

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Transforaminal epidural injection (TFEI) in the lumbosacral spine is an effective treatment for lumbar spinal stenosis, which often occurs secondary to lumbar disc pathology, degenerative conditions of the lumbar spine, and failed back surgery syndrome [1234]. Many physicians prefer TFEI to the interlaminar or caudal approach [567] because of the advantage of delivering a high concentration of medication into the ventral epidural space [8910]. The ventral epidural space is considered the main source of spinal pain [11]. However, the Adamkiewicz artery enters the spinal canal in immediate proximity to the exiting spinal nerve, typically situated ventral or slightly rostrolateral to the dorsal root ganglion/ventral ramus [12]. Therefore, there can be a risk of a vascular injection of Adamkiewicz artery when performing TFEI.
Minor complications, such as nausea, vomiting, numbness, hematomas, vasovagal syncope, transient weakness, and urinary retention are associated with TFEI [13]. Although it is uncommon, there can be serious complications, such as arachnoiditis, epidural hematoma, epidural abscess, neurologic deficit, nerve injury, paraplegia, quadriparesis, spinal cord infarction, hypersensitivity reaction, and death [1314151617]. Some of the serious complications such as hematoma, spinal cord infarction, paraplegia, quadriparesis, and death can be related to intravascular injection or vasospasm. Therefore, the methods for decreasing the intravascular injection rate can reduce these complications after TFEI [1819].
There are several investigations regarding the intravascular injection rate between different needle types in TFEI [202122232425]. Our aim was to conduct a systematic review and meta-analysis of existing comparative studies between different needle types in lumbosacral TFEI.
Go to : 
MATERIALS AND METHODS
1. Literature search
A computer-based literature search of databases, including PubMed, MEDLINE, the Cochrane Library, EMBASE, and Web of Science from 1966 to October 2018 was conducted. Keywords used to search the literature were as follows: “Whitacre”, or “Sprotte”, or “Quincke”, or “short bevel”, or “long bevel”, or “blunt tip needle”, or “catheter extension needle”. or “intravascular injection”, and “transforaminal”, or “epidural.” The reference lists of articles obtained were searched manually for additional relevant articles. We focused on randomized trials and observational studies. Abstracts were reviewed and their eligibility for the meta-analysis was determined.
2. Inclusion criteria and study selection
We enrolled randomized controlled trials and observational studies on the transforaminal epidural injection and intravascular injection rate of the Quincke and other needles. Studies about the transforaminal epidural injection that did not describe the contents of the intravascular injection were excluded. Further, case reports and case series were also excluded. An initial eligibility screening of all the retrieved titles and abstracts was conducted, and randomized controlled trials and observational studies related to the comparison of the intravascular injection rate of needles and needle types in TFEI were selected. Each study was reviewed by two authors for the stated criteria, and any disagreements were resolved with discussion.
3. Data extraction
Characteristics of each study were extracted, including the last name of the first author, publication year, study design, number of intravascular injections in the different needle groups, total number of patients, probability value, and sites that underwent TFEI (Table 1).
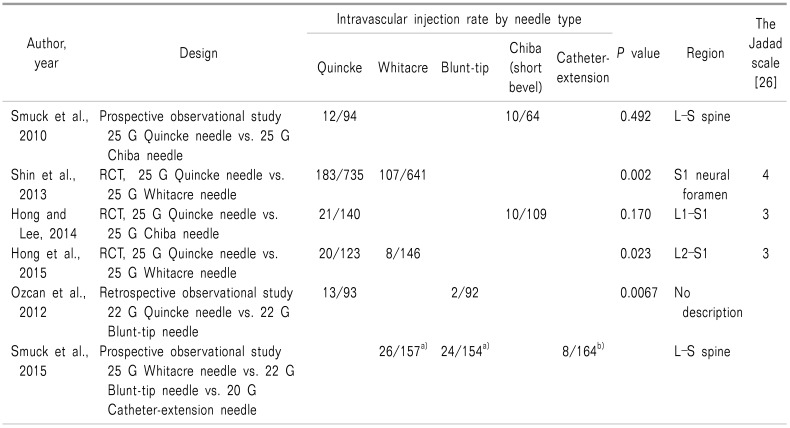
Table 1
Summary of the Studies on Transforaminal Epidural Injection
Small letter of Smuck et al. [23]'s investigation (2015): the same letters indicate non-significant difference between groups based on multiple comparison tests.
![]()
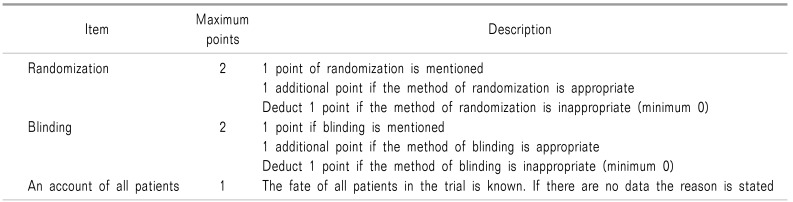
4. Quality assessment
The quality and clinical relevance were assessed using the Jadad scale [26], known as the Oxford quality scoring system, which consists of 5 questions (randomization, blinding, and an account of all patients) to assess the quality of randomized controlled trials. The range of overall scores is 0 to 5 (Table 2).
5. Statistical analysis
A meta-analysis was performed by calculating the standardized mean differences and 95% confidence intervals to evaluate the effect of the needle type on intravascular injection in TFEI. The data were analyzed using the Comprehensive Meta-Analysis version 2 to calculate the odds ratio (95% confidence interval) for each study on the intravascular injection rate of each needle type.
Go to :
RESULTS
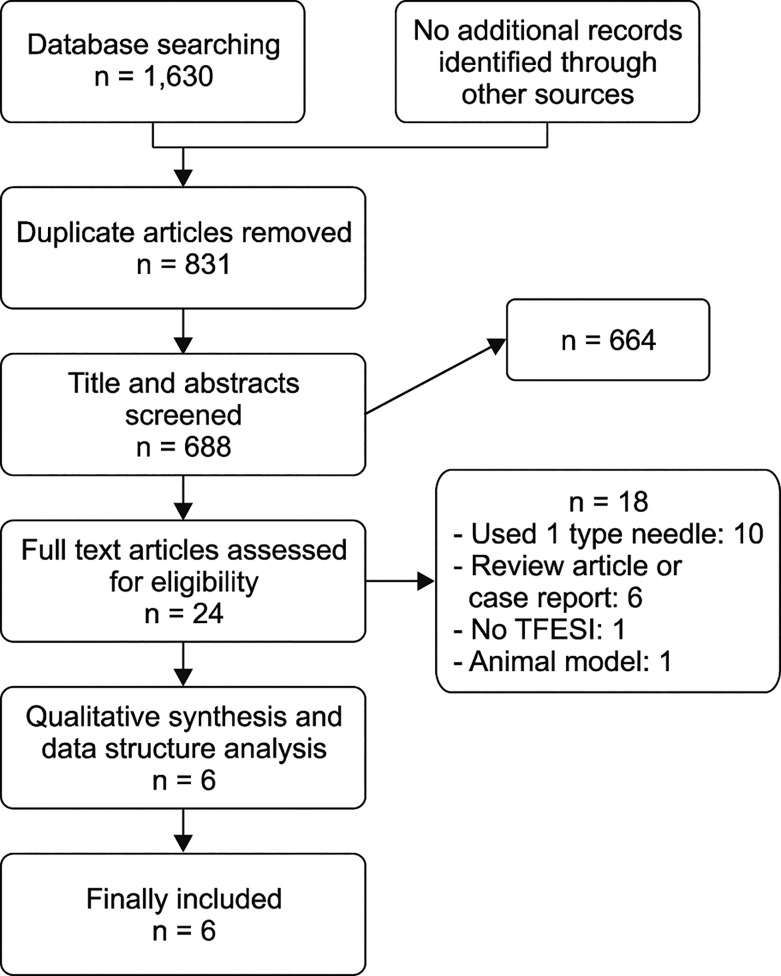
The initial search identified 335 articles in PubMed, 402 in EMBASE, 384 in Web of Science, 335 in MEDLINE complete, and 174 in the Cochrane Library. After the screening of the articles, 25 articles were identified to be associated with intravascular injection, and excluding those related to only one needle type, without transforaminal approach, animal models, review articles, and case reports, three randomized controlled trials and three observational studies were identified for analysis [202122232425]. Fig. 1 shows a flow diagram of the study selection as recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [27]. All six studies performed epidural injection using the transforaminal approach [202122232425]. Four of the six studies reported data at the lumbosacral level [21232425], and one reported data at the S1 level [22]. In another study, there was no description of the injection level [20]. They checked the transient weakness of the lower extremity; therefore, the spine level was assumed as the lumbar or lumbosacral area (Table 1).
Methodological quality assessment was carried out for three randomized controlled trials, and all of them scored 3–4 points. Two articles compared the Quincke and Whitacre needles [2225]. Two others compared the Quincke and Chiba (short bevel) needles [2124]. One article compared the blunt-tip and sharp needles [20]. Even though there was no description in the methods regarding the type of the sharp needle, the discussion revealed that it was a Quincke needle. Another article compared the blunt-tip, Whitacre, and catheter-extension needles [23].
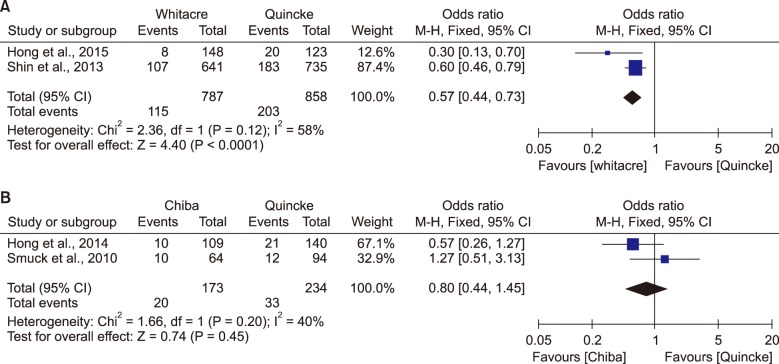
All studies comprising 2,359 patients were identified. In the subgroup analysis, 115 intravascular injections out of 787 injections were detected in the Whitacre needle, while 203 intravascular injections out of 858 injections were detected in the Quincke needle. The Whitacre needle could significantly reduce the intravascular injection rate compared w ith the Quincke needle (OR = 0.57; 95% CI, 0.44–0.73; P < 0.001) (Fig. 2). In comparing the Chiba and Quincke needles, 21 intravascular injections out of 173 injections were detected in the Chiba needle, while 23 intravascular injections out of 156 injections were detected in the Quincke needle. As a result, the intravascular injection rate of the Chiba needle has no significant difference from that of the Quincke needle (OR = 0.80; 95% CI, 0.44–1.45; P = 0.46) (Fig. 2).
In another study, 2 intravascular injections of the total 92 injections were detected with the blunt-tip needle, while 13 intravascular injections of the total 93 injections were detected with the sharp needle. Compared with the sharp needle, the blunt-tip needle could reduce the intravascular injection rate (P = 0.0067) (Table 1).
Smuck et al. [23] investigated the pencil-point (25-G Whitacre) needle, blunt-tip needle, and catheter-extension needle in TFEI, and the catheter extension needle showed the lowest incidence of inadvertent vascular uptake [23]. The incidence of vascular injections was 26/157 in the pencil-point group (16.6 ± 5.81%), 24/154 in the blunt-tip group (15.6 ± 5.73%), and 8/164 in the catheter extension group (4.9 ± 3.3%). The Whitacre and the blunt-tip needles have similar intravascular injection rates. Compared with these two types of needles, the catheter- extension needle could reduce the intravascular injection rate.
Go to :
DISCUSSION
This meta-analysis shows that the Whitacre needle can reduce the intravascular injection rate compared with the Quincke needle (OR = 0.57, 95% CI, 0.44–0.73); however, the Chiba (short bevel) needle cannot decrease the intravascular injection rate compared with the Quincke (long bevel) needle in TFEI. It was also noted that the fascicular nerve injury frequency was lower with a 45° beveled needle than that with a 14° beveled needle [28]. In our meta-analysis, no statistically significant difference was observed in the intravascular injection rates between the Chiba needle (35° bevel angle) and Quincke needle (20° bevel angle), in TFEI. Similarly, there was no statistical difference on the intravascular injection rate between the Whitacre and the blunt-tip needles; however, it was found that the intravascular injection rate was lower with the catheter-extension needle than that with the Whitacre and the blunt- tip needles.
The Whitacre needle has a pencil-point, non-cutting tip, designed to separate the tissue planes, and causes fewer post-lumbar puncture headaches in comparison with the sharp and long-beveled Quincke needles in dural puncture [2930]. It is thought that the Whitacre needle can separate the vessels and surrounding tissues; therefore, it may reduce vessel puncture and decrease the intravascular injection rate. The pencil-point tip of the Whitacre needle may slide through the vessel without damage, and the side hole of the pencil-point tip may reduce intravascular injection in spite of the tip positioned in the vessel [22]. However, the Whitacre needle has some demerits. Due to the absence of a sharp tip, it had lower steering ability than the Quincke needle [22], and skin puncture was more difficult than with the Quincke needle [22]; therefore, it may increase the total procedure time and amount of radiation exposure during the procedure.
There are some needles developed to prevent intravascular or intraneural injection. The blunt-tip needles produce less nerve damage and appear less likely to enter the blood vessels, and produce less bleeding than the sharp-beveled needles in animal studies [31]. Akins et al. [31] reported that an 18-G blunt-tip needle was less likely than a sharp needle to unintentionally enter the blood vessels. Heavner et al. [32] reported that when they tried to directly puncture the renal artery, using an 18-G, 20-G, 22-G, or 25-G blunt-tip and sharp needle, intravascular puncture was observed in more cases using the sharp needle (3 out of 5) than those using the blunt-tip needle (0 out of 8).
We could not identify any report about direct puncture of the artery using the Whitacre needle. The pencil-point tip of the Whitacre needle is not sharper than the Quincke needle, and this can be related to the lower intravascular injection rate. Kloth et al. [33] investigated the catheter extension needle, which was designed to minimize the vascular trespass risk, and the Quincke needle during TFEI; the catheter extension needle decreased the intravascular trespass rate in comparison with the Quincke needle (19/180 [10.6%] vs. 62/231 [26.8%]).
TFEI can carry a risk of intravascular injection. Kim et al. [34] investigated vascular injections and simultaneous vascular and perineural injections. According to the results, intravascular spreading patterns were observed in 45 of the 71 cervical TFEIs (63.4%) and 11 of the 111 lumbar TFEIs (9.9%) [34]. Furman et al. [35] reported that in 504 cervical TFEIs performed, the overall rate of fluoroscopically confirmed intravascular contrast injections was 19.4%, and in 761 lumbosacral TFEIs performed, the overall rate of intravascular injections was 11.2% (S1 level = 21.3%, lumbar level = 8.1%) [36]. El Abd et al. [37] reported that out of 222 TFEIs, 41 intravascular injections were observed at the cervical levels (18.47%), 113 at the lumbar levels (50.9%), and 68 at the sacral levels (30.36%). According to these results, the intravascular injection rate in the cervical and sacral spine is higher than that of the lumbar spine. Therefore, the methods that can decrease intravascular injection, such as the use of a Whitacre needle, may be a good option for cervical and sacral procedures.
To reduce intravascular injection during TFEI, physicians found other methods, such as, the use of digital subtraction angiography, catheter extension needle or blunt-tip needle, computed tomography (CT)-guided needle injection (Wolter et al. [38] performed CT-guided TFEI with dorsal access and concluded that the technique minimizes the danger of inadvertent puncture of the nerve root artery because the target point of the needle tip lies posterior to the course of the radicular artery), and specific needle tip position (Desai et al. [39] compared the superior posterior approach and superior anterior approach when performing TFEI and concluded that the former had the advantage of avoiding the radicular arteries).
Digital subtraction angiography can more precisely detect intravascular injection [4041]. Visnjevac et al. [42] reported in their meta-analysis that digital subtraction angiography detected an additional 40 events missed by real-time fluoroscopy, which detected 148 events out of 1,290 cases of TFEI (OR = 1.32 [1.05–1.67]; P = 0.02). However, digital subtraction angiography is not a basic option of mobile C-arm fluoroscopy and cannot detect all vascular injections [43]. In addition, it can increase the cost of operation and radiation exposure [44].
Some methods can reduce intravascular injection during TFEI. For example, Kim et al. reported that the overall incidence of intravascular injection during S1 TFEI in the postero-anterior approach using an anteroposterior view (29% [29/99]) demonstrated a significantly higher intravascular injection rate than that in the oblique approach using an oblique view (11%, 11/102, P = 0.001) [45]. However, they concluded that S1 TFEI, by use of an oblique view, could reduce the puncture risk to the posterior longitudinal vein. When the needle comes in contact with the bone during TFEI, the vascular injection rate increases. Therefore, in order to reduce the intravascular injection rate, avoiding contact of the needle with the bone is helpful during TFEI.
There are some limitations in this meta-analysis. There were only six articles related to intravascular injection using different needle types in TFEI. In addition, there were only two investigations comparing the Quincke and Whitacre needle, as well as the Quincke and Chiba needle. We could not find studies on the cervical or thoracic TFEI. It is thought that further investigations regarding the lumbar and other spinal TFEIs will be needed.
In conclusion, this study does not demonstrate a decrease in the intravascular injection rate with the Chiba needle as compared to the Quincke needle; however, the Whitacre needle and the blunt-tip needle can reduce the intravascular injection rate compared with the Quincke needle in TFEI. In addition, there is no difference in the intravascular injection rate between the Whitacre needle and that of the blunt-tip needle, whereas, that of the catheter-extension needle is lower than that of the Whitacre and the blunt-tip needles in TFEI.
Go to :
 XML Download
XML Download