

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
An individual's pain experience is multidimensional and dynamic, comprising psychological, cognitive, physiological and behavioral determinants [1]. Among these, personality is one of the most extensively investigated psychological constructs [2345].
Previous research has suggested that baseline personality traits significantly contribute to pain heterogeneity, as well as pain-related characteristics [678]. In general, neuroticism, has often been linked with negative health outcomes [91011].
Neuroticism was a significant predictor of fibromyalgia symptoms along with factors associated with the hypothalamic-pituitary-adrenal axis in a study that compared 22 fibromyalgia patients to 17 controls [12].
Affleck et al. [13] showed that rheumatoid arthritis patients who reported higher in neuroticism reported more intense pain and a more negative mood, their daily mood was less strongly linked to their daily pain.
The most robust finding was a significant phenotypic association between cold pressor pain intensity and the personality facets Impulsiveness (a facet of Neuroticism) and Excitement-Seeking (a facet of Extraversion), and estimates of the genetic correlation were 0.37 (P < 0.05) and 0.43 (P < 0.05), respectively [14].
Neuroticism is nowadays considered to be a broad construct and some pain-related cognitive and behavioral characteristics, including pain catastrophizing, are shown to be associated to it [1516]. Furthermore, catastrophizing has been shown to mediate the relationship between negative affect (neuroticism), somatic complaints, and functional disability [1718] and its consistent association with pain has been observed across a variety of measures and patient groups, where it accounts for 7 to 31% of the variance in pain ratings [19].
The association of the remaining two dimensions of EPQ to pain, extraversion and psychoticism, are less consistent. It has been shown that participants who scored higher on the extraversion scale tolerated pain longer [14]. A study by Harkins explored the associations of neuroticism and extraversion with experimental thermal pain (43-51C stimuli) and clinical pain in patients with myofascial pain dysfunction. Extroverts didn't differ from introverts in visual analogue scale pain ratings from thermal pain nor VAS ratings of their clinical pain. Psychoticism, as the third segment of Eysencks' personality model which consists of a combination of obsessive, compulsive and paranoid sub-traits was only occasionally found to influence chronic pain treatment outcomes [20].
Lee et al. [21] 2010 demonstrated the results of a regression analysis which showed that lower-order pain constructs (fear, catastrophizing, and hypochondriasis) are correlated through a single underlying factor that is partially related to the higher-order negative-valence personality traits; 2) pain-was more strongly predictive of pain quality than higher order traits (e.g. neuroticism); and 3) qualitative pain ratings rather than quantitative ones were significantly predicted by psychological factors.
Even though there are numerous studies exploring the association between personality traits and chronic pain conditions [22232425], it is often difficult to determine whether an individual's personality characteristics contribute to how they perceive and experience pain or, conversely, whether it is their pain condition that has affected their personality. Accordingly, the current study examined the above constructs in two ostensibly healthy participant samples, using standardized measurements for both pain and personality constructs.
Participants were derived from an island and a mainland setting in the Croatian region, respectively, whereas previous studies have suggested high levels of social, environmental and genetic homogeneity [262728]. The current study aimed to examine the relationship between higher-order personality traits (neuroticism, extraversion, psychoticism) and pain catastrophizing as well as their relation to experimentally-induced pressure pain, by testing whether pain catastrophizing mediates the relationship between neuroticism and pain. These relationships would be explored on the level of a complete sample as well as island (Korcula) and mainland (Split) subsamples. We hypothesized that neuroticism and psychoticism would be correlated to pain catastrophizing while extraversion would not. Based on previous research, we also hypothesized that pain catastrophizing would at least partially mediate the relationship between neuroticism/psychoticism and pain responses.
Go to : 
MATERIALS AND METHODS
1. Ethics statement
The experiment was conducted in accordance with the Helsinki Guidelines and IASP guidelines for human pain research. Approval was granted by the Ethics Committee of the School of Medicine, University of Split. All participants have provided written informed consent which was also previously approved by the ethics committee.
2. Participants and study setting
For purposes of this study, we enrolled participants from the island of Korcula and the mainland city of Split. All the participants were apparently healthy, with no noticeable severe medical conditions that could affect their health status.
A trained research assistant evaluated if they had any of the following exclusion criteria, which could preclude understanding of study procedures or participation in pain induction procedures: acute illness or injury that may impact their performance (eg. fever, flu symptoms), hand injuries, use of opioids in the previous 48 hours, prescription medication, developmental delay, or significant anatomic impairment.
3. Measures
Pressure pain threshold (PPT) is defined as the amount of force needed to elicit a sensation of pain distinct from pressure. In this study, PPT was measured using a handheld digital pressure algometer (Wagner Instruments, Greenwich, CT), mounted with a 1-cm diameter circular probe and calibrated in kilopascals (kPa). To assess the PPT, the probe was held perpendicularly on the middle phalanx of the index finger of both hands, and the pressure was applied at an approximately constant rate of 5 kPa/s. When the PPT was reached, the participant said “stop”, at which moment the algometer pressure was lifted, while the device recorded the maximum force achieved. In order to provide reliable measurement, a total of five measurements were made. The initial two measurements were done to familiarize the participants with the process. After at least 30 minutes, the PPT was measured again, three times at the same spot. Finally, we calculated mean value for all three measurements to obtain mean PPT.
The pressure pain tolerance (PPTOL) was measured in the similar way as the PPT, but this time the participants were asked to tolerate the pain for as long as it seemed reasonable. We also set a cut-off value at 130 kPa in order to avoid tissue damage in participants who still did not stop the pressure application. Two consecutive measurements were done, and their mean value was used as the PPTOL, for each hand separately. Participants were then involved in the pain pressure test in the following order: PPT and then PPTOL. The same team of experimenters conducted all procedures, with a female researcher who performed all of the pain pressure tolerance and threshold measurements for participants.
The Eysenck Personality Questionnaire-Revised (EPQ-R) was used to provide estimates in four sub-scales: psychoticism, extraversion, neuroticism, and social desirability (applied only as a control scale and not analyzed in this study). Higher scores on the neuroticism scale (EPQ-N) indicate an anxious, worrisome, overly emotional, and somewhat rigid personality. A higher score on the extraversion scale (EPQ-E) indicates a sociable, optimistic, excitement-craving, easy-going personality. Higher scores on the psychoticism scale (EPQ-P) indicate a disinhibited, hostile, and non-conformist personality. EPQ-R has been demonstrated to have good internal consistency and test-retest reliability [29]. In this study we used a short form of the EPQ-R with 48 items, containing 12 items for each of the subscales. The Croatian version of this questionnaire has been validated and extensively used [30].
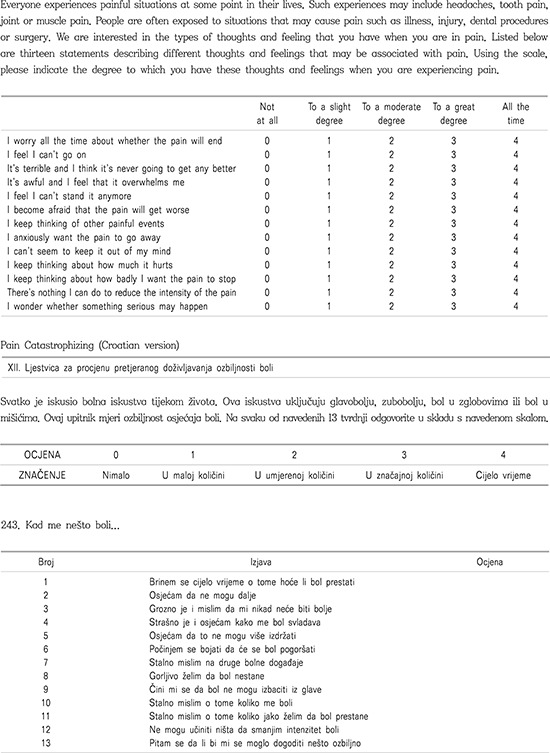
The Pain Catastrophizing Scale (PCS) was used as a measure of catastrophic thinking associated with pain [31]. The PCS instructions require a participant to reflect on past painful experiences, and to indicate the degree to which they experienced each of 13 thoughts or feelings when experiencing pain, on 5-point scales with the end points (0) not at all and (4) all the time. The PCS yields a total score and three subscale scores assessing rumination, magnification, and helplessness. The validated Croatian version of the PCS was used. PCS measurements in this study were shown to have very high internal consistencies (Cronbach coefficient αs: total PCS = 0.94, rumination = 0.89, magnification = 0.80, and helplessness = 0.88).
4. Statistics
Descriptive statistics were calculated for each study variable, including distinctive analysis for the two cohorts (Korcula and Split), as well as the gender differences. Variance homogeneity analysis would be conducted first which would determine how the further statistical analysis would proceed (entire sample analysis or separate analysis for each cohort).
To determine if sample distributions were approximately normal, the Kolmogorov-Smirnov test was used. The General Linear Model (GLM), including the factors of Group and Sex on the EPQ personality and pain ratings, with the age as the covariate was used to explore the differences between the island and mainland cohorts.
Univariate comparisons for sociodemographic characteristics were performed using appropriate tests (the t-test or Chi square test). Associations of the pain and psychological variables were assessed using Pearson's correlation coefficients. In addition, a regression analysis was used to test mediation models of pain catastrophizing, EPQ traits, and outcomes in perceived pain (pain tolerance/threshold) using the criteria outlined by Baron and Kenny [32] are: (1) (neuroticism) must be significantly associated with (the pain threshold and pain tolerance); (2) (neuroticism) must be significantly associated with the mediator (catastrophizing); (3) the mediator (catastrophizing) must be significantly associated with (the pain tolerance and pain threshold) after controlling for the (neuroticism); and (4) the strength of the relationship between (the neuroticism) and (the pain threshold and pain tolerance) must be significantly reduced after controlling for the mediator (pain catastrophizing scale, Appendix 1).
All analyses were conducted using IBM SPSS for Windows Version 17 (SPSS Inc., Chicago, IL). The significance of indirect paths was computed by Process (SPSS macro) [33]. Significance was set at the level of P < 0.05.
Go to :
RESULTS
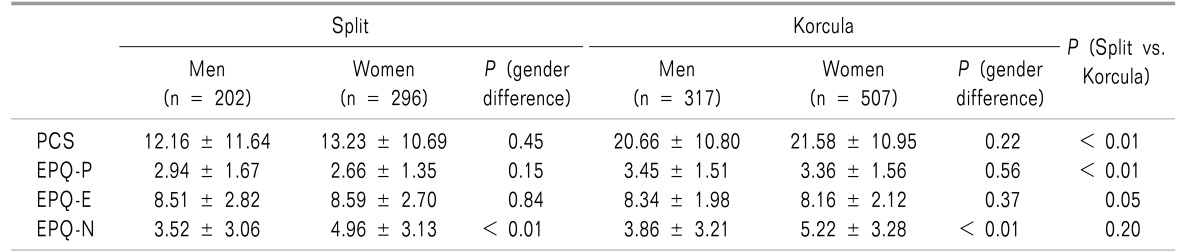
A total of 1,322 participants were enrolled in this study, with 824 from Korcula and 498 participants from Split (Table 1). Personality trait scores slightly differed between the Split and Korcula cohorts, so we presented the EPQ and pain reports separately. The initial comparison suggested that the cohorts differed in age which was then added as a covariate in further analysis. The Korcula cohort had significantly higher values of psychoticism, and marginally lower mean values of extraversion and neuroticism, compared to Split cohort (Table 1). Pain catastrophizing scores were significantly higher for the Korcula cohort compared to the Split cohort.
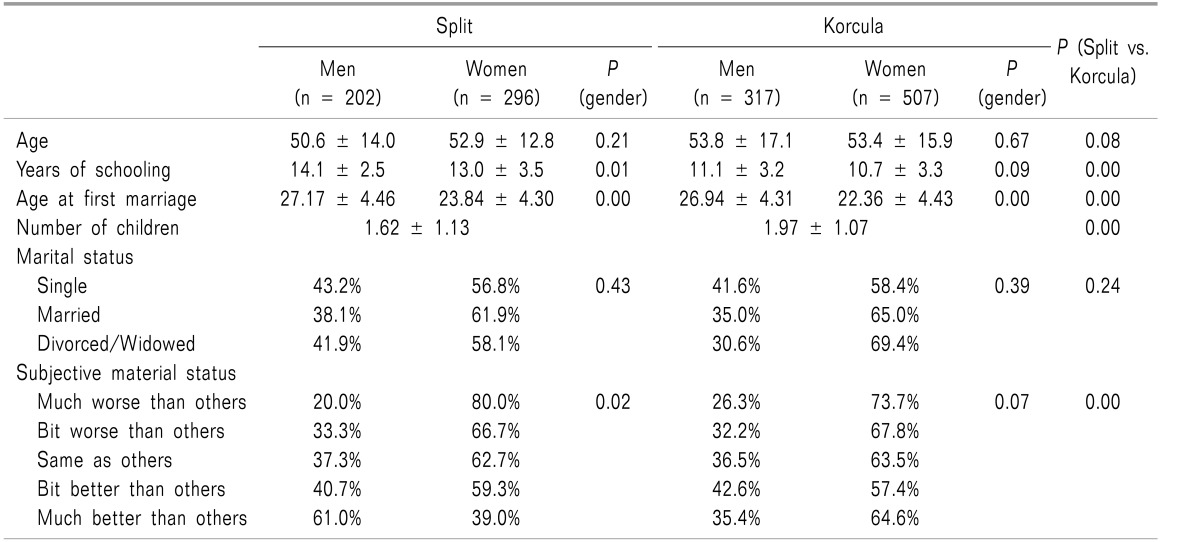
Furthermore, a cohort-based analysis suggested that in both instances women had higher neuroticism scores, did not differ on the extraversion scale, while in terms of psychoticism the results suggested either significant difference in Split or marginally insignificant difference in Korcula (Table 2).
Neuroticism was the only personality trait that indicated gender differences, as women showed significantly higher results (F = 26.24, P < 0.001) when controlled for age; however, no differences were found between the two cohorts. The island cohort showed increased pain catastrophizing scores (F = 51.50, P < 0.001) and increased psychoticism (F = 28.23, P < 0.001). No significant interaction effect was found between the cohort and the gender of the person for any of the personality constructs (lowest P = 0.301).
The association between neuroticism and pain threshold was mediated by pain catastrophizing (Fig. 1), the same pattern being found in both cohorts (Korcula and Split). The standardized regression coefficient between pain threshold and neuroticism decreased when controlling for pain catastrophizing. The other conditions of mediation were also met: neuroticism was a significant predictor in pain perception and pain catastrophizing, while pain catastrophizing was a significant predictor in pain perception, while controlling for neuroticism (Fig. 1).
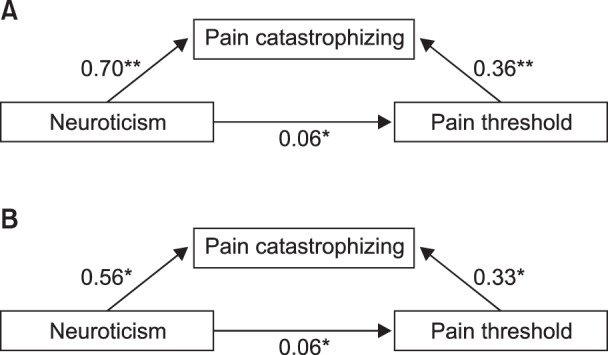 | Fig. 1Standardized regression coefficients for the relationship between neuroticism and pain threshold, mediated by pain catastrophizing, A (Korcula), B (Split). The standardized regression coefficient between neuroticism and pain threshold controlling for pain catastrophizing is in parentheses. *Denotes significance at the level of P < 0.05, while **Denote significance level of P < 0.001.
|
The comparison of PPT and PPTOL measures for both hands, adjusted for age, suggested that cohorts significantly differed in their response to pain (Table 3). PPT was higher for the mainland cohort (F = 102.32, P < 0.0011), similarly to PPTOL, (F = 9.52, P = 0.002). Gender differences were observed across all measures in both cohorts, where men consistently reported higher thresholds (F = 49.88, P < 0.001) as well as higher tolerance (F = 90.38, P < 0.001), even after adjustment for age.

There was no significant interaction effect between the cohort and the gender of the person on pain tolerance measures (P > 0.05). This indicates that affiliation to either cohort affected pain tolerance measurement of both genders in the same way.
Correlations between pain threshold and tolerances were significant for all pairs at the level of P < 0.001 (Table 4).

Contrary to our expectations, the higher-order, negative valence traits (neuroticism and psychoticism) were not correlated with each other (Table 4). Psychoticism was not correlated with any of the traits (Table 4). Extraversion was negatively correlated with negative valence traits. The lower order construct, pain catastrophizing, had the highest correlation with neuroticism and was significantly correlated with other higher order traits (Table 4).
Go to :
DISCUSSION
The results of this study show a strong association of neuroticism with pain catastrophizing, and a partial mediation effect of pain catastrophizing in the association between pain and neuroticism. The remaining two personality constructs were not consistently related to pain (either pain tolerance or pain threshold). Although pain catastrophizing was significantly associated to all measured personality traits in bivariate analysis, only marginal associations were found with the pain reports.
Neuroticism as a higher order personality trait proved to be directly associated with pain reports and pain catastrophizing (a lower order personality trait) served as a partial mediator to this association, contrary to the recent literature [3435363738].
Our results support the idea that neuroticism could be perceived as a vulnerability factor within a diathesis-stress framework [15]. When a person is faced with a stressor, such as (acute) pain, neuroticism may influence whether the person appraises the pain as threatening or not [363940]. No direct effect of catastrophizing could also be a consequence of contextual factors such as the threat value of pain, which may differ in laboratory settings versus clinical environments.
Some studies have suggested that measuring pain catastrophizing in an experimental setting could be seen as more valid if taken after noxious stimulation [41]. Post-noxious assessment of catastrophizing refers to a participant's actual behavior in response to an immediate and relevant pain situation. This finding is directly applicable to the clinicians' assessment of catastrophizing in the chronic pain patient [39].
In addition, neuroticism may even reduce the threshold at which pain is perceived as threatening, and at which pain elicits catastrophic thoughts. These results support a dynamic view of personality where behaviors are modified according to the context. Extraversion and psychoticism explored in our study did not seem to play a role in pain perception. We found no evidence that participants who scored higher on the extraversion scale were able to tolerate more pain compared to introverts as is suggested in the literature [42].
Pain catastrophizing, as assessed in this study, did not have any direct association to pain tolerance, contrary to the growing body of literature that suggests pain catastrophizing to be a stable mode of responding to painful experiences [434445]. No cohort-related or gender-related differences were statistically significant, even though women and the island cohort had elevated results on the PCS.
Neuroticism is also characterized by emotional instability, sensitivity, and dependency which may serve as predisposition for pain stimulus appraisal or threat of a potential pain stimulus [46]. Also neuroticism was the only psychological variable that differentiated between men and women. In general, women tend to score higher on neuroticism [4647], whereas gender differences in other Eysenck personality traits have been either inconsistent or of negligible magnitude.
The described gender differences seem to be consistent across different ages in the life span [48]. Several authors have indicated that gender differences in personality are modest in magnitude but consistent with gender stereotypes, and replicable cross-culturally [14]. A systematic review published in 2012, which examined gender differences in experimentally induced pain, showed that women and men have comparable thresholds for cold and ischemic pain, while pressure pain thresholds were lower in women compared to men [49]. They indicated that women tolerate less thermal (heat, cold) and pressure pain than men. The majority of the studies that measured pain intensity and unpleasantness showed no sex difference in many pain modalities [505152]. A considerable body of experimental research showed a lack of consistency related to gender differences in human pain sensitivity, even with the use of deep, tonic, long-lasting stimuli, which are known to better mimic clinical pain [53].
Island-mainland differences were evident in both the pressure pain threshold and pressure pain tolerance measures. Also, pain catastrophizing and psychoticism seem to be the only personality traits which produced a consistent difference between these two cohorts. The study of isolated populations is advantageous because of its increased genetic and environmental homogeneity compared with urban populations [27]. Even though studying island populations facilitates gene mapping, it has the disadvantage of reducing the diversity of genetic effects and increasing the extent of shared environmental effects [26].
The limitations of this study include selection bias (the inability to properly address the sample representativeness for the cohort they are representing) and the facts that all pain ratings were performed by a female research assistant, which could have potentially affected the results (pain reports) of men. Furthermore, some results were shown to be inconsistent with previously published studies, thus suggesting that replication of the results is needed before more general conclusions can be drawn. Nevertheless, these findings could have important practical implications, as certain factors assessed a priori (e.g. preoperatively) may have predictive value for those who will perceive greater pain using qualitative assessments.
A better understanding of the structure defined by potential pain-related psychological variables and their influence on the perception of acute pain may assist in the development of future treatment. Individualized multidisciplinary therapeutic interventions may be plausible to better meet the needs of patients for a variety of acute pain conditions.
Go to :
 XML Download
XML Download