

 PDF
PDF Citation
Citation Print
Print


Foraminal or extraforaminal far lateral disc herniations (FLDH) extending into or beyond the foraminal zone have been recognized as between 7-12% of all lumbosacral disc herniations [1]. The term "far lateral" is often used to describe a lumbar disc herniation that compresses the exiting nerve root at the same level, lateral to the neural foramen or further laterally [2]. Conventional posterior laminectomy may not provide good access to a herniation that lies far lateral to the lateral margin of the pedicle. In the era of endoscopic surgery, employment of the endoscopic technique through a percutaneous approach to treat such FLDH patients can decrease the surgical morbidity while achieving similar or better outcomes [3]. However, there is no consensus as to the degree of migration that can be removed using current instruments and techniques. The authors present a case of an endoscopically resected lumbar extruded disc to the left extraforaminal zone with superior foraminal migration which had led to foot drop at the level of L5-S1 through the epiduroscopic technique without facetectomy.
CASE REPORT
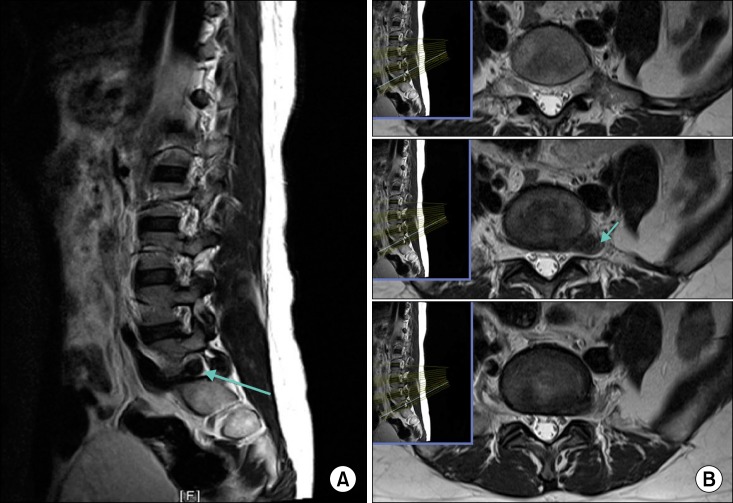
A 41-year-old female presented with a chief complaint of lancinating pain in her lower back, radiating to the left buttock, thigh, and calf in the L5 dermatome. The onset of her symptoms had been five days earlier. The patient had been treated with nonsteroidal anti-inflammatory drugs, opioids, and L5 nerve root block, which had offered only temporary relief. Her average pain score according to the Numeric Rating Scale (NRS) was 8/10, and it was 9/10 at its worst. Her Oswestry Disability Index (ODI) score was 84. Her Straight Leg Raising (SLR) test showed pain at an angle of 10 degrees on the left side. Great toe dorsiflexion and ankle doesiflexion were graded as 3/5 on the left side. Magnetic Resonance Imaging (MRI) showed disc extrusion to the left extraforaminal zone with superior foraminal migration below the L5 pedicle with a left L5 nerve compression (Fig. 1). The patient was then scheduled to undergo percutaneous endoscopic discectomy for L5-S1 FLDH with a paraspinal approach.
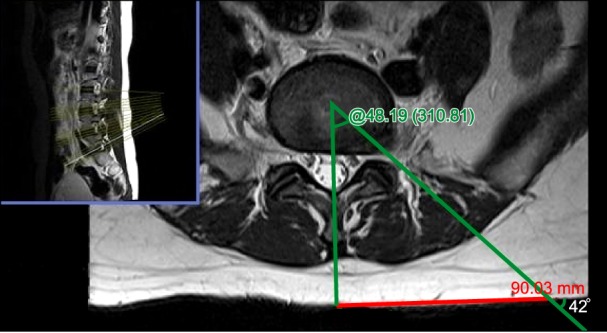
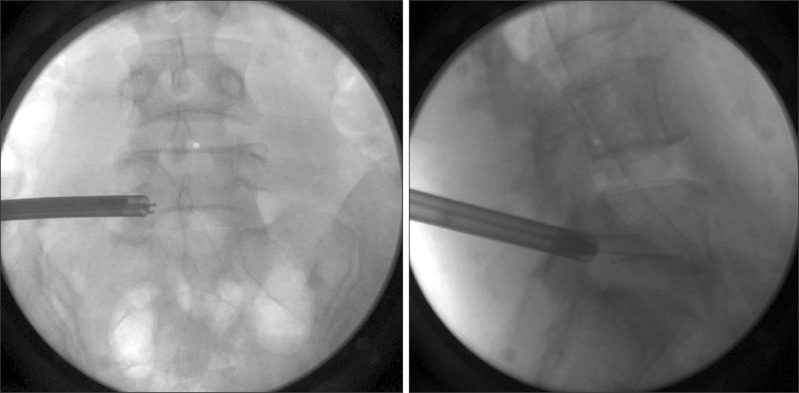
The paraspinal PELD procedure was performed under local anesthesia and conscious sedation. The patient was positioned prone with slightly flexed hips and knees on the Wilson frame. The Panoview Plus discoscope (Richard Wolf GmbH, Knittlingen, Germany) was used for the procedure. We used axial MR images to calculate the distance from the midline to the skin entry point of the needle (Fig. 2). Percutaneous entry was established at the L5-S1 foramen entering through the skin 9 cm lateral to the midline at a 42 degree angle. The final target point for introducing the spinal needle was the medial pedicular line on the anteroposterior (AP) image and the posterior vertebral line on the lateral image. Next, an epidurography was performed using contrast medium (Pamiray, Dong Kook Pharm Co., Ltd., Seoul, Korea) to confirm the location of the exiting and traversing root. After targeting the central part via Kambin's triangle, insertion of the spinal needle into the L5-S1 disc was performed. The nucleus pulposus was stained blue with 1 mL of indigo carmine (Carmine, Korea United Pharmaceutical, Yoenki, Korea). The following steps were then performed: a guide wire was inserted through the spinal needle; the spinal needle was removed; a small incision was made in the skin at the entry site; a tapered cannulated obturator was inserted along the guide wire (Fig. 3); the obturator was inserted gently into the epidural space; and a non-beveled round-shaped working cannula 8.0 mm in outer diameter was inserted into the epidural space along the obturator. Rotating the non-beveled cannula and endoscope allowed for 360 degree visualization of the annulus, and the exiting and traversing nerve roots. Forceps can be used so they open horizontally or vertically in the epidural space. Opening the forceps vertically and withdrawing them worked to retract the dura to explore the epidural space. During the procedure, the epidural space and the dura were readily exposed. The blue-stained disc was removed without facetectomy using a high frequency bipolar probe manufactured by Ellman (Ellman International, Inc., Hicksville, NY, USA) and endoscopic forceps. A mixture of triamcinolone acetate 40 mg and normal saline 8mL was injected to reduce postoperative nerve irritation via a working cannula. A sterile dressing was applied with a one point suture.
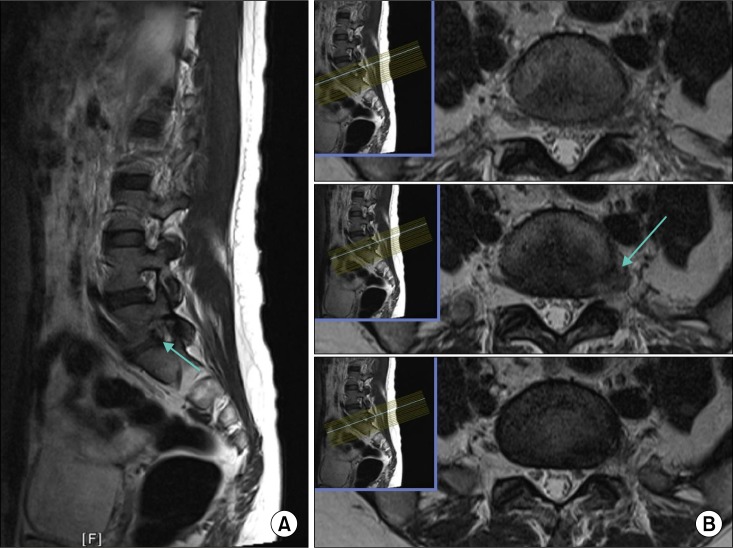
The patient's postoperative course was notable for 90% pain relief within 30 minutes after the operation. Her SLR test result showed immediate improvement of 80 degrees on the left side. Great toe dorsiflexion promptly improved to 4+/5 on the left side. An MRI obtained at one day postoperative showed improvement of the left L5 nerve compression and resolution of the disc fragment in the left extraforaminal zone (Fig. 4). At her 6-week, 3-month, and 6-month follow-ups, the patient continued to report complete pain relief and her ODI score continued to be 6. She showed residual dysesthesia at her 6-week and 3-month follow-ups, but it was not newly present, and it had diminished at the time of her 6-month follow-up. Left great toe and ankle dorsiflexion had recovered to a grade of 5/5 at the patient's 6-week follow-up.
Go to : 
DISCUSSION
The pathogenesis of FLDH is different from that of intraspinal central or paracentral disc herniations in terms of how they cause lumbar radicular pain. The latter could compress the dura and traversing nerve root, while the former could compress the exiting nerve root and dorsal root ganglion. Preoperatively, patients with FLDH experience more severe radicular leg pain and the frequent occurrence of sensory dysesthesia [4]. Furthermore, the sensory dysesthesia could be more remarkable than the motor deficit (75% versus 55%) due to the fact that the lesser injury of the ventral root produces lesser paresis of the muscle innervated by the motor neuron in the FLDH group. Postoperatively, the sensory dysesthesia has been found to be less improved and back pain more severe in FLDH patients [5]. However, the patient in our case had the foraminal upmigrated type of FLDH which could lead to greater injury of the ventral root, and she showed more prominent motor deficits than other patients with FLDH. This was the reason that we had planned a prompt surgical intervention, using either PELD or open surgery, without waiting several weeks for the response to conservative treatment.
Conventional posterior laminotomy and discectomy or microendoscopic discectomy (MED) [6] may not be a good surgical option for a FLDH due to a increase in postsurgical morbidity and related late complications such as recurrent back pain by a possible occurrence of iatrogenic instability and spondylolisthesis [7] after extended facetectomy or even complete resection of the pars. PELD, in contrast to open surgery or MED, is being performed under local anesthesia [89], in order to get direct feedback from the patient to deter any possible nerve damage during and after the procedure.
The PELD approach may be extremely difficult at this L5-S1 level, because the operative window narrows progressively due to the prominent iliac crest, wider disc space, and more oblique pedicles; and the more coronally oriented facet joints at L5-S1 impede posterior or posterolateral access to the disc [10]. In order to gain improved intraspinal access via a transforaminal approach at the level of L5-S1, foraminoplasty or facetectomy was often necessitated [111213]. Because of these anatomical complexities, the interlaminar approach has been acclaimed recently due to the provision of the largest interlaminar window, providing enough room for direct posterior access to the axillary or shoulder area of the S1 nerve root [14]. However, application of this interlaminar approach would be limited only to intraspinal disc herniations compromising the S1 nerve root.
Another paraspinal approach mimicking the conventional transforaminal access was chosen in the present case since the location of the ruptured disc was at the left extraforaminal zone with superior foraminal migration below the L5 pedicle. The skin entry point of paraspinal approach is medial and the angle to the skin is steeper compared with those of the common transforaminal PELD. The trajectory plan was based on the estimation from the preoperative axial MRI (Fig. 2) and X-ray.
The technique is similar to the "targeted fragmentectomy" described by Choi et al. [3]. The target was located in the epidural space, thus we performed a targeted fragmentectomy keeping the endoscope mobile in the epidural space instead of docking inside the disc space [1213].
There are few reports on PELD performance for lumbar disc herniation associated with a progressive motor deficit. The feasibility of the free-floating epiduroscopic technique as in the present case may justify the performance of PELD despite the patients' foot drop. However, PELD might be contraindicated for the intraspinal disc herniations which had led to the same foot drop because the root compression would be worsened by device's landing and irrigating pressure.
Most lumbar disc herniation patients with foot drop are treated with open surgery. However, if a proper trajectory of approach could be designed during the preoperative estimation, PELD, placing the endoscope in the anterior epidural space outside of the disc, can be used to treat.
Go to :
 XML Download
XML Download