

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Low back pain is commonly defined as pain between the costal margin and the inferior gluteal folds [1]. The prevalence is known to vary from 49% to 70% [1]. Low back pain is categorized into specific and non-specific low back pain. Specific low back pain is derived from specific morphologic lesions and non-specific low back pain has no specific morphologic lesions [1].
Computed tomography (CT) or magnetic resonance imaging (MRI) are usually used to evaluate cause of low back pain and could reveal morphologic changes such as osteophytes, narrowing of the disk space, spondylolysis, Schmorl's nodes, or osteoporotic fractures. However, these findings could be observed in asymptomatic patients. Bone scintigraphy could show increased uptake at morphologic changes identified by CT or MRI imaging and the uptake of bone lesion could be assumed that it is related with clinical symptoms [2].
However, in some cases, diseases involving spine did not show increased uptake in bone scintigraphy. In one study, lumbar pain syndrome, herniated nucleus pulposus, post-surgery syndrome, and spinal stenosis did not show increased uptake, while tumor, Paget's disease, infection, pseudarthrosis, degenerative disk disease, spondylolysis, spondylolisthesis, and compression fracture showed often increased uptake [3]. Bone scintigraphy could be obtained either planar imaging or single photon emission computed tomography (SPECT). SPECT is known to have better resolution than planar images and helps to detect additional abnormal uptake in patients with low back pain [4].
Complex regional pain syndrome (CRPS) is a disorder showing continuous pain, which is characterized by sensory, vasomotor, sudomotor, or motor symptoms and signs [56]. It can be due to surgery, trauma, or minor injury [7] and nerve damage is the standard for classifying CRPS type I and II [58].
The diagnostic criteria of CRPS was developed by the International Association for the Study of Pain (IASP) through The Budapest Clinical Diagnostic Criteria for Complex Regional Pain Syndrome in 1994 [9]. However, the criteria of IASP had a tendency to over-diagnose CRPS and it has a difficulty in discriminating between CRPS and other neuropathic pain [10]. The criteria showed a sensitivity of 98%, and specificity of 36% [11]. In this context, refinement of the criteria was needed. In 2007, the revised criteria were introduced by IASP (Budapest Clinical Diagnostic Criteria) (Table 1) [12]. The revised criteria presented a sensitivity of 85% and a specificity of 69%, and reduced false positive diagnosis [12]. Although diagnostic procedures such as three-phase bone scintigraphy (TPBS), magnetic resonance imaging (MRI), X-ray, and skin temperature differences were not included in the revised criteria of CRPS, it could provide additional information to diagnose CRPS [1314]. The usefulness of bone scintigraphy for extremity pain has not been well studied. However, as the study of single photon emission computed tomography/computed tomography (SPECT/CT) has increasing, studies regarding SPECT/CT in patients with extremity pain has been performed.
In this review, we will discuss and illustrate the usefulness of bone scintigraphy and SPECT in pain medicine as follows: low back pain, complex regional pain syndrome, and pain on extremities and joints.
Go to : 
MAIN BODY
1. Low back pain
1) Metastatic bone disease
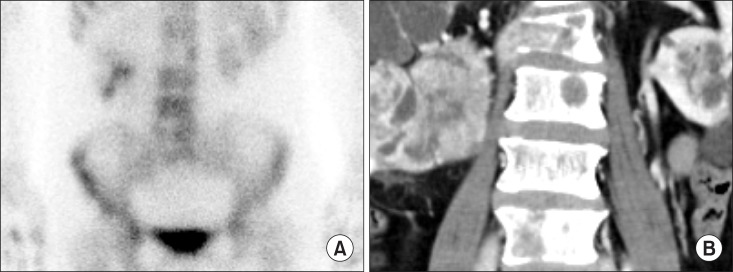
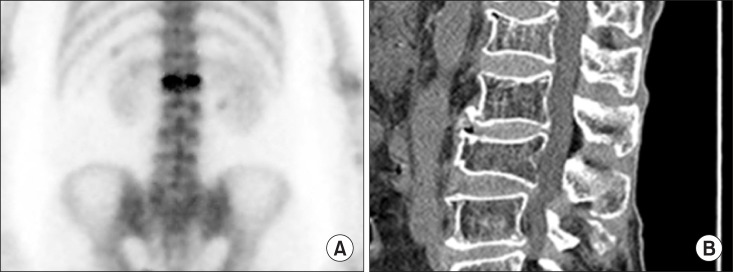
Bone metastases usually demonstrated as multiple foci with random distribution [15]. A 73-year-old female complained dyspnea and low back pain. CT chest was performed and the result reported lung cancer. Percutaneous needle aspirational biopsy revealed adenocarcinoma of lung. Subsequently, bone scintigraphy was performed and showed typical pattern of multiple bone metastases (Fig. 1A). CT showed sclerotic bone lesions consistent with bone scintigraphy (Fig. 1B). However, neuroblastoma, renal cell carcinoma, thyroid carcinoma, and anaplastic tumors are known to show ‘cold lesion’ in metastatic bone lesions due to aggressive tumor, disruption of the blood supply to the bone, or significant marrow involvement [16].
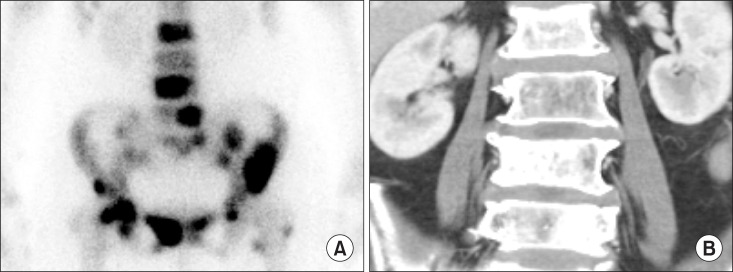
Fig. 2A showed ‘cold lesions’ at L2 and L5 spine in bone scintigraphy. CT showed osteolytic bone lesions at ‘cold lesion’ (Fig. 2B). Biopsy of L2 spine reported metastatic renal cell carcinoma. Bone scintigraphy is widely used to detect bone metastasis because of its effectiveness, low cost, widespread availability and favorable dosimetry [17]. The sensitivity and specificity of bone scintigraphy for detection of bone metastasis is 78% and 48% [17]. SPECT shows axial slices through the body, providing better localization of abnormal radionuclide uptake. The sensitivity and specificity of SPECT for detection of bone metastasis is 87% and 91% [17].
2) Benign bone tumor
Osteoid osteoma, osteoblastoma, giant cell tumor, and aneurysmal bone cyst are known to common primary benign spine tumors [18] and the uptake of these tumors is well shown in bone scintigraphy [16]. In case of chondroblastoma and enchondroma, bone scintigraphy show moderate uptake [16]. Hemangioma shows variable uptake [16].
3) Osteoporotic vertebral compression fracture
Osteoporotic vertebral compression fracture is a common cause of back pain in the elderly [19]. To diagnose symptomatic vertebra accurately before treatment is important. In one study, the treatment of osteoporotic vertebral fracture was performed in vertebrae that showed increased uptake on bone scintigraphy [20]. Ninety-three percent of patients reported pain relief after treatment [20]. As the uptake of vertebral fracture gradually decreases during the period of 6 to 24 months, bone scintigraphy can be used to discriminate between an acute fracture and an old fracture [21]. In addition, as bone scintigraphy can assess whole skeleton, it can detect additional traumatic bone lesions such as rib fracture during bed rest for treatment of vertebral fracture [22].
4) Vertebral osteomyelitis
Although bone is known to resistant to infection, however, trauma, bacteremia, surgery, or foreign bodies could cause osteomyelitis [23]. Vertebral osteomyelitis is increasing due to increased life expectancies, chronic disease, use of indwelling catheters, and immunosuppressive therapies [2425]. The lumbar spine is the most affected region of vertebral osteomyelitis [26]. Early diagnosis is often difficult and this may result in permanent neurological damage or even death [26]. Bone scintigraphy can detect osteomyelitis 10 to 14 days prior to plain radiographs [23].
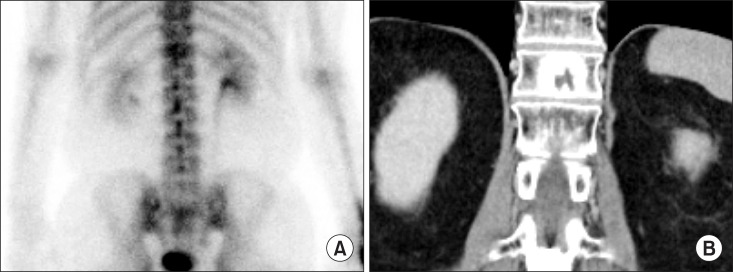
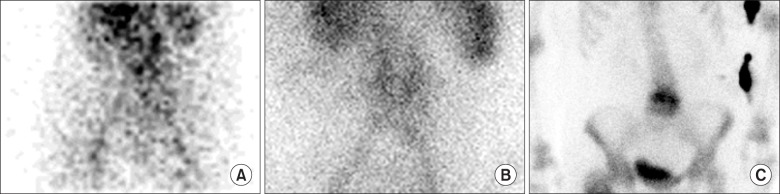
The typical pattern of vertebral osteomyelitis shows hyper-perfusion, hyperemia, and increased bone uptake in bone scan three phase. However, bone scintigraphy is sensitive, but not specific. Ga-67 scintigraphy can be used to supplement the low specificity of the study [27]. Fig. 5 shows typical pattern of vertebral osteomyelitis in 3 phase bone scintigraphy.
5) Facet joints arthropathy
The prevalence of symptomatic facet joint arthropathy varies from 5% to 15% [18]. The L4-L5 facet joints are the most commonly and severely implicated. Repetitive stress and low-grade trauma are major cause of facet joint arthropathy.
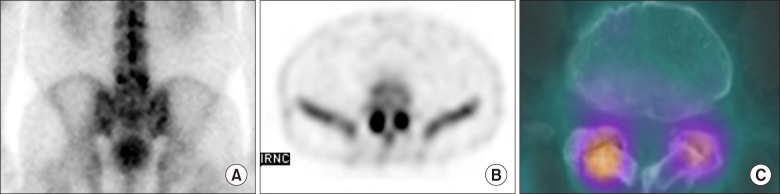
CT has high contrast between bony structures and soft tissues and show good delineation of osteophytosis, subchondral sclerosis and erosions, and capsular calcification. MRI has a superior delineation of soft tissues compared to other imaging modality. However, both modalities were not significant predictor of clinical outcome in the treatment of facet joint block while bone SPECT was able to detect appropriate patients to be treated [28]. Fig. 6A showed focal uptake at L5 on planar image. SPECT and SPECT/CT showed focal uptake at both facet joints (Fig. 6B and 6C).
6) Spondylolysis
Spondylolysis is a disease showing bony defect in the pars interarticularis of the vertebral arch [29] and it is thought to be one of the most common causes of low back pain with incidence of 3-6% [3031]. The major site of spondylolysis is a L5 level, and spondylolisthesis is commonly accompanied in patients with bilateral spondylolysis [29].
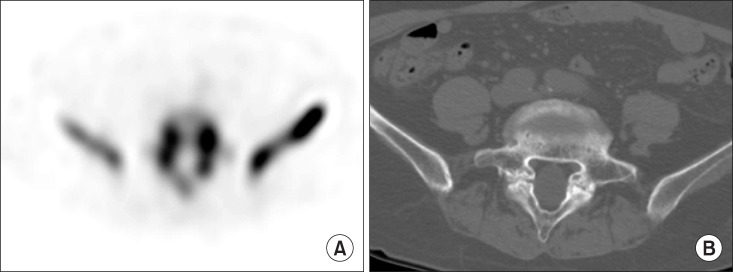
MRI is usually performed in the evaluation of children and adolescents with back pain [30]. However, MRI missed a spondylolysis in over half of the adolescents [30]. In one study, bone scintigraphy with SPECT showed superior diagnostic performance than MRI in detecting spondylolysis [32]. Fig. 7A shows spondylolysis of L5 on SPECT. Fig. 7B showed a bony defect in the pars interarticularis on CT.
2. Complex regional pain syndrome (CRPS)
1) Three-phase bone scintigraphy (TPBS)
The radiopharmaceuticals used in TPBS were technetium-99m-labeled methylene diphosphonate, hydroxyl methylene diphosphonate, and dicarboxypropane diphosphonate, which did not show the significant difference between them [33]. These radiopharmaceuticals are absorbed to hydroxyapatite and calcium pyrophosphate of bones [34]. The uptake of radiopharmaceuticals in bones is associated with blood flow and osteoblastic activity, seen in fractures, osteomyelitis, and bone metastasis [35]. “Cold defect”, absent of uptake, could also be seen in bone scintigraphy by the following situations: 1) aggressive processes, 2) indolent processes that induce little healing reaction, 3) disruption of blood flow [35].
TPBS consists of flow, blood pool, and delayed phases [36]. The flow phase consists of serial 2- to 5-second dynamic images acquired for 60 seconds and reflects the relative amount of blood flow to the area of interest. The blood pool phase is obtained by static images for 5 minutes immediate after flow phase reflecting the amount of activity that has extravasated into the tissues around the area of interest. Finally, the delayed phase is obtained at 2-4 hours after radiopharmaceutical injection reflecting the rate of bone turnover [3637]. Until now, the mechanism of uptake in TPBS in patients of CRPS is not fully understood. It might be due to decreased sympathetic activity, abolished sympathetic activity, or neurogenic inflammation [38].
2) Diagnostic performance of TPBS in CRPS
Diagnostic performance of TPBS in CRPS ranged widely as a sensitivity between 14% and 100% and a specificity between 50% and 100% [39]. Ringer et al. [40] showed the pooled sensitivity of 87% and the pooled specificity of 69% in a meta-analysis. False positive TPBS might be due to other clinical conditions mimicking similar biological processes such as posttraumatic or post-operative bone affections according to Ringer et al. [40].
Recently, Wertli et al. [41] reported diagnostic accuracy for TPBS according to diagnostic criteria. They reported the pooled sensitivity of 93.3% and the pooled specificity of 82.9% without diagnostic criteria, 90.6% and 94.6% with Kozin criteria, 60.8% and 89.7% with IASP criteria, and 55.1% and 93.5% with Budapest criteria. Wüppenhorst et al. [38] reported that diagnostic performance was limited by duration of CRPS, and the optimum time to use TPBS is within the first 5 months after onset of symptoms [38].
Schürmann et al. [42] compared the diagnostic performance of TPBS with thermography, and MRI. The sensitivity of TPBS, and MRI were 19%, and 43% at 8 weeks, and 14%, and 13% at 16 weeks after trauma, showing the poor sensitivity of both modalities. However, the specificity of TPBS, and MRI were 96%, and 78% at 8 weeks, and 100%, and 98% at 16 weeks after trauma, which might have a potential to rule out CRPS. According to a meta-analysis by Cappello et al. [13], TPBS had a significantly higher sensitivity and negative predictive value than MRI.
3) Findings of CRPS on TPBS
Although TPBS findings are variable depending on the duration of disease, the typical pattern of TPBS are increase of the uptake in all of blood flow, blood pool, and delayed phases [3643]. Fig. 8 demonstrated a typical finding of CRPS on TPBS. Sixty-three years old female fell down and the styloid process of left radius fractured. Long arm cast was applied as a treatment. After 2 months, she complained of pain and swelling of left hand. X-ray showed osteopenia and styloid process fracture of left radius. TPBS showed increased uptake at left hand and wrist in all three phase. This pattern is commonly demonstrated in the early phase of CRPS [43].
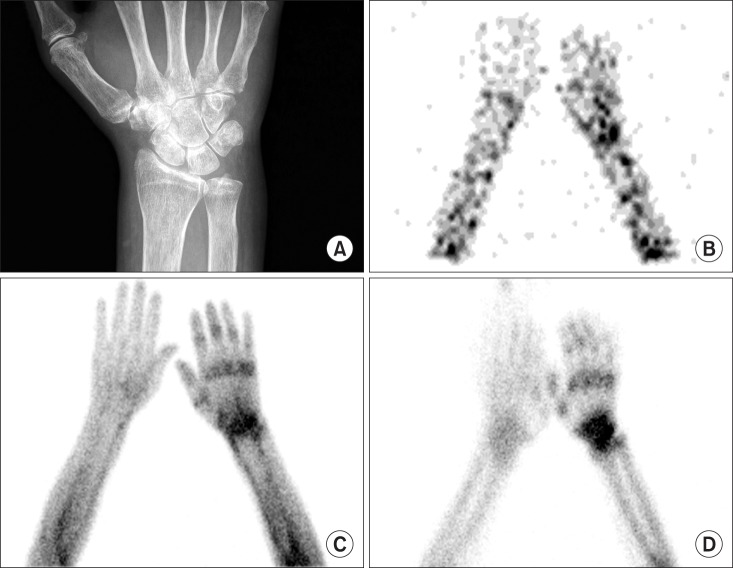
Fig. 9 presented an atypical finding of CRPS on TPBS, which is increased uptake only on delayed image without abnormalities on flow and blood pool phases. Forty-six years old female complained of pain of right shoulder and wrist after fell down. After 5 months, she underwent surgery due to carpal tunnel syndrome of right wrist. After surgery, she appealed sustained pain at right shoulder, right arm, right elbow, and right wrist and hypoesthesia of right 1st to 3rd fingers. TPBS was done at 6 years after initial trauma. Images of flow phase and blood pool phase did not show the abnormalities, however, increased periarticular uptake was seen on a delayed image.

Fig. 10 demonstrated the other type of atypical findings of CRPS on TPBS. A 44-year-old male complained of sustained left hand pain after median nerve decompression surgery. With suspicion of CRPS, TPBS was performed 15 months after initial trauma. The uptake of flow phase and blood pool phase decreased comparing with contralateral side, while increased uptake was seen on a delayed image. This pattern of TPBS in CRPS was known rare in adults, however, young patients with CRPS usually demonstrated this atypical finding [44]. Low et al. [45] reported that 7 of 14 young patients with CRPS showed the decreased uptake in the flow phase of TPBS. In case of paralysis and immobilization, TPBS could exhibit the similar finding [43].

Fig. 11 showed another pattern in CRPS. A 54-year-old male complained of left wrist pain after trauma. Three years after trauma, TPBS was done to evaluate the possibility of CRPS. All three phases showed decreased uptake at the affected limb. However, including decreased uptake on a delayed image as a positive finding of CRPS is controversial. Decreased uptake on a delayed image might be a supportive finding for CRPS [39], however, it could be caused by disuse of affected limb [46].

3. Pain on extremities
1) Upper extremity
Few studies regarding usefulness of bone scintigraphy in patients with upper extremity pain are published [47]. Hirschmann et al. [48] reported that SPECT/CT in patient with shoulder pain could differentiate between infection and humeral head necrosis, identify prosthesis loosening, and localize exact sites of pain. The study for diagnosing acromioclavicular joint pain showed that bone scintigraphy had better diagnostic performance than MRI [49]. In patients with hand and wrist pain, MRI showed higher sensitivity (86%) than SPECT/CT (71%), however, the specificity (20%) was lower than SPECT/CT (100%). Accuracy of both MRI and SPECT/CT were 73% and 77%, respectively [50].
2) Lower extremity
Total hip replacement is commonly undertaken to relieve pain and functional disability of hip osteoarthritis [51]. Aseptic prosthesis loosening is known to most common cause of prosthetic failure [52]. MRI and CT are limited by metal artifacts to evaluate loosening of prosthesis [53]. In one meta-analysis, bone scintigraphy showed a pooled sensitivity of 85% and a pooled specificity of 72% [54]. In a study regarding diagnostic performance between planar/SPECT and SPECT/CT, SPECT/CT showed higher sensitivity (93.7%) than planar/SPECT (77.08%), especially in loosening of acetabular component [53].
Anterior knee pain, also known as patellofemoral pain syndrome, is one of common causes of knee pain [55]. It could be due to patellar pad lesions, patellar tendinopathy, patellofemoral malalignment, and chondral lesions of the patellofemoral joint [55]. However, these lesions are not always correlated with symptoms [55]. SPECT/CT showed that patella uptake was associated with treatment response and severity of patellar condral lesions [55]. Similar to painful hip prosthesis, In patients with painful knee prostheses, SPECT/CT could diagnose accurately infection and prosthesis loosening and had clinical impact on 85.5% of patients [56].
X-ray, US, CT, and MRI have been used to evaluate pain on foot and ankles [57]. The diagnosis of foot and ankle lesions is difficult due to complex anatomy and functions [57]. Singh et al. [57] reported that SPECT/CT had a high diagnostic accuracy in diagnosing foot and ankle lesions. The sensitivity and specificity were 94% and 95.45%m respectively [57]. Compared with MRI, the diagnostic performance was comparable to MRI [58]. The sensitivity, specificity, positive predictive value, and negative predictive value of SPECT/CT were 93%, 48%, 56%, 91%, and that of MRI were 98%, 24%, 48%, 95% [58]. Moreover, SPCET/CT had a high clinical impact on treatment decision. 68.6% of patients were changed diagnosis and treatment by SPECT/CT [59].
3) Rheumatoid arthritis
Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic inflammation of joint [60]. Several studies reported that bone scintigraphy did not discriminate active inflammatory joint from inactive joint in RA patients [6162] and was inferior to ultrasonography to detect early RA [63]. However, recent study showed that TPBS had better diagnostic performance than conventional bone scintigraphy and was helpful in the diagnosis of RA in patients with insufficient evidence of RA [6465].
Go to :
CONCLUSIONS
In patients with low back pain, CRPS, and extremity pain, nuclear medicine imaging is an essential imaging modality. Bone scintigraphy is superior to other imaging modalities in evaluate low back pain. CRPS, and extremity pain. Further studies are needed to investigate the underlying mechanisms of uptake in CRPS.
Go to :
 XML Download
XML Download