

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Epidural corticosteroid injection (ESI) is being increasingly employed as a medical intervention for back pain and pain in the extremities [12]. It involves various techniques, including the transforaminal, caudal, and interlaminar approaches [3]. There are several methods for identifying the epidural space for ESI using the interlaminar approach, including the hanging drop and loss of resistance techniques [45]. With the interlaminar approach, air or saline solution is commonly employed for identifying the epidural space. Additionally, a variety of drugs, such as local anesthetics and corticosteroids, are used as well. The injected air, local anesthetic, saline, or corticosteroid is retained in the epidural space for a certain period of time after the epidural injection, which might contribute to the misreading of radiological images acquired after ESI.
Magnetic resonance imaging (MRI) of the spine is the preferred diagnostic tool for pathologic conditions affecting the spine and spinal cord. In recent years, there has been a dramatic increase in the availability and use of MRI [6]. However, acquisition of MR images following ESI might lead to signal distortion and the misreading of MR images. In patients receiving an ESI for treatment of spinal diseases, there is a possibility of misreading or difficulty in interpretation of MR images because of air or fluid in the epidural space after the injection. Kim et al. [7] reported a case of air bubbles mimicking disc herniation in MR images acquired after a cervical epidural block. Additionally, Ammirati and Perino [8] reported a case of symptomatic epidural air trapped in the spine after ESI. However, the effect of the ESI on MR images has not been adequately evaluated in terms of the types and duration of the persistence of abnormal findings.
In recent years, Davidson et al. [9] reported air and needle tracks in MR images acquired within 6 h after epidural injection. von Rothenburg et al. [10] reported soft tissue changes after epidural injection. However, these studies only evaluated MR images of a few patients acquired a short period after epidural injection.
With this background, we evaluated MR images acquired within 7 days after epidural injection through the interlaminar approach using the loss of resistance technique with air at the lumbar spine. The purpose of this study was to define the characteristics of abnormal changes in MRI findings after ESI at the lumbar spine.
MATERIALS AND METHODS
This study was a retrospective analysis of patients admitted to the pain management practice center of a single national university hospital between January 2006 and December 2015. The study was approved by the local institutional review board and registered with the Clinical Research Information Service of South Korea (http://cris.nih.go.kr; no. KCT0002116).
From among patients who received epidural injection using the interlaminar approach and the loss of resistance technique with air at the lumbar spine, 133 patients who underwent spinal MRI within 7 days after ESI were enrolled in the present study. Patients with a history of spinal surgery or other conditions that could have an impact on MRI findings, such as paresthesia or unanticipated dural puncture after ESI, were excluded. Subjects were classified according to either the presence of abnormal MRI findings after ESI or the interval between MRI and ESI.
All patients were administered ESI at the lumbar spine through the interlaminar approach by a staff member experienced in pain medicine. A 22-gauge Tuohy needle was placed at the midline. The epidural space was identified by the loss of resistance technique with fluoroscopic guidance while injecting a maximum of 2–3 ml of air. An 8-ml solution of lidocaine hydrochloride (0.5%, preservative-free) and triamcinolone or dexamethasone was administered into the epidural space at the lumbar spine. All patients underwent MRI within 7 days of ESI. Spinal MR images of the lumbar region were acquired with a 1.5T scanner, using a spine surface coil. The images were reviewed by a neuroradiologist blinded to the interval between the ESI and MRI and by pain physicians who participated in ESIs.
The primary outcome of measure was the proportion of patients with abnormal changes in MR images acquired approximately 24 h after ESI. The baseline proportion of an event was determined as 90%, based on the findings of previous studies [911]. A total of 35 patients were required to obtain a proportion of 90%, with an allowable limit of error of 10% with a two-tailed α-level of 0.05. The secondary outcome was the time point of the disappearance of abnormal MRI findings.
Data are presented as mean values ± standard deviation or number of patients (%). The one-sample proportion test was used for hypothesis testing of the proportion of patients with abnormal imaging findings due to ESI in MR images acquired approximately 24 h after injection. Group means were compared by the unpaired t-test, while group proportions were compared by the chi-square test. For all comparisons, P < 0.05 was considered significant. Statistical analyses were performed using SPSS, version 23.0 for Windows (IBM Corp, Armonk, NY, USA).
RESULTS
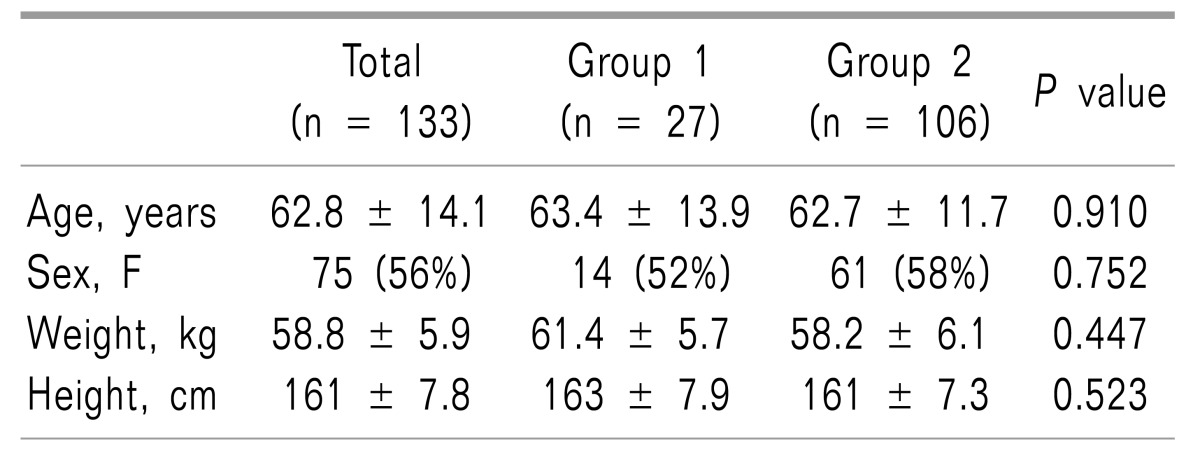
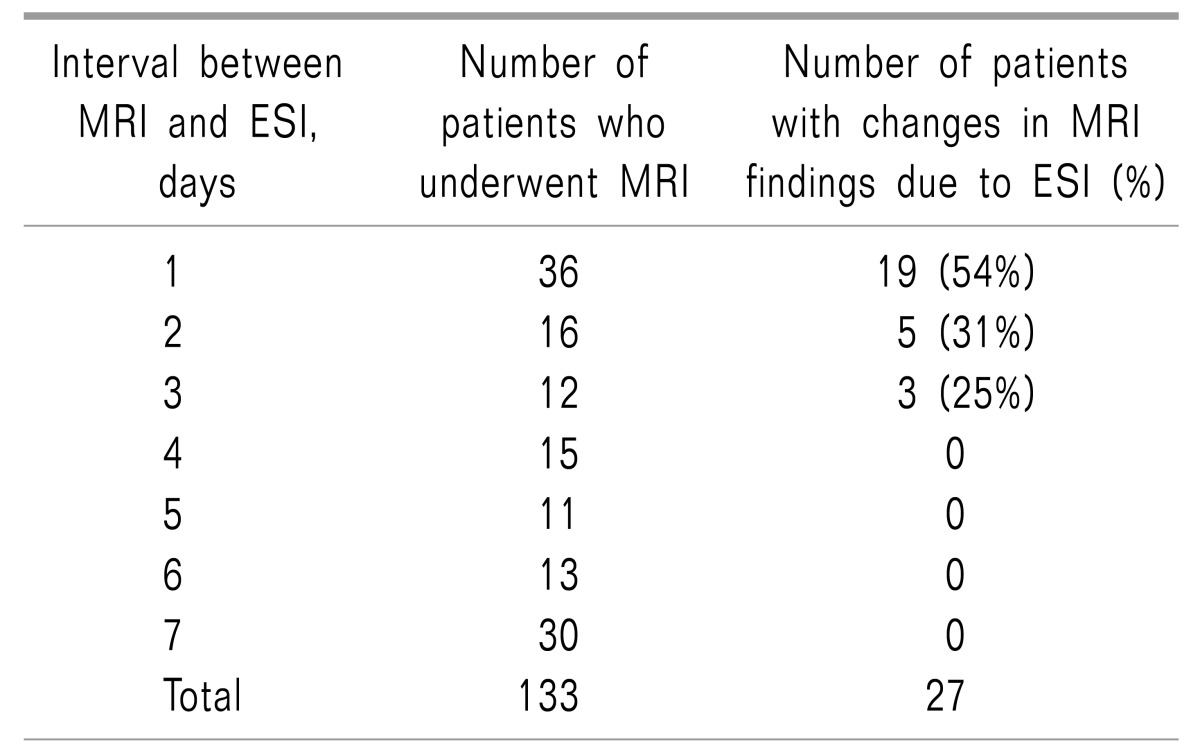
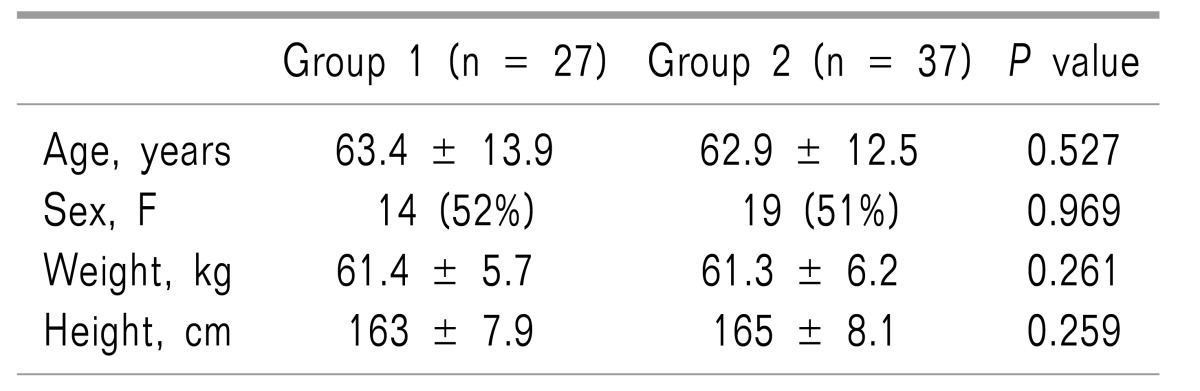
There were no significant differences in demographic characteristics between patients with or without abnormal imaging findings in MR images acquired within 7 days after ESI (Table 1). Of the 133 included patients, 27 exhibited abnormal changes in MRI findings after ESI. The incidences of abnormal MRI findings following ESI were 54%, 31%, and 25%, respectively, among patients who underwent MRI approximately 24 h, and 2 and 3 days after ESI (Table 2). None of the patients who underwent MRI 4 days after ESI exhibited abnormal changes in MRI findings.
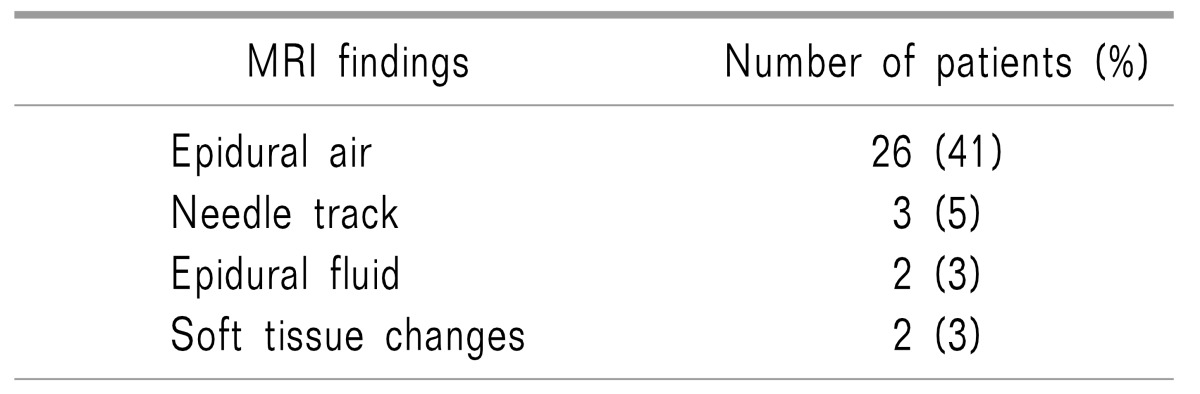
Among patients who underwent MRI within 3 days after ESI, there were no significant differences in demographic characteristics between patients with and without abnormal MRI findings (Table 3). Of the 64 patients, 26 (41%) exhibited epidural air; 3 (5%), needle tracks; 2 (3%), epidural fluid; and 2 (3%), soft tissue changes (Table 4).
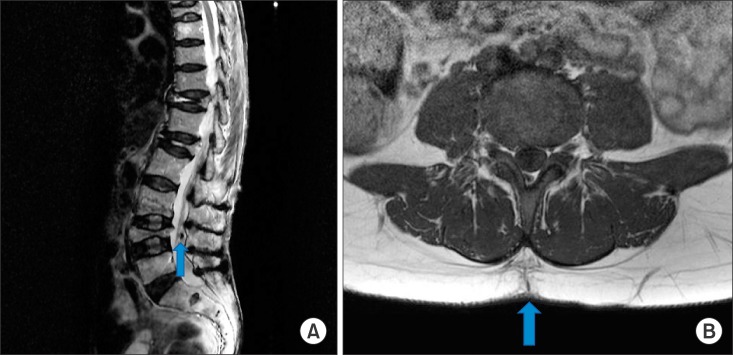
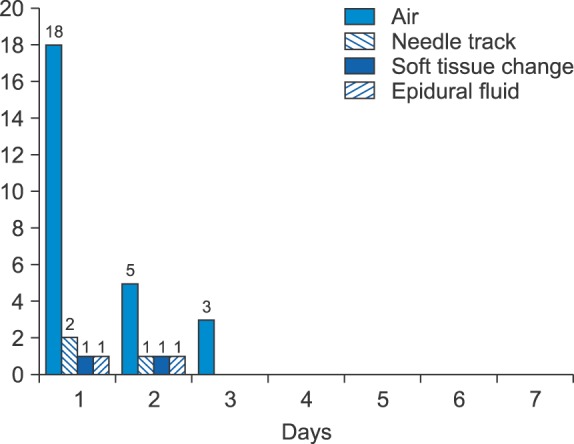
Representative MR images demonstrating air in the epidural space and a needle track in subcutaneous tissue at the level of the injection are presented in Fig. 1. The numbers of patients with changes in MRI findings after ESI are presented in Fig. 2. The numbers of patients with epidural air in MR images acquired approximately 24 h, and 2 and 3 days after ESI were 18 (50%), 5 (31%), and 3 (25%), respectively. The volume of epidural air exhibited a tendency to decrease.
DISCUSSION
Epidural steroid injection is a commonly used procedure not only in pain clinics but also in several medical departments. It is an effective treatment method for improving ambulatory and functional limitations and for pain management in patients with spinal diseases [1213]. Magnetic resonance imaging is the most sensitive and trustworthy diagnostic technique for spinal diseases; it has become increasingly common in recent years [1415]. It is useful for excluding other causes of spinal diseases. Despite the fact that MRI is the first line of diagnostic evaluation in patients with spinal diseases, interpretation of MR images acquired after an ESI might be confusing or impossible.
In the present study, the incidences of abnormal changes in MRI findings due to ESI were 54%, 31%, and 25%, respectively, in patients who underwent MRI approximately 24 h, and 2 and 3 days after ESI. Abnormal MRI findings included epidural air and fluid, needle tracks, and soft tissue changes. Epidural air was the most common abnormal finding (82%), and was observed in 41% of patients who underwent MRI within 3 days after ESI. No abnormal MRI findings following ESIs were observed in MR images acquired 4 days after ESI or later.
A history of invasive spine interventions (e.g., ESI) is known to be a risk factor for spinal epidural abscesses [1617]. The occurrence of a hematoma or an abscess after an ESI is an uncommon event, but one that might be associated with permanent neurologic dysfunction or death. Therefore, confirmation of a spinal hematoma or infection is considered an emergency requirement because neurologic prognosis and mortality depend on the interval between onset of neurologic symptoms and proper management. However, in such emergency situations, either symptom onset is delayed or only some of the symptoms are manifested. Changes in MR images acquired after an ESI might lead to confusion or misinterpretation of MR findings. Ikushima et al. [18] reported false positive findings mimicking those of an epidural abscess in the absence of infection in MR images of patients treated with an epidural infusion. In the present study, abnormal findings (e.g., soft tissue changes and epidural fluid) mimicking those of epidural infection were observed in 4 patients (3%) who underwent MRI within 3 days after an ESI. Based on the present results, abnormal findings on MR images acquired 4 days after an ESI could probably exclude the effects of an ESI on MRI findings.
In previous studies, image readers were able to correctly identify if an epidural injection preceded MRI in 90–93% of cases [911]; the corresponding value in the present study was 54%. This significant difference in results between the present and previous studies might have been because of several factors. First, patients in the two previous studies underwent MRI within 3–12 h of neuroaxial blockage, while those in the present study underwent MRI at approximately 24 h after ESI. Second, ESIs in these previous studies were administered with a 17-gauge epidural needle, while that in the present study they were administered with a 22-gauge epidural needle.
Previous studies [911] have reported air in 75–77% of MR images acquired after epidural injection. However, in the present study, MR images acquired at approximately 24 h after ESI demonstrated epidural air in only 50% of cases. The low incidence of epidural air in the present study could be because of the longer interval between the ESI and MRI (approximately 24 h) in comparison with that in the previous study (3–12 h). In the present study, the incidence of epidural air decreased gradually from 50% at 24 h after ESI to 25% at 3 days after ESI. Additionally, the volume of epidural air tended to decrease as well. There were no instances of epidural air among patients who underwent MRI 4 days after an ESI or later. Stevens et al. [19] observed air bubbles in all dogs in MR images acquired 24 h after ESI, and in 3 of 6 dogs in MR images acquired 2 days after ESI. Although small and few in number, the air bubbles were often located near intervertebral spaces. However, all of the air bubbles disappeared after 96 h, which corresponds with the findings of the present study.
The incidences of needle tracks reported in two previous studies [911] were 50% and 85%, respectively. However, MR images acquired after ESI in the present study demonstrated needle tracks in only 5% of cases. The low incidence of needle tracks in the present study could be because of the use of fine epidural needles (22 gauge) in comparison with the 17-gauge needles used in the previous study. Davidson et al. [11] reported paravertebral edema in 43% of MR images acquired within 3–12 h of labor and delivery after uneventful continuous epidural infusion through an epidural catheter. The relatively high incidence of paravertebral edema in this previous study might have been because of pregnancy, the use of 17-gauge epidural needles, continuous epidural infusion through an epidural catheter, or the short interval between the continuous epidural infusion and MRI. In the present study, MR images acquired after ESI demonstrated soft tissue changes in 3% of cases. While the low incidence of soft tissue changes and needle tracks in the present study could be because of the use of finer epidural needles (22 gauge) and longer intervals between the ESI and MRI in comparison with the previous study, it may also be attributed to the strict exclusion criteria of the present study. The present authors excluded findings that were difficult to distinguish from Baastrup's sign or degenerative changes [2021].
The present study has some limitations. First, we did not have post-epidural MRI data from the same patient acquired at different times. These data were not collected because we judged that subjecting patients to serial MRI would be an ethical issue under these circumstances. Second, this study only included patients admitted at a single institution. Since there is a possibility of discrepancies in the volume of injected air and the size or type of epidural needle among different institutions, it might be difficult to generalize the present findings. Further larger studies addressing all clinical scenarios that clinicians could possibly encounter are required to prevent the misreading of MR images acquired after ESIs.
In conclusion, based on the present findings, we recommend the use of fine epidural needles (22-gauge) when practitioners perform ESIs using the interlaminar approach and air at the lumbar spine. Pain physicians should consider the possibility of abnormal findings in MR images acquired after an epidural injection using the interlaminar approach and the loss of resistance technique with air at the lumbar spine.
 XML Download
XML Download