

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal polyps are the most common cause of isolated hematochezia in children.1234 However, in clinical settings, anal fissures may also present with isolated hematochezia. Therefore, distinguishing colorectal polyps from anal fissures may often be difficult, especially when the findings of anal inspection and digital rectal exam are negative. Ulcerative colitis (UC) may also present with isolated hematochezia, especially in those whose lesions are confined to the rectum.5 In these cases of isolated hematochezia, a colonoscopy or sigmoidoscopy is required. However, there are limitations in performing endoscopy in pediatric patients, especially in infancy or childhood.
Fecal calprotectin (FC) is a surrogate marker that is popularly used for assessing intestinal inflammation in patients with inflammatory bowel disease.67 However, consensus has not been established for the clinical use of FC in colorectal polyps due to the lack of baseline data.8 Meanwhile, recent studies have shown that FC may have a role in detecting and furthermore monitoring recurrence in colorectal polyps.9101112 Considering the aforementioned conditions of children presenting with isolated hematochezia, FC may be able to discriminate colorectal polyps from different diseases and conditions before conducting an endoscopy.
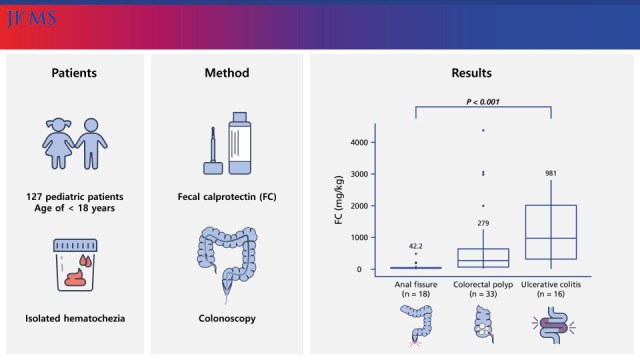
In this study, we aimed to investigate the potential utility of FC in assessing colorectal polyps detected by colonoscopy among children presenting with isolated hematochezia.
Go to : 
METHODS
Patients and study design
The present study was a multicenter, retrospective, cross-sectional study conducted in 15 medical centers in South Korea; Kyungpook National University Children’s Hospital affiliated with Kyungpook National University Chilgok Hospital, Ajou University Medical Center, Eulji University Hospital, Chungnam National University Hospital, Soonchunhyang University Bucheon Hospital, Korea University Anam Hospital, Keimyung University Dongsan Hospital, Nowon Eulji Medical Center, Hallym University Sacred Heart Hospital, Jeonbuk National University Medical School, Kosin University Gospel Hospital, Wonju Severance Christian Hospital, Kyungpook National University Hospital, Chung-Ang University Hospital, and Inje University Ilsan Paik Hospital. Pediatric patients of the age of < 18 years who had undergone a colonoscopy for isolated hematochezia from June 2016 to May 2020 were included. Medical charts were reviewed and those with symptoms other than hematochezia, or who were previously diagnosed with a gastrointestinal tract disease were excluded. Additionally, those who had not conducted FC tests within 1 month before the colonoscopy were also excluded to control for alteration of FC levels owing to disease progression. The etiologies of isolated hematochezia were investigated. Thereafter, those with the diagnosis of colorectal polyps, anal fissures, and UC were ultimately included for statistical analysis.
Baseline clinicodemographics including sex, diagnosis age, family history of colorectal polyps, growth indicators, serum laboratory test results, and fecal test results including FC and fecal immunochemistry test (FIT) were investigated in all the patients with available data. FC level was analyzed using an enzyme-linked immunosorbent assay in 3 centers, while fluorescence immunoassay was conducted in 12 centers. Patients were divided according to diseases, and variables were compared between the following three diseases; colorectal polyps, anal fissure, and UC. Furthermore, FC level cut-off levels that could possibly discriminate colorectal polyps from anal fissures and UC were investigated.
Statistical analysis
For statistical comparison between the three groups, analysis of variance test and post-hoc Bonferroni t test was used for continuous variables, and chi square test or Fisher’s exact test was used for categorical variables. Wilcoxon’s rank-sum test was used for the comparison of FC levels between two groups. Comparative data for continuous variables are reported as median (interquartile range) or mean ± SD. Receiver operating characteristic (ROC) curve analysis was performed to derive the most accurate FC cut-off points associated with the diagnosis of colorectal polyps. The results were expressed as area under the curve (AUC) with 95% confidence interval (CI), and sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. Data were considered to be statistically significantly different if P < 0.05. Statistical analyses were conducted using R version 3.2.3 (http://www.r-project.org).
Ethics statement
The present study was conducted with approval from 16 participating institutions including the Institutional Review Board (IRB) of Kyungpook National University Chilgok Hospital (IRB No. 2020-07-017), and informed consent was waived due to the retrospective nature of the study.
Go to :
RESULTS
Patients
Among 1,036 children during the study period, 909 patients were excluded leaving 127 patients for inclusion. Colorectal polyp was the most common etiology of isolated hematochezia, comprising 27.6% of all etiologies followed by anal fissure (14.2%), and UC (12.6%) (Table 1).
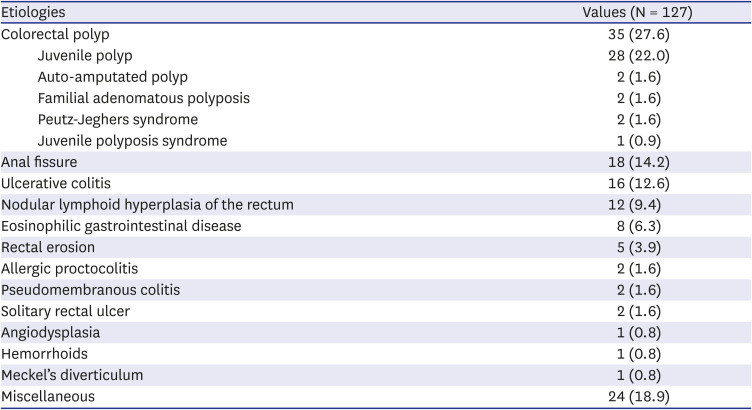
Table 1
Etiologies of isolated hematochezia
![]()
Comparison of findings between groups of colorectal polyp, anal fissure, and UC
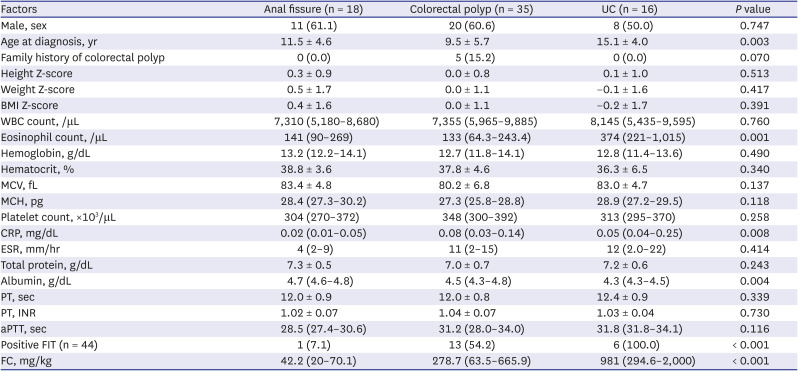
A total 69 patients with colorectal polyp, anal fissure, and UC were divided into three groups. Two patients with auto-amputated polyps were additionally excluded, ultimately leaving 67 patients for statistical analysis (Fig. 1). Clinicodemographic findings and laboratory test results were statistically compared between the three groups. Comparison between groups revealed statistically significant differences between the three groups in age at diagnosis, eosinophil count, C-reactive protein, serum albumin, proportion of patients with a positive FIT, and FC levels (Table 2, Fig 2). According to the post-hoc Bonferroni t test, significant differences in FC levels were observed between the anal fissure group and the colorectal polyp group (P = 0.048), and between the anal fissure group and the UC group (P = 0.002).
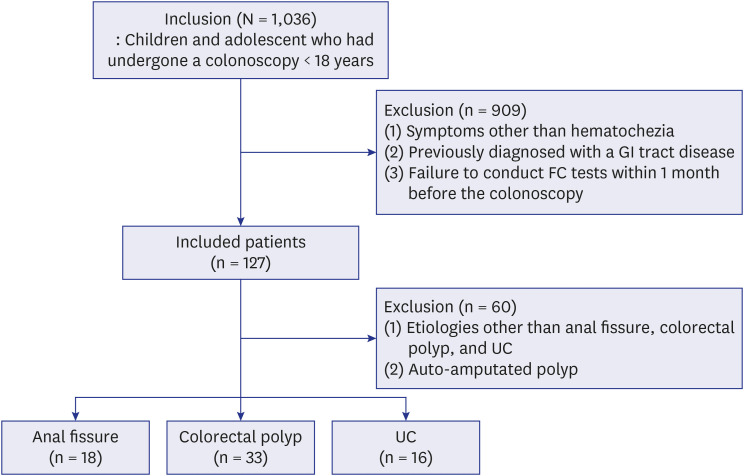 | Fig. 1Patient inclusion and exclusion.GI = gastrointestinal, FC = fecal calprotectin, UC = ulcerative colitis.
|
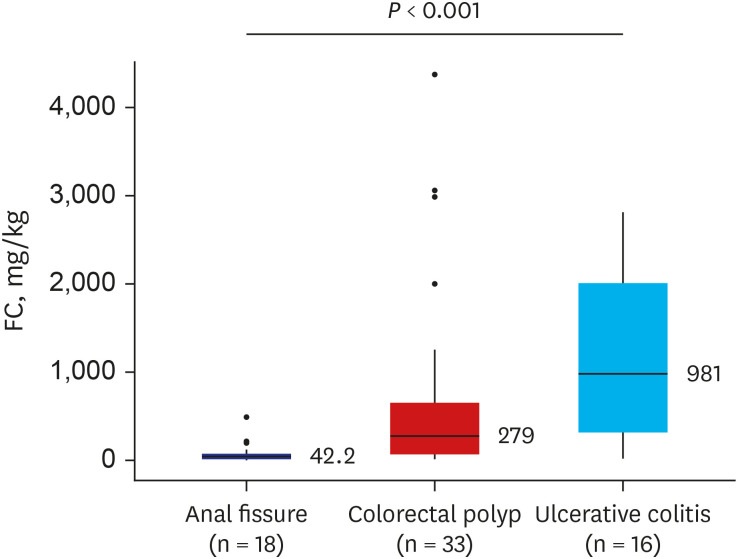 | Fig. 2Significant FC level differences between major etiologies of isolated hematochezia.FC = fecal calprotectin.
|
Table 2
Comparison of clinicodemographic, laboratory factors between anal fissures, juvenile polyps, and UC
Data are expressed as means ± SD for continuous variables that showed normal distribution, and median (interquartile range) or number (%) for continuous variables that did not show normal distribution, unless otherwise indicated.
UC = ulcerative colitis, BMI = body mass index, WBC = white blood cell, MCV = mean corpuscular volume, MCH = mean corpuscular hemoglobin, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, PT = prothrombin time, INR = International Normalized Ratio, aPTT = activated partial thromboplastin time, FIT = fecal immunochemistry test, FC = fecal calprotectin.
![]()
Cut-off level for the discrimination between colorectal polyps and other major etiologies
According to ROC curve analysis, the most accurate FC cut-off level for the discrimination between colorectal polyp and anal fissure was 225 (AUC, 0.8; 95% CI, 0.678–0.923; sensitivity, 59.4%; specificity, 94.4%; PPV, 95.0%; NPV, 56.7%; P < 0.001) (Fig. 3A). According to ROC curve analysis, the most accurate FC cut-off level for the discrimination between colorectal polyp and anal fissure was 879 (AUC, 0.687; 95% CI, 0.521–0.852; sensitivity, 81.2%; specificity, 56.2%; PPV, 78.8%; NPV, 60.0%; P < 0.001) (Fig. 3B).
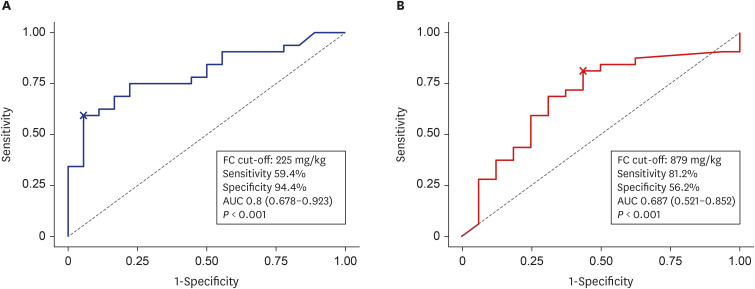 | Fig. 3ROC curve analysis for the discrimination between colorectal polyp and other major etiologies. (A) ROC curve analysis for the discrimination between colorectal polyp and anal fissure. (B) ROC curve analysis for the discrimination between colorectal polyp and ulcerative colitis.FC = fecal calprotectin, AUC = area under the curve; ROC = receiver operating characteristic.
|
Go to :
DISCUSSION
This is the first multicenter study to evaluate the value of FC in assessing colorectal polyps detected by colonoscopy among children presenting with isolated hematochezia. A significant difference in FC levels was observed between patients with colorectal polyps and other major etiologies, such as anal fissures, and UC. Furthermore, we were able to identify FC cut-off levels for discriminating between colorectal polyps and anal fissures and colorectal polyps and UC.
In our study, the most common cause of isolated hematochezia was colorectal polyps (27.6%), which are in line with previous studies of 19.5–44.1%.11113 However, unlike previous studies we were also capable of identifying a relatively high proportion of patients with anal fissures (14.2%). Although, anal fissures can be observed by inspection and a history of constipation, there are uncertain cases in which the fissures are located in the anal canal or cases of an insufficient physical exam owing to the unwillingness of the child to cooperate. Moreover, it is hard to discriminate only by history taking if the child’s history of constipation is acute or if the child does not have hardened stool. In these indefinite cases, a colonoscopy or sigmoidoscopy is required to evaluate the cause of hematochezia, and to rule out the possibility of a colorectal polyp.
FC is a neutrophil-derived substance released during cell disruption and death in the gastrointestinal tract, and is widely used as a screening test for inflammatory bowel disease (IBD), colorectal cancer, celiac disease, and necrotizing enterocolitis of newborns.1415 It is also popularly used for monitoring disease activity in patients with IBD.6716 Several previous studies have proposed the potential role of FC in identifying colorectal polyps. In a case series of 4 patients with juvenile polyps, pre-polypectomy FC levels were increased to a median 1,800 mg/kg (range, 534–2,500 mg/kg), while post-polypectomy FC levels decreased to normal in all 4 of these cases.9
In another study of 203 children who had undergone FC measurement and colonoscopy, median FC level was 844 mg/kg (range, 28–2,287 mg/kg) among 12 cases with colorectal polyps.10 That finding of elevated FC was significantly higher than the 83 cases who revealed normal findings on colonoscopy (median, 130 mg/kg; range, < 20–2,443 mg/kg; P < 0.0001). However, no significant difference was observed between the colorectal group and 108 patients with IBD (median, 962 mg/kg; range, < 20–7,780 mg/kg; P = 0.630). Meanwhile, we identified a significant difference in FC levels between patients with colorectal polyps and those with UC. This difference may be due to the larger number of patients with colorectal polyps in our study, as well as the difference in patient characteristics. We included those with isolated hematochezia, while the aforementioned study included those who had undergone a combined colonoscopy and FC, irrespective of symptoms. Meanwhile, in another prospective study in 59 children with lower gastrointestinal bleeding, FC was increased in all 26 cases with polyps (median, 685 mg/kg; range, 220–2,736 mg/kg). Furthermore, FC revealed a strong discriminative power showing a PPV of 92.8% and NPV of 100% in differentiating from the normal colonoscopy group.11
The underlying mechanism of FC elevation in colorectal polyps is yet to be elucidated. However, it is known that juvenile polyps exhibit an ulcerated surface due to auto-infarction macroscopically, while dilated cysts filled with mucin, and abundant lamina propria with prominent inflammatory infiltration are observed microscopically.17 Although there are limitations in stating whether histologically consistent characteristics exist in the different pediatric polyposis, however, depending on its unregulated growth rate, causes imbalance of blood supply, and ischemia mediates cellular injury and neutrophil recruitment. Increased calprotectin release into alimentary tract may be elucidated in this process.
Our study has some limitations and thus results should be interpretated with caution. First, this was a retrospective study and patients who did not have FC results were excluded. Therefore, selection bias may have been introduced in this process. Second, the number of patients in each group was not large. Third, we did not investigate the outcomes of post-polypectomy in our studies due to the small number of patients with such data. Fourth, differences in FC tests among centers may have affected the results. However, it has been reported that the accuracy in the FC measurement is comparable between enzyme-linked immunosorbent assay and fluorescence immunoassay.18
Future large-scaled prospective longitudinal studies may better elucidate the results of our study.
In conclusion, FC levels were capable of discriminating between colorectal polyps and other major etiologies presenting with isolated hematochezia in children. FC may assist in assessing the cause of lower gastrointestinal tract bleeding in children who present with isolated hematochezia.
Go to :
 XML Download
XML Download