

 PDF
PDF Citation
Citation Print
Print


LETTER TO EDITORS
Since ancient times, electrical sources were used for curing and rehabilitating numerous physical and mental ailments. Thereafter, in the modern scientific era, physical therapists started using electrical current to diagnose and treat various neuro-musculoskeletal dysfunctions [1]. Since then, researchers and biomedical experts have invented various types of electrical stimulators for physiotherapeutic purposes. Interestingly, physiotherapists around the globe are using electrode placement methods which are suggested by stimulator manuals without completely analysing their hypothetical reasons. Especially for muscle electrical stimulation, a cathode pole is placed over the motor points and an anode pole placed proximally to obtain stronger muscle contraction. Importantly, similar kinds of electrode placement methods have been used to treat the painful conditions even when the duration of the patho-physiology varied [2]. In my opinion, while treating chronic pain, clinicians have to give more importance to changes in the electrode placement methods rather than just changing the stimulation intensity and duration.
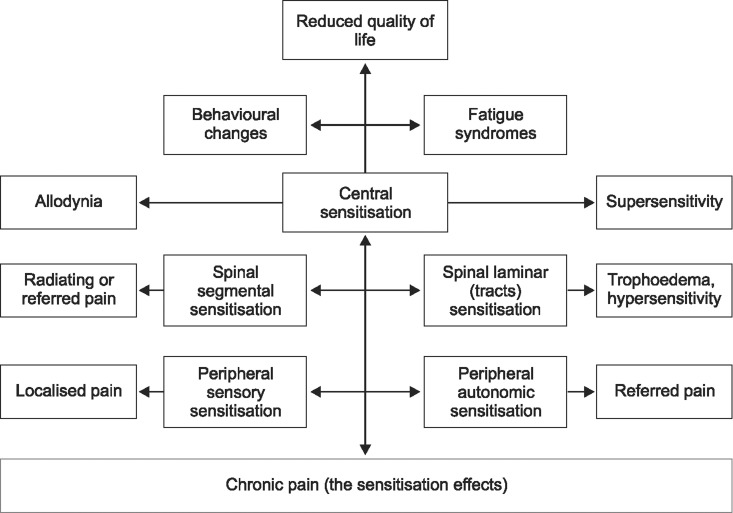
Chronic pain is a complex abnormal sensory phenomenon primarily caused by the sensitisation of neurons at the various levels of the nervous system which manifest features of the central patho-physiology more than the peripheral [34]. The functional and structural characteristics of neurons in the peripheral, spinal, laminar, and cortical level have been altered in most of patients with chronic pain [4]. The altered sensory relays along the ascending sensory pathways may produce localised and/or referred (peripheral sensitisation), radiating (spinal sensitisation), allodynic (laminar irritation), hyperalgesic (autonomic sensitisation) and other psychosomatic (central sensitisation) types of pain (Fig. 1). The combination of central and peripherally mediated manifestations of chronic pain can reduces the quality of life, which restricts the individuals' ability to take care of society and themselves [35]. So, it is important for us to treat central and peripheral phenomenon effectively by inverse electrode placement, because the conventional electrode placement primarily targets the peripheral neuromuscular system.
Inverse electrode placement is a modified method in which the cathode pole is placed over the spinal level and the anode pole is placed on the distal parts of limb to initiate the bidirectional flow of electrical impulses. This method may generate action potential at the spinal level first, and propagate bi-directionally; one towards the periphery and another towards the various parts of the central nervous system (Fig. 2). So, in order to achieve faster pain relief by desensitising the pain perception in all levels of the neural system, we can use this inverse electrode placement method to treat chronic pain syndromes.
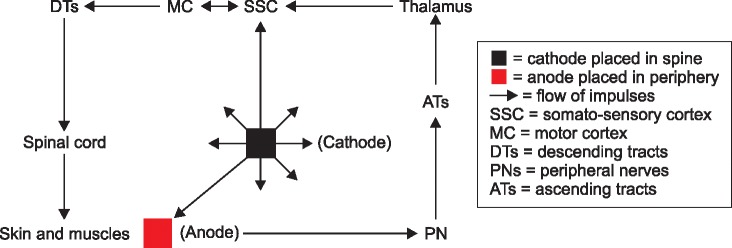
The generated action potentials under the cathode pole at the spinal level may stimulate local and adjacent spinal segmental sensory-motor and the autonomic neuronal pool. Subsequently, the centrally propagating action potentials can stimulate the axons of the ascending sensory tracts in the spinal cord and brainstem. Furthermore, the flow of ascending impulses may stimulate the higher cortical sensory-motor and associated perceptual neuronal areas. In the other direction, propagation of action potentials in the peripheral motor axons can stimulate the axon terminals and muscle fibers, especially at the level of reference electrode placement [6]. The enhanced sensory perception can possibly create more awareness and feedback regarding affected dermatomes and myotomes which may increase the efficacy of applied therapeutic currents.
Electrical stimulation with inverse electrode placement may work efficiently to reduce the sensitization of neurons of the central and peripheral nervous system, and increases the sensory perception in order to induce tissue healing.
1. Desensitization of spinal root hypersensitivity
It is evident that neuronal irritability at the spinal level reduces the muscle's flexibility which causes sustained mechanical loading over the facet joints, spinal nerve roots, and sympathetic ganglions. This excessive stress on the neural structures can be reduced by inducing the relaxation of the spinal segmental musculatures with the application of cathodal electrical impulses over the spinal level instead of peripheral areas [678].
2. Desensitization of ascending tract irritability
The placement of the cathode pole in the spinal level may increase interspinal-segmental sensory motor stimulation which may help in achieving multi-segmental therapeutic benefits. The machno-receptor stimulation under the cathode pole of the spinal level may modulate the transmission of pain impulses along the ascending sensory tracts. Further it may reduce the laminar irritability caused by lateral conduction of chronic pain impulses from the spinal as well as peripheral receptors [69].
3. Desensitisation of peripheral receptors
Stimulation of superficial and deep sensory receptors under the anode electrode at the periphery may induce enkephalin release and reflex relaxation. Sustained electrical stimulation may increase local blood circulation by reflex vasodilatation which reduces the accumulation of chemical irritants which cause the receptor sensitivity. The peripherally propagating motor neuron impulses from the spinal electrode may produce contraction of peripheral muscles under the anode pole which helps in movement re-education and proprioceptive biofeedback [89].
4. Perceptual healing of tissues
The somato-sensory perception induced by spinal and peripheral stimulation may activate the local healing process over the affected dermatomes and myotomes. The existing literature also suggests perception may play a major role in accelerating the healing process in the peripheral tissues. This central perception-induced tissue healing may modulate the central and peripheral hypersensitivity and improve the quality of life in patients with chronic pain syndromes [8910].
Go to : 
 XML Download
XML Download