

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Cervical epidural steroid injection has been used for conservative management in neck pain and/or cervical radicular pain for many years [123]. Even though its mechanism of action is not well known, it is believed that epidural steroids and local anesthetics interrupt nociceptive input or alter the pattern of central neuronal activities [34]. The potent anti-inflammatory properties of the steroid and wash out effect of inflammatory mediators were accomplished by delivering the steroid and local anesthetic solution into the target area [56].
The effect of CIESI is not well studied and is more controversial than lumbar epidural steroid injection [2378910]. Past outcomes of CIESI using blind technique were poorer [781112]. Fluoroscopy guided studies suggest CIESI is beneficial for the management of cervical radicular pain, but the evidence is still weak, due to the lack of a control group that does not exclude natural improvement [7101314]. However, CIESI has been suggested as a general treatment option when avoiding surgical treatment in patients with radicular pain [15]. Recent meta-analysis showed that the pain from cervical disc herniation was well managed, but the pain management for axial discogenic pain, central spinal stenosis, and post-surgery syndrome was only fair [3].
Analysis of the predictive factors for CIESI is necessary for appropriate treatment selection and outcome prediction, especially for considering complications. In previous studies, effectiveness and the predictive factor for CIESI have been evaluated with primary symptom, pain duration, MRI findings, serologic tests, or other characteristics independently [7111415161718192021222324]. It is widely accepted that CIESI is more effective in treating radicular pain than axial neck pain, but there has been little study comparing these directly. Moreover, the difference in the efficacy of CIESI between MRI findings is inconsistent [111618]. In this retrospective study, we evaluated the therapeutic response of CIESI according to pain patterns and MRI findings altogether for clinically practical use.
Go to : 
MATERIALS AND METHODS
1. Patients
After approval of the Institutional Reviews Board (No. 2015-03-126-001), the electronic medical records of 192 patients managed by fluoroscopy guided CIESI (from January 2010 to December 2014) in our pain clinic were reviewed. All patients were diagnosed by history taking and physical examination. CIESI was not performed for neck pain with multiple site pain syndromes, such as in fibromyalgia or rheumatoid arthritis. Neck pain or referred pain suspected of arising from facet joint pain syndrome or myofascial pain syndrome were differentiated by Spurling's test, a nerve root compression test, a trigger point examination, and diagnostic blocks such as cervical medial branch blocks. We attempted a CIESI in these patients when their symptoms were not explained nor improved with the theses diagnoses, but confirmed with other, more appropriate disagnoses on MRI. General contraindications of CIESI, including sepsis or local infection in the cervical area and coagulopathy, were ruled out by history, and physical and laboratory examination. Antiplatelet agents were stopped for an appropriate period with the permission of the prescribing physician. Inclusion criteria were: (1) the first CIESI for the patient for either neck pain or cervical radicular pain, (2) cervical MRI study prior to the CIESI. Exclusion criteria were: (1) pain due to cancer, fracture, or infection, (2) patients with a poorly controlled co-existing psychiatric diagnosis or where there was a suspicion of secondary gain, (3) history of previous posterior neck surgery, (4) a previous CESI within 1 year, (5) all other interventions for cervical pain management including acupuncture, trigger point injections, medial branch blocks, facet joint blocks, and neuroplasties before the second visit after CIESI, and (6) incomplete medical records of the primary symptoms or MRI findings.
2. Injection technique
All CIESIs were performed under fluoroscopic guidance by physicians with over 5 years of experience. The level of CIESI was determined by MRI findings and symptoms, the most suspicious level or one below, but mostly C7-T1 and limited not to exceed C5/6 due to concern with spinal cord injury or dura puncture. The patients were placed in the prone position, and the neck was flexed using a pillow under the chest. After an aseptic preparation and local anesthetic infiltration, a 22-gauge Tuohy needle was inserted at the midline of the C7-T1 interspace at anteroposterior view. If a loss of resistance was felt during the advance of the needle near the base of the spinous process at lateral view, 1 cc of contrast medium was injected at real time lateral and anteroposterior view to confirm the epidural space following negative aspiration. A mixture of 2 ml of 0.2% ropivacaine with 5 mg of dexamethasone was then slowly injected into the epidural space. After the procedure, the patients were observed for 30 minutes, and any observed complication was recorded.
3. Review of clinical data
Patients' demographic variables such as age, gender, body mass index (BMI), and history of whiplash injury were available from the initial pretreatment clinical evaluation. Self-reported neck or radiating pain severity was recorded with a 100 mm line visual analog scale (VAS). MRI findings and laboratory data of the erythrocyte sediment rate (ESR) and C-reactive protein (CRP) level in the serum were also collected.
All patients were classified by (1) pain site; neck pain/radicular pain, (2) pain duration; acute/chronic, and (3) MRI findings; herniated intervertebral disc/spinal stenosis. Cervical radicular pain and neck pain were sorted from pain histories and physical examination records. We defined radicular pain as pain radiating to the shoulder or arms, and axial neck pain as pain from the upper neck to interscapular area. Patient having both radicular pain and neck pain were classified as having radicular pain. We defined chronic pain as pain lasting more than 6 month from the first symptom (not recent aggravation), 4 pain patterns were classified as acute neck pain, acute radicular pain, chronic neck pain, and chronic radicular pain. When MRI findings showed HIVD and spinal stenosis simultaneously, we selected radiologic findings more likely to provoke the patient's pain.
Therapeutic response was evaluated by changes on the VAS in the initial region at the second visit (from 2 week to 2 month after CIESI). We regarded more than a 50% reduction of the VAS score by the second visit as a responder [11151622]. Major procedure-related major complications were also reviewed.
4. Statistical analysis
Demographic variables between the two groups (responder vs. non-responder) were analysed using two sample t-tests if they were continuous variables, or a Chi-square test if they were categorical variables. Evaluation of effectiveness was compared with the paired t-test. And correlation of the pain pattern with MRI findings was analyzed by multivariable logistic regression analysis to avoid the confounding effect. IBM SPSS Statistics version 22 (SPSS Inc., Chicago, IL, USA) software was used throughout, and P values < 0.05 were considered statistically significant.
Go to :
RESULTS
Among 192 patients, 64 patients were excluded and a total of 128 cases were able to be analyzed. The reasons of exclusion were mostly incomplete medical records of primary symptom at the second visit followed by MRI without interpretation, previous CESI or neck surgery, and rarely concurrent other cervical interventions. Only 2 cases had immediate procedure-related complications (vascular injection and subdural injection).
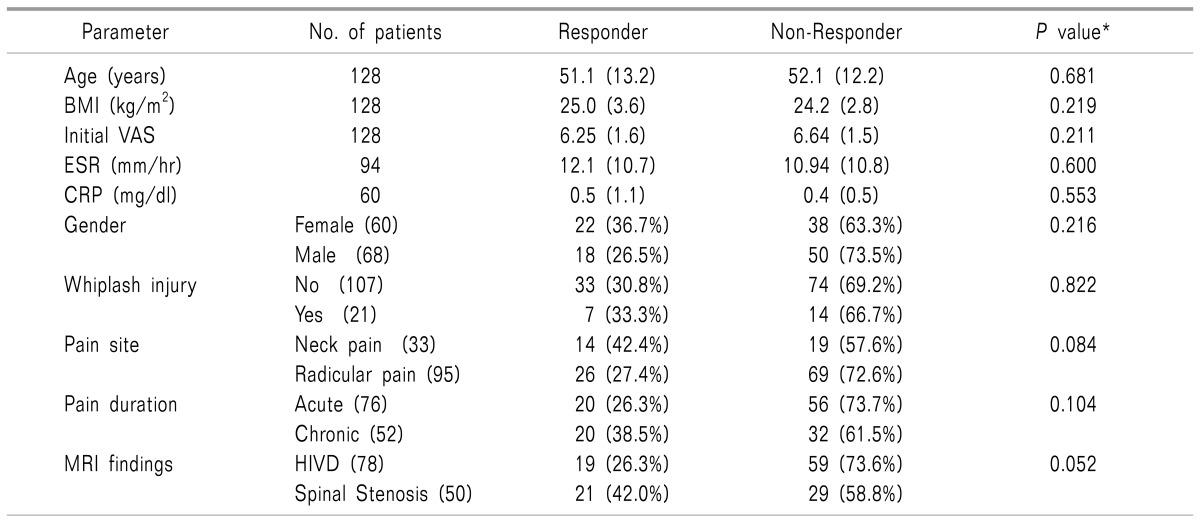
Among the 128 patients, CIESI was effective in 88 patients (68.8%), but not in 40 patients (31.2%). The interval from CIESI to the follow up evaluation (second visit) was not significantly different between the responder and non-responder groups (36.7 ± 14.3 vs. 35.3 ± 13.8 days, P = 0.645). There was no significant difference between responder and non-responder groups in age, gender, BMI, initial VAS score, history of whiplash injury, ESR, CRP, pain site, pain duration, and MRI findings (Table 1).
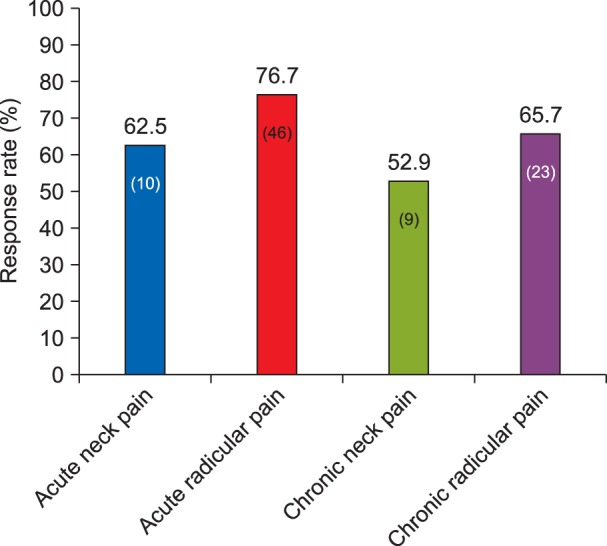
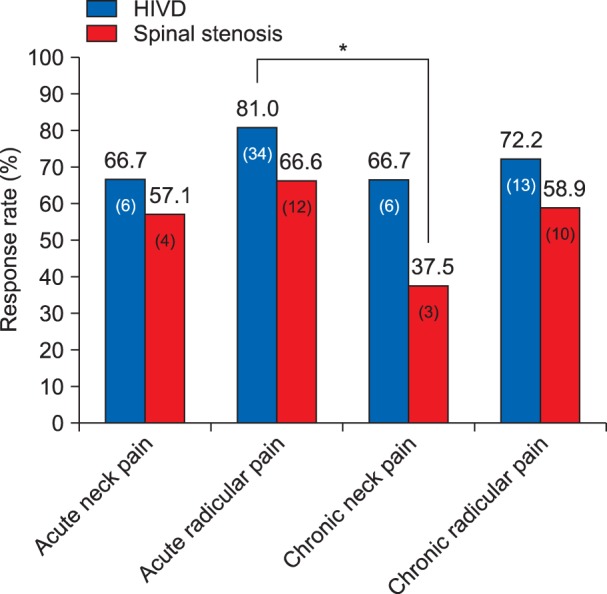
All 4 pain pattern groups showed significant symptom improvement after CIESI (P < 0.001), but there was no significant difference between groups (Fig. 1). The acute radicular pain group was the best responder (76.7%), and the chronic neck pain group (52.9%) was the worst responder, but there was no significant difference between the two groups (P = 0.06) (Fig. 2). The patients with acute radicular pain with HIVD (81.0%) were the best responders and the patients with chronic neck pain with spinal stenosis (37.5%) were the worst responders in the classification of pain patterns and MRI findings (P = 0.04) (Fig. 3).
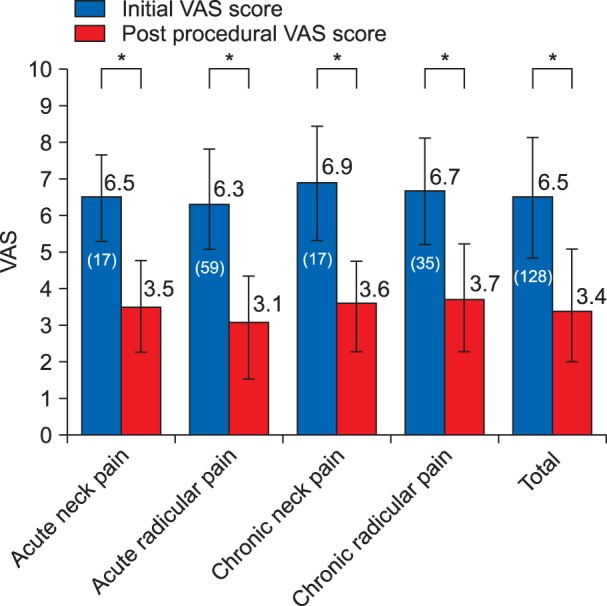 | Fig. 1All pain pattern groups show significant pain reduction after cervical interlaminar steroid injection, but there was no significant difference between groups. The number in parenthesis means actual number of patients. *P < 0.05.
|
Go to :
DISCUSSION
In this study, mean VAS was decreased from 6.5 to 3.4 and the overall therapeutic response rate was 68.8% after CIESI in neck pain with or without radicular pain. Previous studies have reported the short term effective rate of CIESI as widely as 64-87% [123]. This diversity in the therapeutic response of CIESI might be influenced by intervention technique including drugs, evaluation method, and patients' characteristics.
Although, statistically not significant, the 72.6% therapeutic response rate in radicular pain after CIESI seems better than the 57.6% of those with pure neck pain in our study. There are several studies which have insisted that cervical epidural steroid injection worked better for radicular pain than neck pain, although they lacked a direct comparison between them [23451011]. Like us, Kwon et al. [16] also failed to find significant difference between the radicular pain and neck pain groups in the effectiveness of CIESI. Any structures in the neck including the intervertebral discs, facet joints, and nerve roots may cause neck pain, upper extremity pain, and associated symptoms [221]. CIESI are not be recommended for axial neck pain unless herniated disc with radiculitis and spinal stenosis are concomitant [22]. It is not easy to identify or differentiate cervical radicular pain and somatic referred pain clinically as the pathoanatomical cause [2], and we might have not differentiate them exactly in this study. Most patients with neck pain don't have structural abnormality [23], but there are several distinguishing features between cervical radicular pain and somatic referred pain. Rowlingson and Kirschenbaum [1] concluded that history, physical examination, and laboratory studies seem to be a satisfactory criteria for CIESI for cervical radicular pain. Shakir et al. [17] distinguished the characteristics of radicular pain as being above and below the elbow to differentiate radiculopathy from referred pain. But there was no difference in outcome after a transforaminal epidural steroid injection between them.
Our study shows that the 73.7% response rate of CIESI in the acute pain group seems better than the 61.5% rate in the chronic pain group, but it was not statistically significant, as in previous studies [111617]. Kwon et al. [16] reported that response rate of CIESI was 80.4% with less than 6 months of duration and 60.0% with more than 6 months. Shakir et al. [17] also reported that the response rate in CIESI for pain duration of less than 1 year was 68% and that in pain duration of more than 1 year was 59%. Peripheral and central sensitization caused by chronic irritation might develop neuropathic pain which is resistant to epidural steroid injection [25].
According to the response rate with MRI findings, CIESI for HIVD was more effective than for spinal stenosis (73.6% vs. 58.8%), but the difference is not statistically significant. Kwon et al. [16] reported that patients with HIVD showed better pain relief than those with spinal stenosis (86.1% vs. 60%). They supposed that steroids are less effective in treating the pain from the mechanical compression of nerve roots in spinal stenosis than in the chemical inflammatory reaction in HIVD. But Ferrante et al. [11] reported that a radiologic finding of spinal stenosis or spondylosis was associated with good pain relief, and HIVD or a normal finding has been suggested to be a statistically significant predictor of poor outcomes after CIESI. Fish et al. [18] also reported that only central canal stenosis was significantly responsive to CIESI in radicular pain among more sophisticatedly classified MRI findings (disc herniation, nerve root comprise, foraminal stenosis, and central canal stenosis). They suggested that central canal stenosis may be an important factor in responding to CIESI, because disc herniations may escape nerve root impingement with a wider spinal canal, whereas a canal stenosis would not allow this. They also insisted that the observer's variations in the interpretation and classification of MRI findings, and ranking them according to severity could be the cause of these discrepancies, especially when they coexist and are ambiguous. According to the recent review and guidelines, the evidence of CIESI for HIVD is more stronger than that of spinal stenosis [231026].
This study also investigated some other predictive factors of CIESI. Therapeutic response to CIESI is not significantly different in gender, age, and history of whiplash injury as in other previous studies [111617]. Ackerman and Zhang [20] reported good response to lumbar epidural steroid injection in back pain patients with low serum CRP, and they concluded that elevated CRP levels may be useful for objectively evaluating and predicting responses to lumbar epidural steroid injection in those patients with lumbar radiculitis. But, in our study, there were no significant differences of inflammation markers (ESR and CRP) between responders and non-responders after CIESI, as in another study in back pain patients [24].
This study has several limitations. Firstly, it was not controlled due to being a retrospective study, especially since oral medication was not equally managed after CIESI. However, most patients continued their routine analgesics until their next visit. And we didn't routinely assess patients' outcomes with tools other than VAS. Our study lacked data regarding patient's satisfaction, functional status, and other scales for quality of life after CIESI. Secondly, upper arm and shoulder pain of some in the radicular group might be referred pain rather than cervical radicular pain. But we know there is no reliable method to distinguish them exactly, even with diagnostic nerve blocks. Thirdly, as mentioned earlier, we admit the possible presence of error in the interpretation and classifying of MRI findings. Lastly, this study was focused on the very short term effects of CIESI.
In this retrospective study, we found that non-significant predictors of an improved outcome including pain site (radicular pain), duration (less than 6 month), and MRI findings (HIVD) show an improved response trend after CIESI, respectively. And we found that the patients with HIVD confirmed by MRI with acute radicular pain were the best responders and those having spinal stenosis with chronic neck pain were worst responders after CIESI. We recommend that the physician who considers CIESI as a conservative treatment option should refer the aforementioned result as well as the cost effectiveness and complication of it. Further well-controlled study is necessary to evaluate more evidenced and the long term effects of CIESI.
Go to :
 XML Download
XML Download