arterial pressure and RV dysfunction are independent predictors of oncoming CTEPH.
Go to :
 XML Download
XML Download