

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Herpes zoster is an infectious disease caused by the reactivation of the varicella zoster virus. The virus usually lies dormant in the sensory ganglia of the cranial and spinal nerves following the resolution of chicken pox [1], but it can be reactivated in patients with decreased cell-mediated immunity due to advanced age or immunosuppressive medical conditions and malignancies [2]. Individuals affected by the reactivated herpes zoster develop characteristic dermatomally distributed vesicular skin lesions that usually heal within 2-3 weeks. Pain which often precedes or accompanies the herpes zoster rash is one of the most common and debilitating complications [3]. Although there is no unified or defined duration of pain, most clinicians define postherpetic neuralgia (PHN) as pain that lasts > 90 days from the onset of the skin rash [456].
PHN incidence varies from 5 percent to more than 50 percent depending on the study design, age distribution of the enrolled patients, and PHN definitions [57]. Although the intensity of postherpetic pain typically decreases over time, pain lasts more than 1 year in more than 30% of patients [5]. Pain severity ranges from mild to excruciating. In some individuals, intractable chronic pain can lead to depression, fatigue, and sleep disturbance [89]. The socioeconomic consequences secondary to prolonged severe pain include decreased socialization, daily activities, and quality of life [10]. Therefore, when treating patients with acute herpes zoster, it is important to prevent PHN at the same time in order to control acute viral infection and associated pain. Because of the complexity of the underlying pathophysiological mechanisms that contribute to the development of postherpetic neuralgia, various strategies for preventing PHN including corticosteroids, antidepressants and anticonvulsants, antiviral agents and vaccination have been proposed [610111213]. However, according to a recently published systematic review and meta-analysis, the effectiveness of these strategies toward preventing PHN is insufficient except among a limited and well-selected population (e.g., administering vaccines to adult ≥ 60 years) [71415].
Applying sympathetic and somatic neural blocks via local anesthetics and/or corticosteroids has also been applied to control pain during the acute phase of herpes zoster and PHN, as well as reduce PHN incidence [1617]. The rationale for applying neural blocks to treat herpes zoster is to attenuate central sensitization by interrupting the transmission of nociceptive afferent impulses to the central nervous system and minimize nerve damage by improving blood flow to the nervous tissue during deafferentation. Additionally, the anti-inflammatory effects of local anesthetics and corticosteroids within the territory of the affected nerve may play a role [18]. Some retrospective and observational studies fail to demonstrate the effectiveness of applying early neural blocks to prevent PHN [19] and only report short-term relief from acute pain [20]. Even though there is weak evidence that neural blocks can prevent PHN during the early phases of herpes zoster, several other studies suggest significant benefits [2122].
This study investigated the efficacy of using neural blocks to prevent the development of PHN in patients with acute herpes zoster. We compared between-group differences in PHN incidence, as published in randomized controlled trials in which the enrolled patients received either standard therapy or standard therapy with additional nerve blocks.
Go to : 
MATERIALS AND METHODS
We searched several comprehensive databases in order to find published studies on applying neural blocks during the acute phase of herpes zoster to prevent PHN. This systematic review was designed according to the Cochrane Review Methods [23]. We report our findings in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [24].
1. Data and literature sources
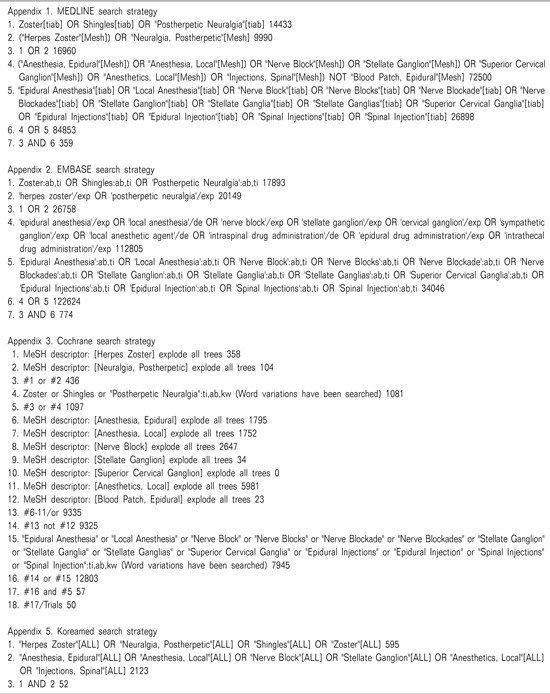
The searches for this review were performed on April 30, 2014. We searched the MEDLINE, EMBASE, Cochrane Library, ClinicalTrials.gov, and KoreaMed databases. Both published and unpublished trials were included, and no language or date restrictions were applied to our electronic searches. Full-text searches were also performed using Google. All records were searched using the following terms: herpes zoster, nerve block, epidural, dorsal root ganglion, stellate ganglion, spinal nerve, sympathetic, postherpetic neuralgia. See Appendices for the comprehensive list. Search strategies were appropriately adapted for other databases according to the MEDLINE strategy. After the initial electronic search, the references of relevant studies were searched to identify additional studies. Identified articles were individually assessed for inclusion.
2. Study selection
Potentially relevant articles were evaluated, and all data were extracted by two independent reviewers (Leem and Kim) according to the predefined selection criteria. Agreement was reached through discussion whenever differences arose. The two reviewers initially assessed the identified studies by the title and abstract. The full text of any potentially relevant articles was reviewed and assessed. Studies were included in our meta-analysis if they meet all of the four following conditions: (1) randomized controlled trials that enrolled patients with herpes zoster within 3 weeks after the onset of herpetic skin rash; (2) the treatment group received nerve blocks that consisted of local anesthetics and/or steroids in addition to standard medical therapy; (3) the control group received either nerve blocks with electrolyte solution and/or steroids or standard medical therapy without nerve blocks; and (4) outcome data were collected > 12 weeks after the final intervention.
3. Data extraction
Data extraction was independently performed by at least two reviewers using a prespecified data-extraction form. Any discrepancies that remained unresolved following discussion were reviewed by a third author. Extracted data included study name, author, country, study year, inclusion and exclusion criteria, number of participants, duration of acute herpes zoster, characteristics of the administered neural blocks (e.g., route, frequency, dosage), number of withdrawals related to intervention, outcomes, and adverse events. The primary outcome was PHN incidence at 3, 6, and 12 months after the onset of herpetic skin rash. PHN was defined (according to clinical diagnostic criteria) as persistent pain at the affected site ≥ 3 months after the onset of the acute rash [25]. Secondary outcomes included duration of pain due to acute herpes zoster, pain severity measured using a validated visual analogue scale (VAS) or numerical rating scale (NRS) at 3, 6, and 12 months, and intervention-related adverse events. If the primary outcome variables were not mentioned, we estimated these data from the figures or requested the data by directly emailing the study authors.
4. Statistical analysis
The primary outcome of our review was the effect of the nerve blocks on PHN in patients with herpes zoster. Although PHN is generally defined as pain persisting ≥ 3 months after disease onset, it may last longer or recur. Therefore, in order to assess the long-term efficacy of intervention, we also evaluated outcomes at 6 and 12 months after final intervention. Secondary outcomes included duration of pain and adverse events caused by administering the nerve blocks. PHN was measured using pooled risk ratios (RR) and 95% confidence intervals (CI), which were calculated using the Mantel-Haenszel method according to the number of events and total number of patients included in the control and intervention groups of each study. Pain intensity was calculated using the weighted mean differences, 95% CIs, and mean and standard deviation values reported in each study using random effects modeling and inverse variance methods. Because all included studies used either VAS or NRS, which have different measurement scales, we used the standard mean differences to standardize the values from each scale. For studies that presented median and range values instead of mean and standard deviation values, we interpreted the median as the mean and calculated the standard deviation from the range using the equations included in the Cochrane Methods.
Heterogeneity was estimated using I2 statistics, which measures the proportion of inconsistency between studies that arises from true differences rather than random errors or chance. I2 values of 25%, 50%, and 75% were interpreted as low, moderate, and high heterogeneity, respectively. We conducted subgroup analyses according to the type of nerve block performed on the intervention group (e.g., stellate ganglion, paravertebral, repeated/continuous epidural, single epidural blocks), frequency of administering the local anesthetics (e.g., single block, repeated/continuous block), and time after intervention (3, 6, 12 months). RevMan version 5.2 was used to perform these analyses.
Go to :
RESULTS
1. Study identification
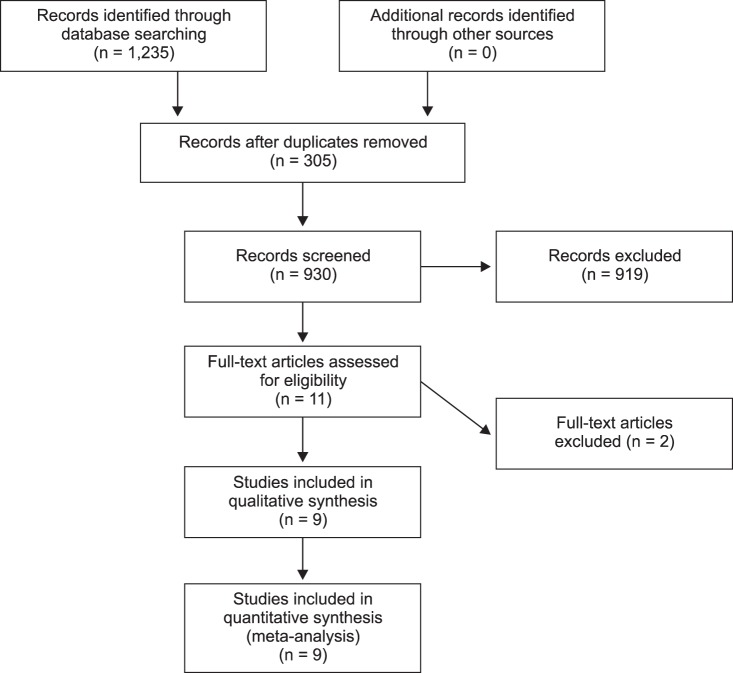
Database searches provided 930 articles (Fig. 1). Of these, 919 publications were excluded because it was clear from the title and abstract that they did not fullfil the selection criteria. We obtained the full manuscripts of the remaining 11 articles, but following additional scrutiny we only identified 9 potentially relevant studies (Fig. 1). Two publications were excluded: 1 publication did not report PHN incidence and no reply was received from the authors [26], and 1 study utilized a cross-over design that used a bupivacaine and electrolyte solution [27].
2. Study characteristics and patient populations
Table 1 summarizes the country that conducted each relevant study, inclusion/exclusion criteria, interventions, outcome measures, and results of the included studies [282930313233343536]. All included trials are randomized controlled parallel studies, except one [28]; however, we included this trial in this review because there were no differences in the demographic characteristics and the study participants were consecutively assigned. A total of 1,645 participants were enrolled in the 9 included studies. Sample sizes ranged between 20-598 patients. There were no differences in the sex ratios between the control and neural block groups mentioned in 8 trials [2829303133343536]. Six trials [293233343536] stated explicit age criteria for inclusion. Among these, 4 trials [29333436] included participants > 50 years old, 1 trial included patients > 55 years [35], and 1 trial included patients > 60 years [32]. Three trials [283031] were conducted in Korea and did not state the age criteria, but the mean age of participants was > 56 years in all 3 trials. The inclusion criteria for the duration of acute herpes zoster in 7 trials [28293233343536] were within 2 weeks after the onset of the rash, and the remaining 2 trials extended duration to up to 3 weeks [3031].
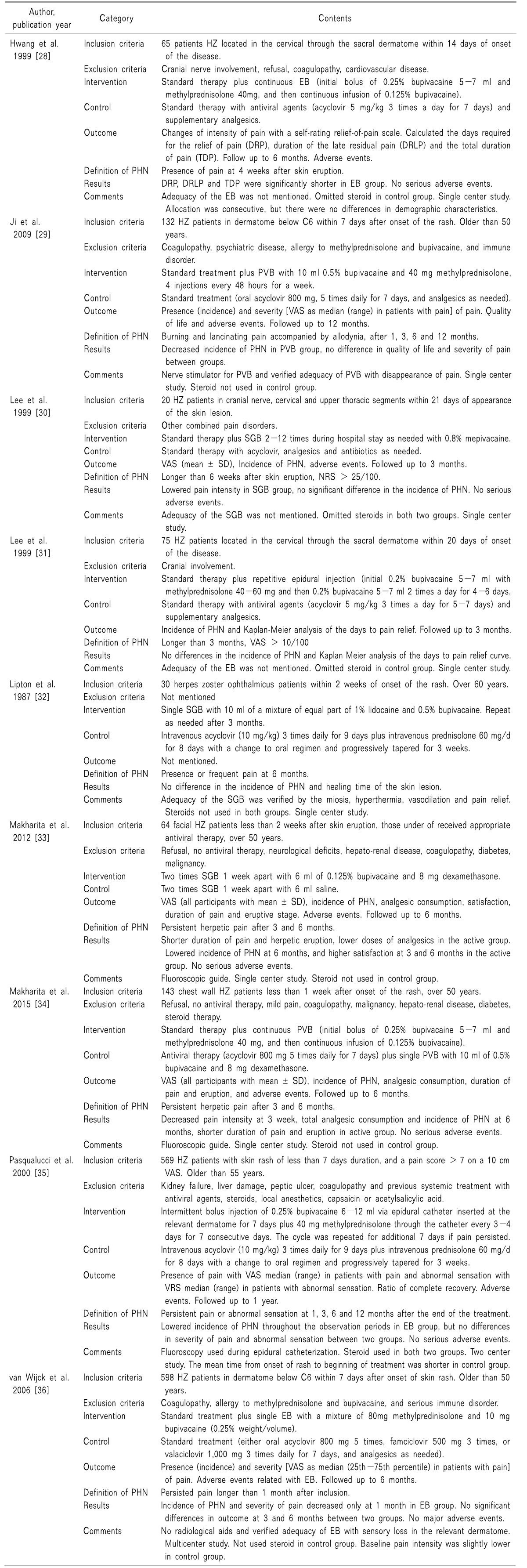
Table 1
Characteristics of Included Studies
HZ: herpes zoster, EB: epidural block, DRP: days required for the relief of pain, DRLP: duration of the late residual pain, TDP: total duration of pain, PVB: paravertebral block, VAS: visual analogue scale, PHN: postherpetic neuralgia, SGB: stellate ganglion block, NRS: numeric rating scale, VRS: verbal rating scale.
![]()
The types of administered neural blocks were determined according to the nerve affected with herpes zoster. Three trials administered stellate ganglion blocks to the facial, cervical, or upper thoracic segment [303233]; 4 trials administered epidural blocks [28313536]; and 2 trials administered paravertebral blocks to the dermatome through the cervical to sacral spinal segments [2934]. Two studies conducted by the same institution enrolled control groups that were administered electrolyte saline solution to the nerve [3334], and 7 trials enrolled control groups that only received standard medical treatment without nerve blocks [28293031323536].
Injections varied in terms of frequency, volume, type of administered local anesthetics, and steroids. Two trials only administered a single injection [3136], but multiple or continuous injections were administered in 7 studies [28293031333435]. Outcome measures differed widely between trials. All included trials reported PHN incidence, as defined as the presence of persistent pain and/or abnormal sensations relevant to the dermatome that were affected by herpes zoster. However, the duration and cutoff times for PHN pain ranged from 1 month through 1 year. Two trials stated that the pain intensity used to define PHN was VAS > 10/100 [31] or > 25/100 [30], respectively. The remaining 7 trials did not mention the pain intensity used to define PHN. In our present review, we used PHN incidence at 3 months after the onset of the rash in the meta analysis, and additionally PHN incidence at 6 and 12 months was used to assess the long-term effects.
3. Quality of the included studies
The heterogeneity between the trials included in this review is high in terms of PHN incidence. However, when the outcomes of the subgroups were assessed according to the type of nerve block (stellate ganglion block, paravertebral block, or epidural block), heterogeneity was insignificant (I2 < 30%). Despite the poor quality of some trials, the paucity of high quality randomized controlled trials made us include those trials in the meta-analyses because there were no significant differences in the outcomes that are relevant to this review.
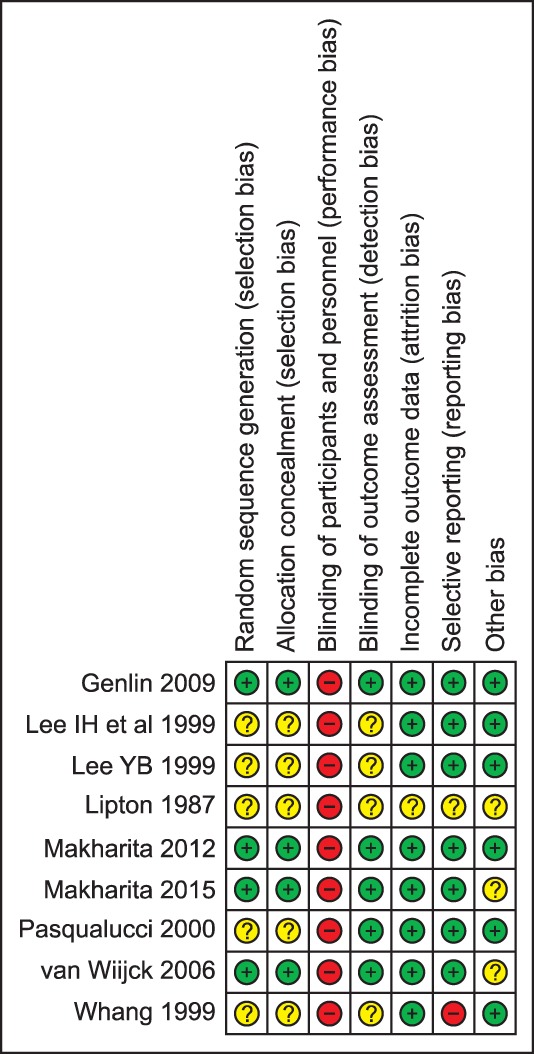
Risk of bias is summarized in Fig. 2. In 5 trials published after 2000 [2933343536373839], participants were randomly assigned using a computer-generated algorithm or computer program with block generation. Although detailed methods for allocation were not mentioned in 4 trials published before 2000 [28303132], the demographic characteristics of the control and intervention groups are similar. It is virtually impossible to study patients who receive nerve blocks in a blind manner. Procedural pain and the symptoms and signs of sensory-motor and/or sympathetic blocks may induce placebo effects. Furthermore, ethical issues make it difficult to enroll active control groups. As a result, we assessed all 9 trials included in this review as “high ” risk to the point of “blinding the participants and personnel ”. In 5 trials [2933343536], the outcomes and adverse events were assessed by researchers who were unaware of the study protocol and graded as “low ” risk for detection bias, but the other 4 trials did not present sufficient information to make a decision [28303132]. For selective reporting bias, PHN incidence was not the primary outcome in 1 trial [28], and another trial did not present any information about the 4 PHN cases in the control group [36]. The demographic characteristics of the participants were not similar between trials. Time from disease onset to the first block was not similar between groups [33], and the baseline pain intensity was slightly lower in the control group [36].
4. PHN at 3, 6, and 12 months after the Onset of the Herpes Zoster
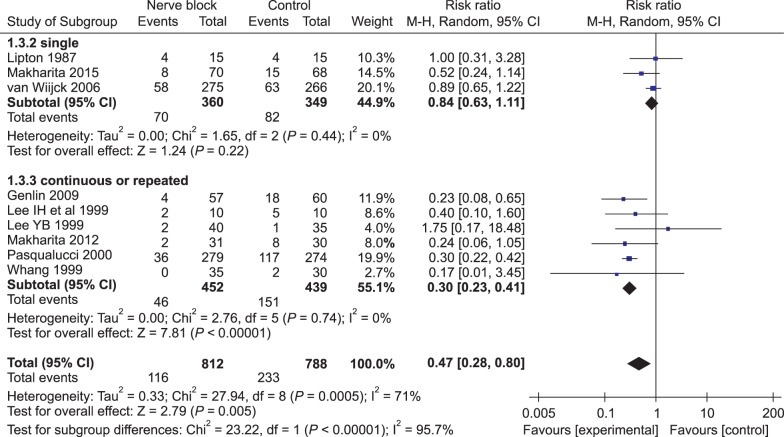
We performed a meta-analysis in order to combine the relevant data obtained by the 9 included trials. The results show that PHN incidence following nerve block application was significantly reduced in comparison with standard treatment alone at 3, 6, and 12 months after the onset of herpes zoster (RR = 0.43, CI = 0.25-0.76, P = 0.004, I2 = 74% at 3 months; RR = 0.41, CI = 0.2-0.83, P = 0.01, I2 = 77% at 6 months; RR = 0.17, CI = 0.1-0.28, P = 0.00001, I2 = 0% at 12 months) (Fig. 3). To reduce heterogeneity, we performed a subgroup analysis according to the type of nerve block administered at 3 months after herpes zoster was diagnosed. PHN incidence was not reduced by administering stellate ganglion block (RR = 0.50, CI = 0.22-1.17, P = 0.11, I2 = 17%) or a single epidural block (RR = 0.89; CI = 0.65-1.22, P = 0.47). However, PHN incidence was significantly reduced by administering continuous/ repeated epidural blocks (RR = 0.34, CI = 0.17-0.67, P = 0.002, I2 = 11%) and paravertebral blocks (RR = 0.37, CI = 0.17-0.81, P = 0.01, I2 = 32%) (Fig. 4). According to the subsequent meta-analysis of the differences between administering single or repeated/continuous blocks, PHN incidence was significantly reduced by administering repeated/continuous block (RR = 0.30, CI = 0.23-0.41, P = 0.000001, I2 = 0%) but not a single block (RR = 0.84, CI = 0.63-1.11, P = 0.22, I2 = 0%) in comparison with standard therapy alone (Fig. 5).
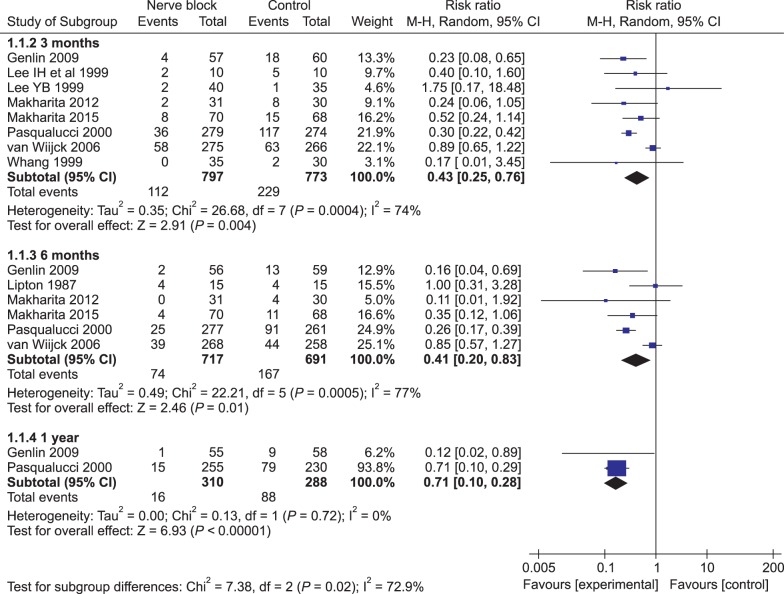 | Fig. 3Effects of nerve blocks on the incidence of postherpetic neuralgia. The incidence of postherpetic neuralgia was significantly lowered in nerve block treatment compared with control standard treatment at 3, 6 and 12 months after the onset of herpetic skin rash, but heterogeneity among trials was high.
|

5. Secondary outcome measures
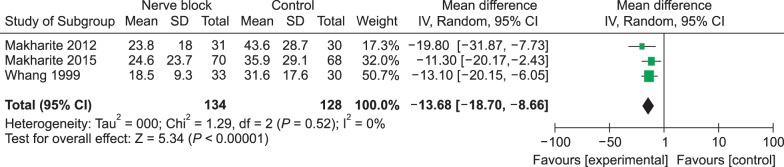
Most of the studies included in this review used VAS or NRS to measure intensity and/or changes in pain. One study used a self-rating relief-of-pain scale, where pain intensity was defined as 100 at the time of admission (or worst pain) and no pain was defined as 0 [28]. Three trials reported the duration of pain as measured by the complete resolution of herpetic pain and/or days required for pain intensity to decrease from 100 to 0 [283334]. The meta analysis of these 3 trials indicated that pain duration after administering nerve blocks was significantly shorter than after standard therapy (pain duration with days, mean difference = −13.68, CI = −18.70 - −8.66, P < 0.00001, I2 = 0%) (Fig. 6).
Eight trials [2829303133343536] included in this review reported the pain intensity from baseline through the end of the study, but 4 trials did not [28313235]. To report the pain intensity during the observation periods, 3 trials used the mean and standard deviation values of all participants [293334], but 3 trials described pain as the median (range) or median values (25-75 percentile) of only the patients with pain [293536]. Two trials [2831] reported pain duration, and 1 trial [32] reported the individual VAS scores of 4 PHN cases. Therefore, we did not combine these data in this meta-analysis. Pain severity significantly differed between stellate ganglion block and standard therapy at 3 and 6 months in only 1 trial [33], but there were no significant differences in pain severity between nerve block and standard therapy throughout the observation period (up to 12 months) in the other 4 trials [29303436].
All of the trials included in this review report the adverse events associated with the relevant neural blocks. The common adverse events reported by the 3 trials on epidural and paravertebral blocks include dizziness, headache, and backache. One trial [31] reported a 5.5% incidence (16 of 290 patients) of dura puncture while administering epidural blocks. Two trials on the effects of epidural block reported the absence of adverse events. Commonly observed adverse events related to stellate ganglion block included drowsiness, local pain, changes in voice, and dysphagia. Most of the minor adverse events fully recovered within 2 weeks. One trial [35] reported study withdrawal due to adverse events related to interventions. Adverse events that caused withdrawal included nausea/vomiting and gastralgia in the standard groups, and dizziness, flushes, headache, backache, sweating, fainting, neck pain, stiffness, and the catheter falling out of the patient. None of the included trials in this review reported clinically meaningful or serious adverse events.
Go to :
DISCUSSION
The aim of this review was to investigate administering neural blocks in order to prevent the development of postherpetic neuralgia in patients with acute herpes zoster. Here, we present the primary outcomes (i.e., PHN incidence) according to > 90 days of persistent pain after the onset of herpetic skin rash because 90 days is widely accepted and reported in the literature [56]. Despite different study designs, neural block methodologies, observation periods, and outcome measurements, we determine the PHN incidence at 3 months after the final intervention in the 9 included trials. Three of 9 trials compared standard medical therapies and/or placebo injection with stellate ganglion block [303233], 4 of 10 trials performed comparisons with epidural block [28313536], and the other 2 trials performed comparisons with paravertebral block [2934]. The results of the meta-analysis of these trials revealed significant differences between the control groups and intervention groups in terms of the PHN incidence at 3, 6, and 12 months after inclusion. Among the trials included in our meta analysis, the incidences of PHN in the control and placebo injection groups were 2.8% and 42.7% at 3 months, 13.3% and 33.9% at 6 months, and 16% and 34.4% at 12 months. These values, which are considered the natural PHN incidence, are similar to previously reported studies [57]; in contrast, PHN incidence in the groups treated with nerve blocks was 0-26.7% at 3 months, 0-26.7% at 6 months, and 2-5.9% at 12 months. Incidence was significantly lower in comparison to the control groups during each observation period, and the efficacy of administering neural blocks to prevent the development of PHN increased over time.
Thus, we conclude that administering neural blocks during the acute phase of herpes zoster reduces PHN incidence, but significant heterogeneity between trials remains (P = 0.004, I2 = 75%). In subsequent analyses, we found that this heterogeneity was due to the type of neural block that was administered. When we conducted a subgroup analysis according to the type of neural block administered at 3 months after the final intervention, PHN incidence among patients who received stellate ganglion block was not significantly reduced [293233]. PHN incidence was 11% in the stellate ganglion block groups vs 31% in control groups (P = 0.12, I2 = 42%). However, in the 2 studies in which stellate ganglion blocks were administered more than twice [2429], incidence was significantly reduced in comparison with the control groups (P = 0.02). PHN incidence in the three trials that investigated the effects of continuous or repeated epidural blocks was significantly reduced (11% in epidural group vs 36% in the control group; P = 0.05, I2 = 41%) [283135]. However, the trial that investigated the effects of administering a single epidural block to 541 patients reported no differences in PHN incidence (21% in epidural group vs 24% in control group, P = 0.47) [36]. These results indicate that even when epidural blocks are administered to control pain during the acute phase of herpes zoster, the repetitive/ continuous blocking of noxious stimuli from reaching the central nervous system is needed in order to more effectively prevent PHN. Finally, 2 trials investigated the effects of administering paravertebral block to 255 participants and reported significantly reduced PHN incidence (9% in the paravertebral group vs 26% in the control group; P = 0.01, I2 = 37%) [2934]. Unlike single paravertebral block [33], however, administering a single epidural block did not effectively prevent PHN [36]. There are several possible explanations for this difference. First, the demographic characteristics of the control and intervention groups in the single epidural trial are not similar. The baseline pain intensity of the participants in the single epidural block trial was higher than the control group. Next, participants with systemic diseases such as diabetes or hepatic and renal diseases were excluded from the paravertebral block trial. Additionally, the administering of more complete and unilateral somatic and sympathetic blocks could have contributed to the lower PHN incidence in the paravertebral block trial.
In addition to PHN incidence, we also analyzed pain duration and intensity at 3 months after final intervention. Three included trials recorded pain duration [283334], and the results of the meta-analysis show that administering nerve blocks significantly reduced pain duration. Furthermore, in these trials, PHN incidence at 3 months was also significantly lower in the nerve block groups in comparison with groups that were administered standard therapy (7.3% vs 19.4%, P = 0.006). In the 5 included studies that evaluated pain intensity during the observation periods, only 1 study reported decreased pain intensity at 3 and 6 months in the nerve block group [33], but there was no significant difference in pain intensity at > 3 months in the remaining 4 studies [29333436]. However, we could not perform an additional meta-analysis because of the different data representations. These differences in pain evaluation methods may have resulted from the small sample sizes and low PHN incidences. Therefore, in order to investigate the efficacy of administering neural blocks to manage pain severity in patients with herpes zoster, a large, prospective, randomized trial is necessary in the future. Ideally, consensus-based multicenter studies are needed to compare outcomes.
Many studies investigate using neural blocks to manage pain due to herpes zoster. The results of randomized controlled trials on administering sympathetic nerve block reveal that applying nerve blocks shortens acute pain in herpes zoster [2527], and these results are consistent with our current findings. Unfortunately, these studies were excluded from this review because they did not report PHN incidence. A few retrospective and observational studies also investigate the preventive effects of early nerve blocks on the development of the PHN. Although several studies report the beneficial effects of applying early nerve blocks on PHN incidence [21223637], many other studies fail to demonstrate efficacy [202238]. Regardless of the results, most studies are weakened by the short-term follow-up period [27], lack of control groups [2021223839], unclear identification of herpes zoster patients [22], small sample sizes [2740], and the use of different clinical cutoff times to define PHN. All of the methodological concerns listed above make it difficult to interpret the results and draw conclusions. In a recent review conducted by the International Association for the Study of Pain Neuropathic Pain Special Interest Group (NeuPSIG), Dworkin et al. [42] reserved a conclusion regarding the preventive effects of neural blockade on the development of PHN due to the relative paucity of high-quality randomized controlled studies and different study results. However, there are no effective treatments that prevent PHN, and administering early nerve blocks may help prevent PHN in patients who require hospitalized care due to old age, severe acute pain, and rash [434445].
Our present review warrants cautious interpretation due to several limitations. First, although the results of this meta-analysis demonstrate decreased PHN incidence following the application of nerve blocks (14%) in comparison with the control groups (30%), the overall PHN incidence in nerve block group at 3 months does not differ from the previously reported studies on populations > 50 years (6.2-43%) [53546]. These results may originate from discrepancies in the inclusion criteria of the study populations, definitions of pain severity due to PHN, and possible overestimation. Second, due to the relative paucity of the high-quality randomized controlled trial, we only included 1 non-randomized trial [28]. In that trial, all admitted patients were consecutively allocated, and there were no differences in the demographic characteristics. Third, we cannot provide standard guidelines regarding nerve blocks, such as number, frequency, duration, or type of local anesthetics with or without steroids. However, a recent review on the use of epidural steroid injections—one of the most common practices in pain practice—concluded that minor variations in nerve block techniques are unlikely to significantly affect outcomes [47]. Lastly, most of the included trials in this review were not designed to set placebo intervention. The therapeutic effects of placebo interventions, especially in pain medicine, remain debatable [4849]. Injecting an inactive solution into the nerve tissue is unethical and is not a true placebo due to the lack of local anesthetic effects. In this review, 2 trials conducted by the same authors and institutions administered placebo interventions (electrolyte solutions) to control groups [1734], but there were no differences in PHN incidence in comparison with other studies in which the control groups did not receive placebo injections (P = 0.96; data not shown).
In summary, applying nerve blocks during the acute phase of herpes zoster shortens the duration of zoster-related pain. Stellate ganglion blocks fail to decrease the incidence of postherpetic neuralgia, but multiple blocks may demonstrate beneficial effects. Somatic blocks, including repeated/continuous epidural blocks and paravertebral blocks, prevent PHN and reduce the likelihood of occurrence. The preventive effects of early nerve block may be more potent when performed with repetitive/continuos treatment modalities than single administration. For future studies, consensus-based definitions of PHN, successful clinical cutoff points that define treatment outcomes, and standardized outcome assessment tools, including physical and emotional functioning, will be required.
Go to :
 XML Download
XML Download