

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vibrio vulnificus is a gram-negative, halophilic bacterium belonging to the genus Vibrio and family Vibrionaceae. It is commonly found in warm seawater and proliferates at a water temperature of ≥ 20ºC.12
V. vulnificus is an important opportunistic pathogen that can induce primary septicemia through the consumption of contaminated raw or undercooked seafood or wound infection through the exposure of a wound to warm seawater inhabited by the organism.234
V. vulnificus is naturally present in estuarine environments and coastal waters and is commonly found in oysters and molluscan shellfish.56 It is a major pathogen that accounts for 95% of all seafood-related deaths in the United States and has the highest fatality rate among foodborne pathogens.67
In patients with chronic liver disease, especially cirrhosis, V. vulnificus infection is a highly lethal condition that usually manifests 1–2 days after exposure to the organism.8 Although the infective or lethal dose of V. vulnificus in humans is unknown, host susceptibility is an important factor in this infection.9 Immunocompromised patients, including those with chronic liver diseases and cancer, have an increased risk of infection and complications.4
V. vulnificus infection has been reported in some coastal cities in the United States, Japan, and Taiwan,10 as well as in France, Demark, Israel, Germany, and Greece.11
V. vulnificus infection is a serious public health concern in Korea, as it occurs annually in the summer and has a high case fatality rate of approximately 50%.5 In Korea, V. vulnificus infection has been monitored since its legal designation as a national notifiable disease on August 1, 2000, and reporting of confirmed or suspected cases is mandatory. However, although there have been some studies on the epidemiology of V. vulnificus infection in Korea,1213 many of its epidemiological characteristics remain unknown.
The present study was designed to analyze the incidence of all notified cases of V. vulnificus infection by time, place, and person from 2001 to 2016, to identify the epidemiologic features and to estimate the case fatality rate using a case epidemiological investigation report by the Korea Centers for Disease Control and Prevention (KCDC, currently Korea Disease Control and Prevention Agency).
METHODS
The scope of the mandatory reporting of V. vulnificus infection, a legally designated infectious disease, covers confirmed or suspected infections. According to the surveillance manual for national notifiable diseases from the KCDC,14 confirmed cases were defined as cases where patients showed clinical symptoms matching the definition of V. vulnificus infection and confirmed by laboratory testing, whereas suspected cases were defined as cases where patients showed clinical symptoms matching the definition of V. vulnificus infection with epidemiological association but were negative on laboratory tests. In this study, we included all reported cases of V. vulnificus infection.
From 2001 to 2016, 913 cases of V. vulnificus infection were identified (835 confirmed and 78 suspected). We estimated the yearly, monthly, and regional incidence of all 913 cases.
In addition to the surveillance data reported to the KCDC, the number of patients who were under the National Health Insurance Service (NHIS) during the study period was collected by year, month, and region. Seawater temperature data for the study period were provided by the Korea Oceanographic Data Center of the National Institute of Fisheries Science.
The standard case report form of epidemiological investigation for V. vulnificus infection was launched in 2003, and a follow-up investigation protocol was launched in 2011 to determine the outcome of cases. We analyzed the standard epidemiological investigation forms of all 761 cases from 2003 to 2016 to determine the detailed demographic factors, clinical features, source of infection, and distribution of underlying diseases. The 152 reported cases who could not be followed up were excluded from the analysis. From all 761 notified cases (696 confirmed and 65 suspected) between 2003 and 2016, we identified the general characteristics (sex, age, occupation, and region of residence), clinical characteristics (date of onset, clinical symptoms, and signs), underlying diseases, source of infection (place of infection, history of seafood consumption, and history of seawater exposure), lifestyle (drinking and smoking status), and outcome (death or survival) of the cases.
Statistical analysis
The incidence rate was calculated as the newly notified number divided by 100,000, according to a specific year or region. The case fatality rate was calculated as the proportion of deaths (%) among all reported cases. Frequency analysis was performed to identify descriptive epidemiological features according to time, place, and personal characteristics. Frequency analysis was also used to compare the number of V. vulnificus infection cases reported to the KCDC with the number of patients under the NHIS.
RESULTS
Incidence rate of V. vulnificus infection
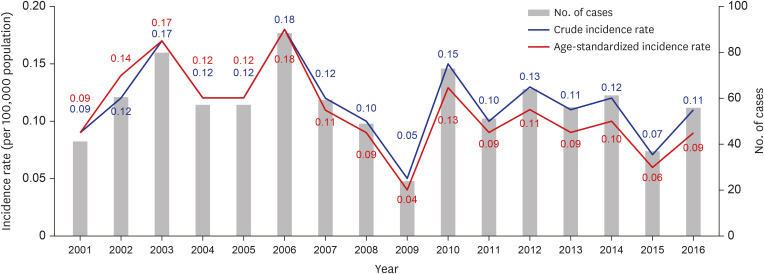
In total, 913 cases were reported between 2001 and 2016. The average crude incidence rate during this period was 0.12 ± 0.03 per 100,000 population, with the highest rate reported in 2006 (0.18), followed by 2003 (0.17), 2010 (0.15), and 2012 (0.13), with the lowest in 2009 (0.05). The age-standardized incidence rates in these years showed a similar pattern (Fig. 1).
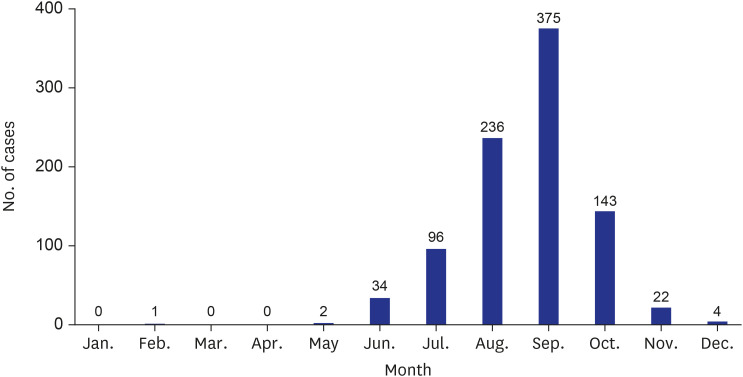
The incidence of V. vulnificus infection showed a high seasonality during the study period. The number of monthly cases was the highest in September (n = 375, 41.1%), followed by August (n = 236, 25.8%), October (n = 143, 15.7%), and July (n = 96, 10.5%), showing that the cases were concentrated between August and October. Few cases were reported between January and May (Fig. 2).
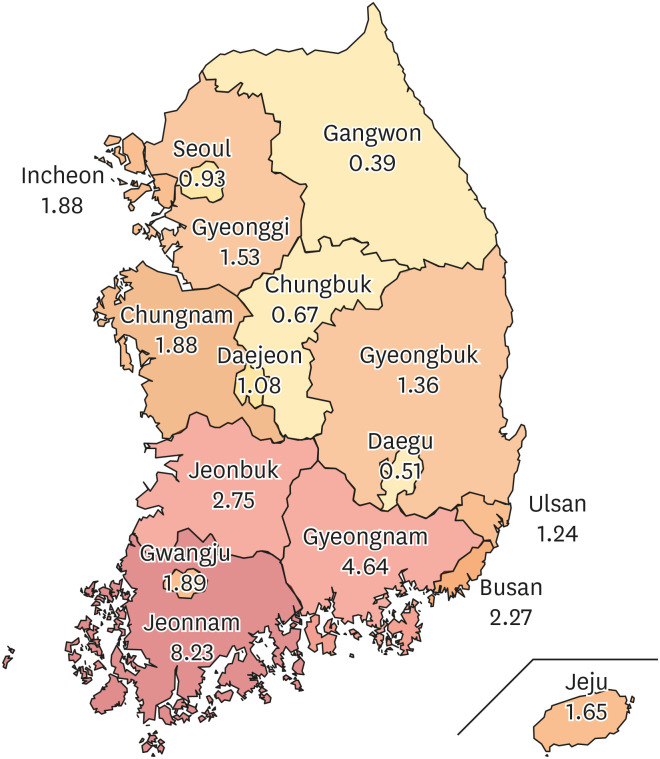
The risk of infection varies regionally. Among the 16 regions in Korea, the incidence rate per 100,000 population was the highest in Jeonnam (8.23), followed by Gyeongnam (4.64), Jeonbuk (2.75), and Busan (2.27) (Fig. 3).
From 2001 to 2016, the age-standardized incidence rate by region, adjusted for the mid-year resident population in 2005, was the highest in Jeonnam for 11 years. The age-standardized incidence rate per 100,000 population was the highest in 2003 (1.73), followed by 2002 (0.77), 2006 (0.58), and 2014 (0.55).
Analysis of the number of V. vulnificus infection patients claimed to the NHIS
The two institutions (KCDC and NHIS) had the highest number of patients in 2012 (64 and 66, respectively) (Supplementary Table 1). Both institutions (KCDC and NHIS) had the highest number of patients in September (137 and 105, respectively), followed by August (77 and 68, respectively). The number of V. vulnificus infection cases reported to the KCDC was the highest in Gyeonggi Province, followed by Jeonnam Province. The number of V. vulnificus-infected patients under the NHIS was the highest in Jeonnam, followed by Seoul and Gyeonggi Province.
Analysis of coastal seawater temperature
For 16 years from 2001 to 2016, when V. vulnificus infection cases occurred, the monthly average seawater temperature ranged from 11.5°C to 24.1°C (Supplementary Fig. 1).
When the number of V. vulnificus infection cases began to increase in earnest in July, the seawater temperature gradually increased, and the average seawater temperature in August was the highest at 24.1°C. The average seawater temperature in September, when the most number of cases occurred, was 23.1°C. As the average seawater temperature decreased from October, the number of cases also decreased.
Epidemiologic characteristics
Among the 761 patients who had completed standard epidemiological investigation forms from 2003 to 2016, there were more male patients (85.7%), and the predominant age group was 40–64 years (71.7%). The most common occupational category was unemployed (housewives: 47.6%). Regarding lifestyle factors, 486 (79.8%) patients were alcohol consumers (Table 1).
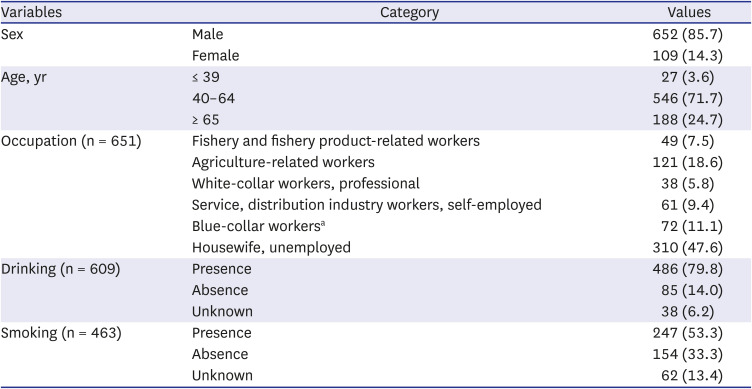
Table 1
General characteristics of cases of Vibrio vulnificus infection (N = 761)
Values are presented as number (%).
aBlue-collar workers include simple laborers in the fields of construction, civil engineering, and architecture.
![]()
Among the 761 patients, fever was the most common symptom (48.2%). In the 91 respondents who specified the site of pain, the most common pain sites were the lower limbs (61 cases, 67.0%), followed by the feet (10 cases, 11.0%), upper limbs (5 cases, 5.5%), both upper and lower limbs (5 cases, 5.5%), whole body (4 cases, 4.4%), hands (4 cases, 4.4%), and chest (2 cases, 2.2%). Hypotension occurred in a third of patients (35.0%). The site of edema was specified by 140 patients. The most common site of edema was the lower limbs (108 cases, 77.2%), followed by the upper limbs (11 cases, 7.9%), both upper and lower limbs (6 cases, 4.3%), feet (6 cases, 4.3%), whole body (3 cases, 2.1%), hands (3 cases, 2.1%), and hands and feet (2 cases, 1.4%). One patient (0.7%) complained of scrotal edema (Table 2).
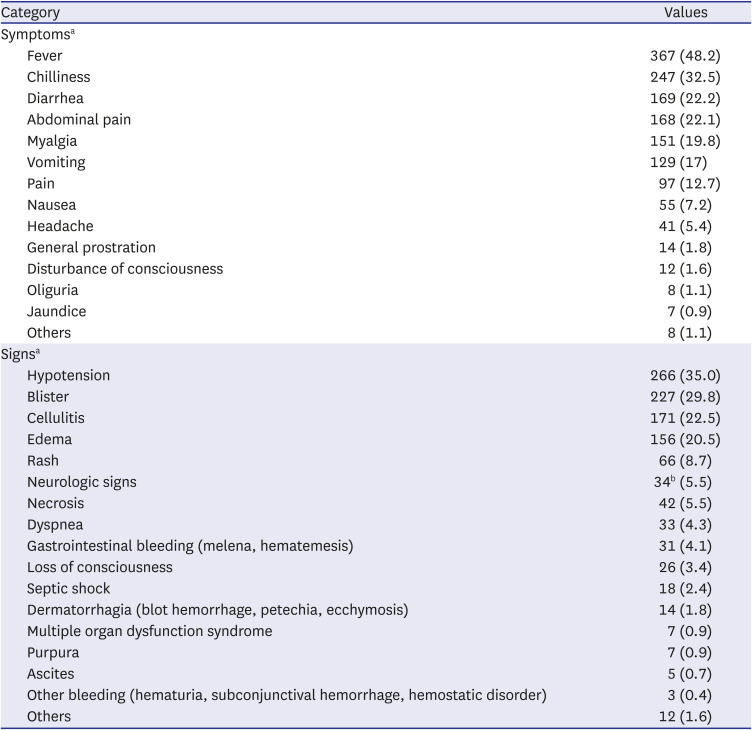
Table 2
Clinical symptoms and signs in cases of Vibrio vulnificus infection (N = 761)
Values are presented as number (%).
aMultiple responses were allowed for symptoms and signs in the case epidemiological investigation form; bDizziness: 13 cases; Paresthesia: 5; Paralysis: 5; Convulsion: 4; Dysphasia: 3; Seizure: 1; Cognitive disorder: 1; Disesthesia: 1; Delirium: 1.
![]()
Of the 691 patients with V. vulnificus infection who answered the question about underlying diseases, 664 (96.1%) reported having an underlying disease (Table 3). The most common underlying disease was liver cirrhosis (56.3%). Among the 89 patients with other liver diseases, 33 (37.1%) had alcoholic liver disease and five (5.6%) had fatty liver disease.
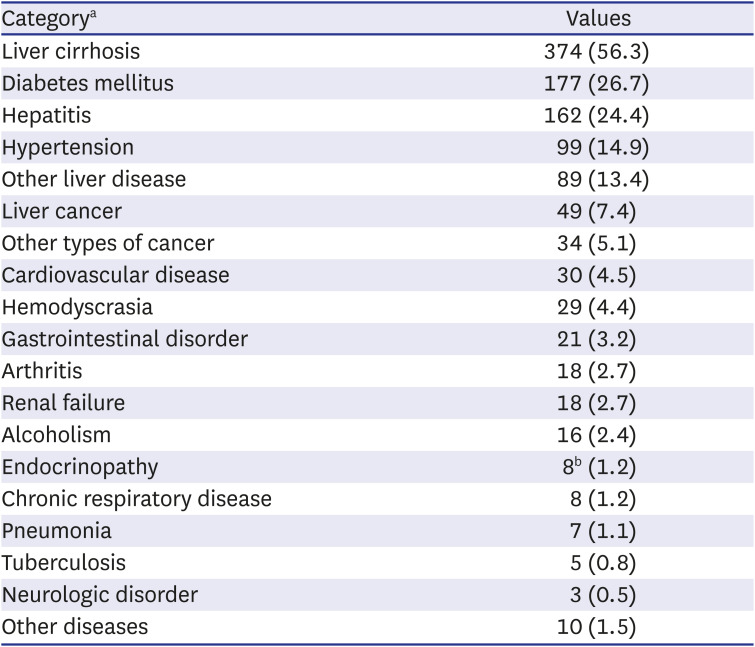
Table 3
Underlying diseases in cases of Vibrio vulnificus infection (N = 664)
Values are presented as number (%).
aMultiple responses were allowed for underlying disease in the case epidemiological investigation form; bHypothyroidism 4 cases, Hypocorticalism 2 cases, Hyperthyroidism 1 case, Cushing’s syndrome 1 case.
![]()
In the 655 cases in which the source of infection was evaluated, the most common source was raw seafood consumption (90.1%), followed by seawater exposure (5.8%) and both raw seafood consumption and seawater exposure (4.1%).
Sex (P = 0.045), age (P = 0.003), and liver disease presence (P = 0.035) showed a statistically significant difference with the route of infection; men (91.0%), patients under 64 years old (91.5%), and patients with liver disease (91.8%) had been infected mainly through seafood consumption.
Regardless of the region of residence, the most common region exposed to V. vulnificus was Jeonnam (24.3%), followed by Gyeongnam (15.6%), Gyeonggi (10.7%), and Incheon (9.5%). Five patients were considered to have acquired the infection in foreign countries, four through seafood consumption (two in China, one in Vietnam, and one in the Philippines), and one through seawater exposure (in Indonesia). Epidemiological reports from 2011 to 2016 show that 159 of 325 notified cases of V. vulnificus infection resulted in death, which represents a fatality rate of 48.9%. The fatality rate was the highest in 2014 (65.6%) and the lowest in 2016 (21.4%).
DISCUSSION
V. vulnificus infection occurs annually in Korea with regional and seasonal features. In our analysis of the cases of V. vulnificus infection from 2001 to 2016, the incidence rate was 0.12 ± 0.03 per 100,000 population, with the highest incidence (8.23) recorded in the Jeonnam region. V. vulnificus infection mostly occurs sporadically in the United States. From 1998 to 2007, 276 cases of V. vulnificus infection were reported in Florida, with an average annual incidence rate of 1.6 per 1 million.15 In Japan, 12–24 cases of V. vulnificus infection have been reported annually.16 In Taiwan,17 the estimated prevalence of V. vulnificus infection from 1985 to 2000 was 0.35–1.24 per 1 million, with the largest number of cases reported in 2000 (n = 26).
In our study, the largest number of cases occurred in September (41.1%), and 82.6% of all cases occurred between August and October. Similarly, most cases of infection in the United States were reported between April and October, which are the months during which the organism flourishes.18 In Japan, 81.1% of the cases were reported between July and September,19 with the greatest number reported in July.16 In Taiwan, almost all cases occurred between late spring and early fall (April through October), a period during which the seawater temperature ranges from 20°C to 29°C.17
In a previous study,20
Vibrio spp. isolated from the environments of the southern coastal tidal water and mud samples of South Korea showed species-specific seasonal patterns, with V. vulnificus limited to summer. Therefore, the results of this previous study20 support the results of our study, which showed that V. vulnificus infection cases occurred intensively in August and October, and the incidence rate per 100,000 population was the highest in Jeonnam (8.23).
It can be assumed that the warm seawater temperature affected the incidence. A previous study,21 showed a positive relationship between seawater temperature and V. vulnificus cases and the relative risks of V. vulnificus infection in the south, west, and east coasts according to the 1°C increase in seawater temperature were 1.35 (95% confidence interval [CI], 1.19–1.53), 1.34 (95% CI, 1.20–1.51), and 1.30 (95% CI, 1.06–1.59), respectively.
According to a previous study on cases reported in Florida from 1981 to 1992,22 oyster consumers with liver disease had 80 times higher risk of V. vulnificus infection. In this study, the risk of V. vulnificus infection was associated with male sex (85.7%), older age (96.5% > 40 years), and underlying disease (96.1%). Similar demographic characteristics have been reported in the United States,23 Taiwan,17 and Japan.19 Leng et al.10 reported that the higher infection rate among men (86.1%) is attributable to higher alcohol use and a higher percentage of occupational exposure to seawater and seafood.24 In our study, 96.1% of the cases had an underlying disease, with liver cirrhosis (56.3%) being the most common, followed by diabetes mellitus (26.7%). In a study that investigated 37 cases in the Ariake Sea region in Japan between 1984 and 2008, 91.6% of the patients had liver disease.19 In a Taiwanese study that investigated 84 patients between 1995 and 2000, over 80% of the patients had liver disease, mainly caused by hepatitis B or C infection, followed by diabetes and steroid use.17 The most common comorbidities among patients with V. vulnificus infection in the United States were heart disease (34%), diabetes mellitus (23%), alcohol consumption (22%), and liver disease (20%).23
In Korea, seafood consumption is the most common (90.1%) route of V. vulnificus infection, resulting in primary sepsis. In a Japanese study, 31 of 37 (83.8%) patients consumed raw seafood, and the remaining six patients had an unknown route of infection, with no clear cases of infection through wound sites.19
In our study, 81.2% of the patients with an underlying disease had liver disease (liver cirrhosis, hepatitis, or liver cancer). These patients most frequently contracted the pathogen through seafood consumption, whereas patients without liver disease most frequently contracted the pathogen through seawater exposure, with the difference being statistically significant (P = 0.035). As liver disease is a potent predictor of death in all patients, a dysfunctional liver is reported to impose an additional risk through an independent mechanism of transferrin saturation or iron overload.24 Because of the strong correlation between liver disease and death, previous studies recommended that patients with liver disease should refrain from activities that involve seawater exposure if they currently have a wound or are likely to sustain a wound injury.2223
In our study, 159 of 325 patients with V. vulnificus infection died (48.9%). In a Taiwanese study of 84 patients with V. vulnificus infection between 1995 and 2000, 25 patients died (29.8%), 57 patients survived (67.9%), and two patients had an unknown status (2.3%).17 In a study in Japan, 24 of 37 patients died (64.9%).19 Yun et al.12 reviewed the clinical data of 34 patients in a Korean hospital between 2000 and 2011, among whom 16 patients (47.1%) died.
In the USA and Korea, V. vulnificus infection is a nationally notifiable disease, but there is no obligation to report it in Japan.16 The Centers for Disease Control and Prevention in the USA monitors vibriosis through the nationwide Cholera and Other Vibrio Illness Surveillance (COVIS) system since 1988 and the 10-state Foodborne Diseases Active Surveillance Network (FoodNet) since 1996.25 COVIS is a passive surveillance system to which all states can report laboratory-confirmed Vibrio infections, and FoodNet conducts an active, population-based surveillance in ten states for all laboratory-confirmed Vibrio infections, as well as other enteric infections transmitted commonly through food.25 The three commonly reported Vibrio species were V. parahaemolyticus, V. vulnificus, and V. alginolyticus, and in both systems, most hospitalizations and deaths were caused by V. vulnificus infection.25 In Korea, since 2000, a passive report-based national notifiable infectious disease surveillance system has been operated to notify suspected and confirmed cases of V. vulnificus infection. Since 2002, laboratory surveillance for pathogenic Vibrio (vibrioNet) has been conducted to monitor the distribution status of three pathogenic Vibrio species (V. vulnificus, V. cholerae, and V. parahaemolyticus) and changes in marine environmental factors (seawater temperature, salinity, pH, turbidity).
From the seawater temperature analysis provided by KCDC from 2001 to 2016, the seawater temperature in August was the highest at 24.1°C. However, in September, when the seawater temperature was 23.1°C, the number of cases was the highest at 375. During the same period, 850 (93.1%) of 913 notified cases occurred between July and October, and the average seawater temperature between July and October was 22.1°C. Therefore, the occurrence of V. vulnificus infection in our study showed a distinct seasonality due to seawater temperature, and it occurred more often in people with underlying diseases such as liver cirrhosis; therefore, host factors can also affect the occurrence of disease.
V. vulnificus infection surveillance results showed a monthly average of 57 V. vulnificus infection cases, but given the passive reporting system and the number of cases where patients died without treatment or diagnosis, it has been reported that the actual number of cases could be much higher than this.26 From 1981 to 1987, among V. vulnificus patients reported in Florida, USA, the case fatality rates of those with and without liver disease were similar at 52% and 62%, respectively.27 In our study, the case fatality rates of V. vulnificus infection cases with and without liver disease were 51.2% and 42.5%, respectively, and there was no statistically significant difference (χ2 = 1.65, P = 0.199). In the future, a retrospective study is needed to identify possible risk factors that may affect mortality by analyzing the medical records of cases.
Our study analyzed all notified cases from investigation reports between 2003 and 2016 in Korea; however, we could not include data on patients’ blood tests, antibiotic use, and specific treatment in our analysis because of the lack of such information in epidemiological reports.
In conclusion, considering the high fatality rate associated with V. vulnificus, it is important to establish public health measures to prevent V. vulnificus infection. To lower the incidence of, and death from, V. vulnificus infection, it is important to increase awareness among people at high risk, especially those living in high-risk areas. The public health approach should emphasize the prevention of V. vulnificus infection.6 Moreover, important approaches for reducing the disease burden include education and prevention strategies.24 The Taiwanese government requires food companies to provide warning labels on seafood containers, menus, and public health brochures.17 Therefore, additional research needs to be conducted in the future.
 XML Download
XML Download