

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prothrombotic disorder vaccine-induced immune thrombotic thrombocytopenia (VITT) has recently been observed in people vaccinated with the ChAdOx1 nCoV-19 adenovirus vector vaccine.12 VITT is a rare but life-threatening complication. Although the incidence is low, the number is not negligible, as of October 11, 2021, approximately 46.5% of the world’s population has received at least one dose of coronavirus disease 2019 (COVID-19) vaccine.3 Taking into account the increasing need for additional vaccination to reach the herd immunity threshold,4 VITT is considered a hurdle to the global vaccination program against severe acute respiratory syndrome coronavirus 2.
VITT strongly mimics auto-immune heparin-induced thrombocytopenia (HIT) and shares clinical features including thrombocytopenia, unusual thrombosis, and the presence of anti-platelet factor 4 (PF4) auto-antibodies.5 VITT evolves with the production of IgG antibodies to PF4, wherein the antibody-PF4 immune complexes activate platelets through FcγIIa receptors, resulting in consumptive coagulopathy including a decrease in the number of platelets and the activation of coagulation.6
Heparin is commonly used to prevent coagulation during hemodialysis. Therefore, nephrologists might encounter patients with end-stage kidney disease or acute kidney injury needing dialysis with a history of heparin exposure who developed thrombotic thrombocytopenia after vaccination.
In this report, we introduce a patient who experienced a thrombotic event with thrombocytopenia after the simultaneous exposure to the ChAdOx1 nCov-19 vaccine and heparin during hemodialysis.
Go to : 
CASE DESCRIPTION
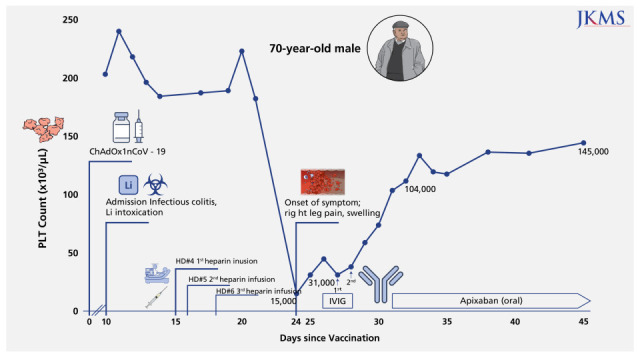
A 70-year-old man presented at the emergency department with altered mental status. He was unable to perform the activities of daily living due to generalized weakness, diarrhea, and poor oral intake for seven days. He had hypertension, diabetes mellitus, diabetic retinopathy, chronic kidney disease (stage 3, baseline serum creatinine (Scr) was confirmed 1.68 mg/dL two years ago) and bipolar affective disorder treated with lithium. He was vaccinated with the ChAdOx1 nCoV-19 vaccine 10 days previously. His blood pressure was 158/114 mmHg and his body temperature was 37.0°C. Physical examination revealed drowsy mental status, dehydrated tongue, decreased skin turgor, and mild lower abdomen tenderness. Upon admission, his hemoglobin was 12.0 g/dL, the white blood cell count was 9,000/µL, platelet count was 204,000/µL, prothrombin time international normalized ratio (PT INR) was 1.08 (reference range, < 1.2), and d-dimer was 0.54 µg/mL (reference range, < 0.50). Serum blood urea nitrogen (39.0 mg/dL), Scr (3.52 mg/dL), C-reactive protein (10.43 mg/L; reference rage, 0–5.0 mg/L), and lithium levels (2.81 mEq/L; reference range, 0.6–1.2 mEq/L) were analyzed. The twenty-four-hour urine test showed a protein of 14.1 g and albumin of 11.1 g. There was marked low-density wall thickening of the cecum and ascending colon on the abdominopelvic computed tomography (CT) scan, compatible with infectious colitis. Diffusion-weighted magnetic resonance imaging of the brain and electroencephalogram were unremarkable. Under a diagnosis of lithium intoxication, hemodialysis was initiated. After six hemodialysis sessions (hospital day 2–5, 7, and 8) using heparin from the 4–6th session (hospital day 5, 7, 8), the lithium level decreased to below the toxic level (0.25 mEq/L) and the patient’s mental status recovered. SCr was decreased to 1.37 mg/dL. Nine days after the first heparin use, the patient’s platelet count abruptly decreased to 15,000/µL and his right calf was swollen. Ultrasonography showed venous thrombi in the right common femoral vein, right superficial femoral vein, and right anterior tibial vein. The patient had evidence of disseminated intravascular coagulation (DIC), including elevated D-dimer level, low fibrinogen levels, a mildly increased PT INR, and an activated partial thromboplastin time (Table 1). Haptoglobin and total bilirubin levels were within the normal ranges. The ADAMTS 13 activity was 81.5%. The fluorescent antinuclear antibody test was positive (homogeneous pattern, 1:320). The extractable nuclear antigen (ENA) antibody panel including the antiphospholipid antibody and antiplatelet antibody were also negative. Despite the transfusion of platelet concentrates, the platelet counts remained low. Considering the deep vein thrombosis in combination with thrombocytopenia after COVID vaccination and also the recent exposure to heparin, the suspicion of VITT or HIT prompted the administration of intravenous immunoglobulin (IVIG).7 The platelet counts gradually increased to 104,000/µL after two days of IVIG infusion with the dose of 1g/kg of bodyweight (which in turn 60 g), and anticoagulation with apixaban at a reduced dose due to decreased renal function (Scr, 1.58 mg/dL) was initiated. Calf swelling was resolved, and the platelet count reached 145,000/µL 17 days after IVIG injection (Fig. 1). Anti-heparin PF4 IgG by both enzyme-linked immunosorbent assay (ELISA, LIFECODES PF4 IgG [Immucor]) (2.54 OD; reference range, < 0.4 OD) and the chemiluminescent immunoassay (analysis machine: ACL-TOP 700 [Werfen]; Reagent, HemosiL HIT-Ab [HemosiL]) (43.60 U/mL; reference rage, < 1.00 U/mL) was confirmed to be positive. The patient was discharged home while receiving oral apixaban.
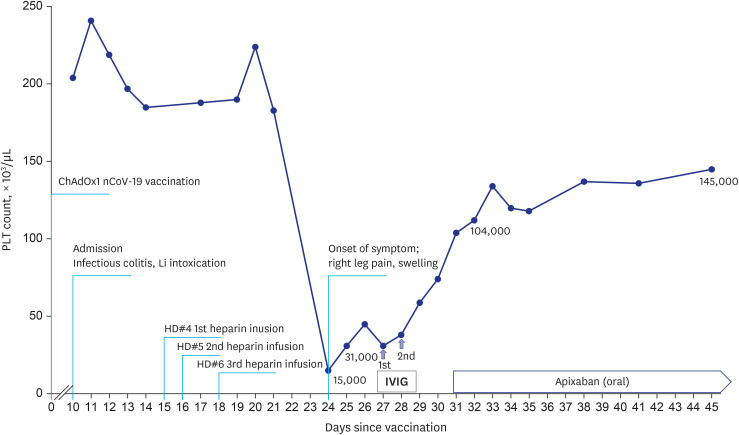 | Fig. 1Serial PLT counts are presented in order to clinical events. A 70-year-old man who had thrombotic thrombocytopenia was complicated by deep vein thrombosis of lower extremity after vaccination. After administration of intravenous immunoglobulin with dose of 1 g/kg for 2 consecutive days, the PLT count gradually rose to 104,000/µL.PLT = platelet, IVIG = intravenous immunoglobulin.
|
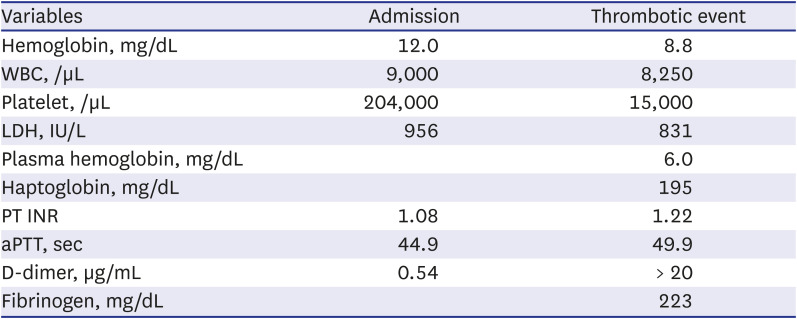
Table 1
Disseminated intravascular coagulation profile at admission and thrombotic event
Reference range: LDH, 238– 422 IU/L; PT INR, < 1.2; aPTT, 30.7–43.0 seconds; D-dimer, < 0.50 µg/mL; Fibrinogen, 225–457 mg/dL.
WBC = white blood cell, LDH = lactate dehydrogenase, PT INR = prothrombin time international normalized ratio, aPTT = activated partial thromboplastin time.
![]()
Go to :
DISCUSSION
In the UK Medicines and Healthcare Products Regulatory Agency (MHRA)’s Yellow Card Weekly Report, as of October 6, 2021, the incidence of VITT was reported to be 15.2 per million episodes. In those aged 18–49 years, the incidence was reported to be 20.9 per million episodes, and in those over 50 years old, the rate was reported to be 10.9 per million episodes.8
The World Health Organization (WHO)’s classification of VITT following a COVID-19 vaccination is established by the degree of conviction. It includes three mandatory criteria of 1) vaccinated against COVID within 30 days, 2) no substitute etiology for the condition, and 3) thrombosis with thrombocytopenia. To confirm the diagnosis, other causes of thrombocytopenia or thrombosis should be ruled out. The other causes of thrombocytopenia include infections, malignancy, medications, hematologic disorders like thrombotic microangiopathy and idiopathic thrombocytopenic purpura, and hematologic manifestations of rheumatic diseases.9
In this case, an abrupt decrease in the platelet count and the development of thrombosis occurred while the patient was recovering from infectious colitis. Therefore, it was difficult to consider that it was elicited by infection-related DIC. No schistocytes were seen on the peripheral blood smear, and stable hemoglobin levels and preserved ADAMTS 13 activity did not support thrombotic thrombocytopenic purpura or atypical hemolytic uremic syndrome. There was no evidence of rheumatic disease and ENA antibody panel including the antiphospholipid antibody were negative. Chest and abdominopelvic CT scans showed no evidence of malignancy.
The diagnosis in the current case was complicated by the use of heparin in the hemodialysis session. Thrombotic thrombocytopenia developed 24 days after vaccination and at the same time, nine days after first heparin use. Both VITT and HIT are characterized by thrombocytopenia, thrombosis, and a positive anti-PF4 antibody test.3 The PF4 autoantigen is a polyanion molecule and can interact with negatively charged bacterial cell walls, DNA molecules, and heparin. PF4 interacts with the double-stranded DNA of the DNA vector vaccine, causing internalization of the viral nucleic acid/PF4 complex by antigen-presenting cells with increased PF4 autoantibody production.10 Because rapid immunoassays for anti-PF4 antibodies are not sensitive, guidelines recommend not using them and using ELISA to diagnose VITT.9 In this case, the anti-PF4 Ab was positive on the ELISA and immunoassays.
Despite the presence of overlapping manifestations, the typical clinical features are distinct. HIT usually occurs 5 to 14 days after heparin exposure. Deep venous thrombosis in vascular beds damaged by catheters and pulmonary embolism are the most common sites of venous thrombosis. Thrombocytopenia in HIT is usually moderate, with median platelet counts in the range of 50–70 × 109/L. Severe thrombocytopenia (platelets < 20 × 109/L) is unusual and can occur as fulminant thrombotic disease and consumptive coagulopathy.1112 In cases of VITT, the reported median time from vaccination to symptom onset was 8 to 9 days with a range of 1 to 37 days. VITT could be confirmed if thrombosis was present in the cerebral or splanchnic veins or multiple organs. However, probable VITT could be diagnosed if thrombosis was present in the pulmonary arteries or veins, limb veins, coronary arteries, cerebral arteries, or other arteries or veins with severe thrombocytopenia (platelets < 20 × 109/L).8 The majority of patients showed severe thrombocytopenia and the median nadir platelet count was approximately 20 × 109/L.5
A review of 44 VITT patients compared patients with favorable outcomes (recovery or full recovery) to those with unfavorable outcomes (death) and a cutoff nadir platelet count of 22,000/µL had significant value for predicting death.13 In this case, the patient’s clinical course was improving despite severe thrombocytopenia below the suggested cutoff. The risk of death in VITT was independently related not only to the degree of thrombocytopenia but also to the presence of intracranial hemorrhage.2 Recently, differences between binding sites and the binding kinetics of VITT antibodies and HIT antibodies to PF4 have been reported.14 The findings suggest the possibility of determining VITT with HIT by the type of PF4 antibody present.
In conclusion, there were no definitive diagnostic tools capable of differentiating between VITT and HIT in this patient. In this case, thrombocytopenia was abruptly initiated on nine days after the first heparin use and not recovered after discontinuation of heparin. In addition, the degree of thrombocytopenia was severe, it can be considered closer to VITT. Although VITT and HIT share treatment with IVIG and non-heparin anticoagulation, it is crucial to distinguish one from the other because immunization to COVID-19 from a public health perspective should be done in all individuals without clear contraindications, including VITT. Distinguishing between VITT and HIT will make it possible to establish a follow-up vaccination plan in a person who has had a thrombocytopenic thrombotic event. Further research is needed to develop the tools to make a clear distinction between the clinical syndromes.
Go to :
 XML Download
XML Download