

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The brachial plexus runs from the C5-T1 ventral rami, forms the superior, middle, and inferior trunks, divides under the clavicle, leads to the lateral, posterior, and medial cords, and finally forms the peripheral nerves running to the arms. The brachial plexus block is popular for anesthetic and pain control purposes in the upper limbs. There are a few approaches to the block, including the interscalene approach, supraclavicular approach, infraclavicular approach, and the axillary approach. The classic interscalene approach has been performed at the C6 level located in the cricoid cartilage and is useful in controlling pain after shoulder surgeries. However, this approach spares the lower trunk of the brachial plexus (C8-T1, ulnar nerve), thus it is not appropriate for some upper limb surgeries [1]. Some studies have reported findings regarding the efficacy of the interscalene brachial plexus block with approaches from lower regions in certain upper limb surgeries; however, there have been no studies that have reported this method being used with ultrasound. Therefore, the present study first divided the distance between C6 and the clavicle into three sections. Then we performed a low approach, ultrasound-guided interscalene brachial plexus block (LISB) on the interscalene groove that is located at a site about two-thirds of the distance caudally from C6 to examine the efficacy of the nerve and motor block at five and fifteen minutes after the block, and monitored for any signs of complications.
Go to : 
MATERIALS AND METHODS
The present study was conducted on twenty-eight patients who were classified as physical status 1 or 2 by the American Society of Anesthesiologists (ASA) and who were scheduled to receive an upper limb surgery at our hospital between May 2013 and April 2014. We excluded patients with coagulation disorders, those who were under the age of 18 or over the age of 75, those who weighed less than 50 kg or more than 100 kg, patients with any kind of neurological deficit, or patients with surgical site infections. After approval from the clinical research ethical review board at our hospital, we explained to the patients the objective of the study as well as potential risks and complications of the procedure. The study proceeded following consent from the patients (IRB number: 2013-02-013). The patients were not premedicated prior to receiving anesthesia. After they arrived in the operating room, patients were connected to a non-invasive blood pressure manometer, pulse oximeter, and electrocardiogram to monitor their vital signs every three minutes. The patients were in the supine position with their heads facing away from the side of the block. The region was prepped with betadine and the linear probe of the ultrasound (SonoSite M-Turbo, SonoSite, Inc., Bothell, WA, USA) was placed on the interscalene groove, which is located at about two-thirds of the distance caudally from C6 when the distance between C6 and the clavicle is divided into three sections, as suggested by Kim et al. [2] (Fig. 1). Sterilized plastic wrap and gels, and 22G, 50 mm needles (UniPlex NanoLine facet tip UP 3/50, Pajunk Medical Produkte GmbH, Geisingen, Germany) were used. With the help of a nerve stimulator (Stimuplex-S, B. Braun Melsungen AG, Melsungen, Germany) at 0.7 mA, the contraction of each muscle (pectoralis, deltoid, arm, forearm or hand) was confirmed (Fig. 2). For the local anesthetic, 40 ml of 1.5% lidocaine, including 1:200,000 epinephrine was used. At five and fifteen minutes after the injection of the local anesthetic, we confirmed the sensory block using alcohol wipes on the musculocutaneous nerve, median nerve, radial nerve, and ulnar nerve with a scale ranging from 0 (no sensation) to 10 (normal sensation) [2]. We also checked for muscular contractions by assessing flexion of the elbow (musculocutaneous nerve), extension of the elbow and wrist (radial nerve), pronation of the arm and flexion of the wrist (median nerve), and flexion and opposition of the fourth and fifth fingers toward the thumb (ulnar nerve), and considered signs of paralysis (loss of contraction) to indicate a successful motor block [3]. One anesthesiologist performed the LISB procedure and one orthopedist performed the surgery. We confirmed cases of hemidiaphragmatic paralysis after the surgery by performing a chest X-ray and consulting a radiologist regarding the results.


Go to :
RESULTS
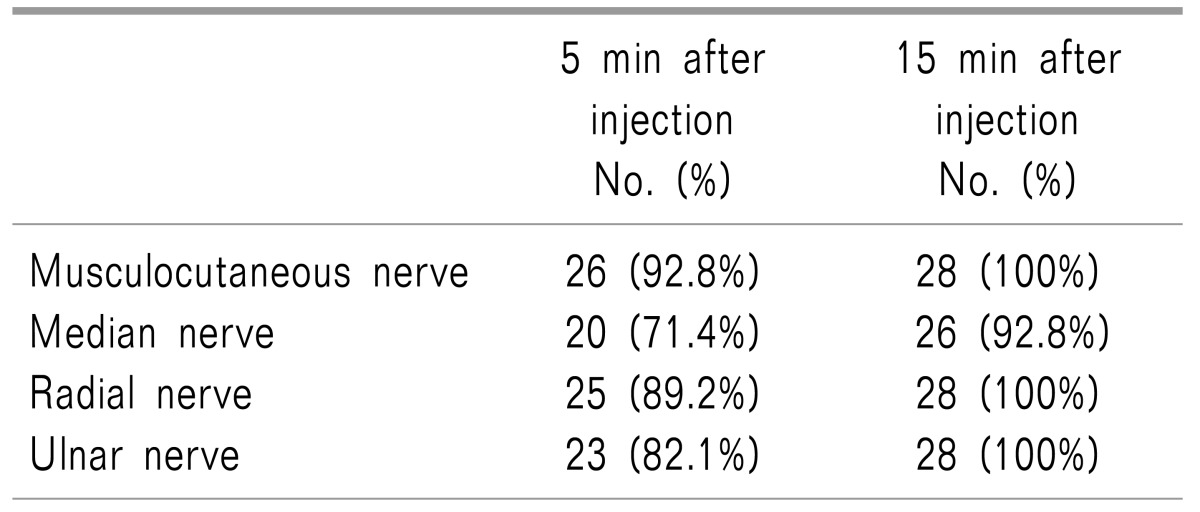
Among the 28 subjects of this study, 10 were male and 18 were female. The patients' demographic and clinical data including age, body weight, height, gender, surgery length, and type of surgery are illustrated in Tables 1 and 2. At five and fifteen minutes after the block procedure, the degree of sensory block in the ulnar nerve was found to be 2.8 ± 2.6 and 1.1 ± 1.8, respectively, on a scale of ten. Muscular block occurred in the median nerve after fifteen minutes in 26 of the 28 patients (92.8%), and in all of the other three nerves in all 28 patients (Tables 3 and 4). None of the patients received additional analgesics after the surgery, and there were no abnormalities during the surgeries. In addition, there were no signs of complications, such as dyspnea or Horner syndrome, during the surgery, in the recovery room, or in the wards (Table 5).
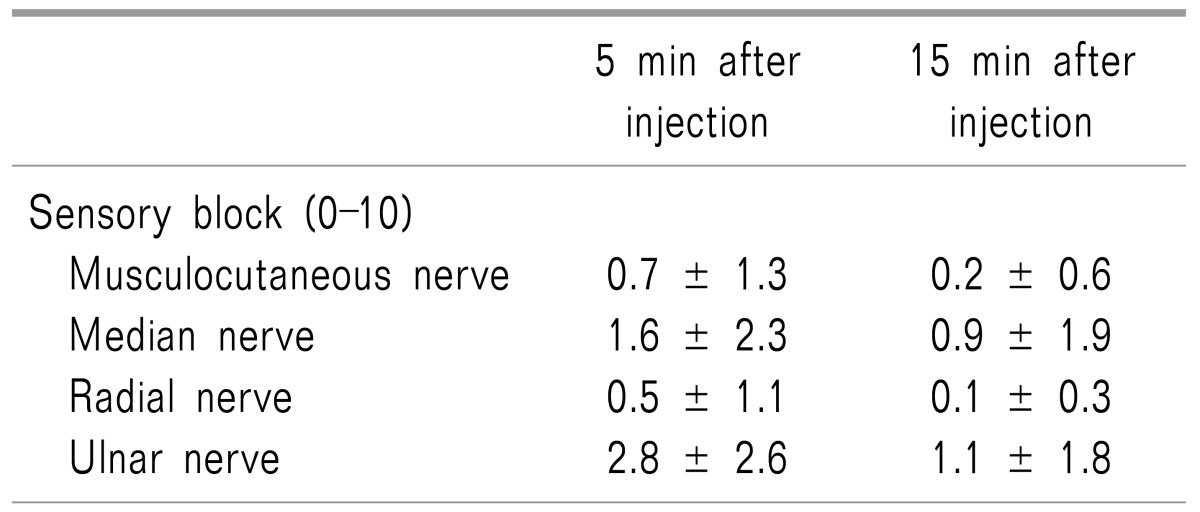
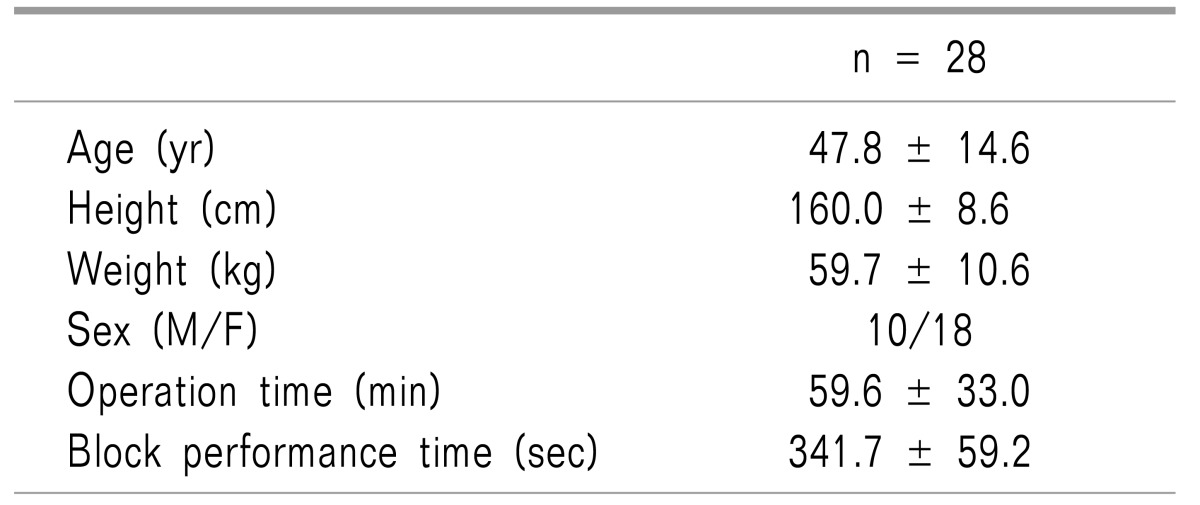
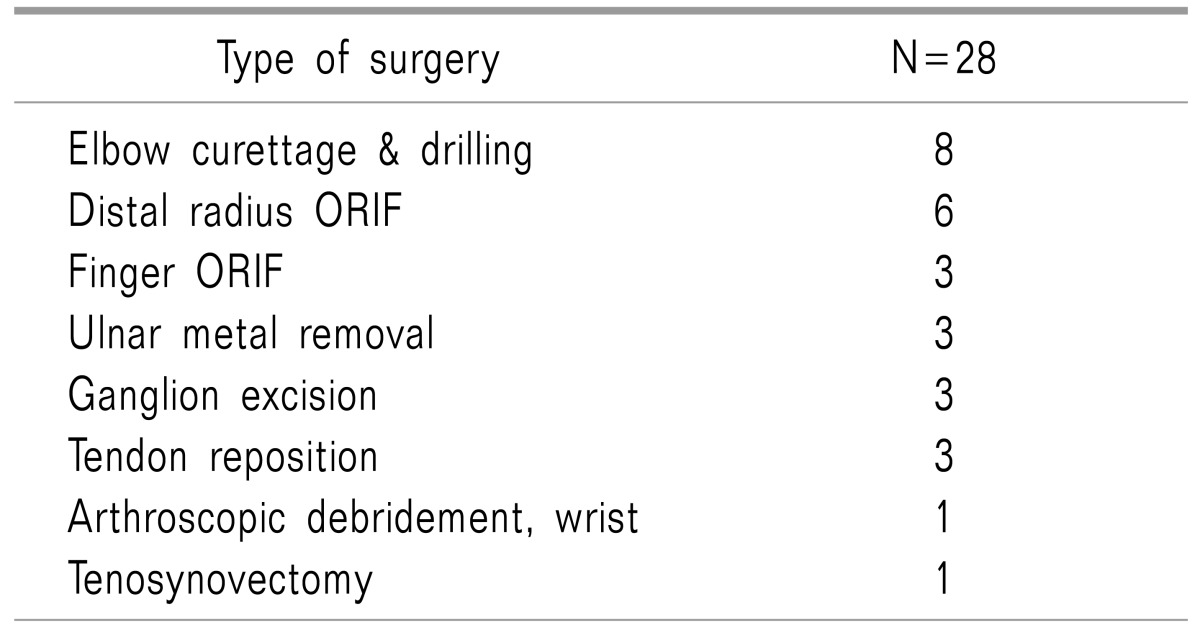
Table 3
Characteristics of the Sensory Block Using a Low Approach Interscalene Brachial Plexus Block
![]()
Go to :
DISCUSSION
This study confirmed that an appropriate sensory and motor block was achieved in the upper extremities, including the ulnar nerve, fifteen minutes after LISB, and that there were no complications associated with the block.
Two methods of LISB have been introduced, namely the anatomical landmark approach and the ultrasound-guided approach. There are three approaches to the anatomical landmark method: first, it can be performed in between the cricoid cartilage and the clavicle. Second, it can be performed 2 cm above the clavicle, and third, it can be performed on the interscalene groove, which is located at about two-thirds of the distance caudally from C6 after dividing the distance between C6 and the clavicle into three sections. There are two methods for the ultrasound-guided approach: first, it can be performed on the superior trunk where C5 and C6 are combined. Second, the injection can be performed on the caudal side of the C6 nerve root [245]. Although different studies define and name the procedures slightly differently (low approach, lower interscalene approach, or superior trunk approach), these procedures are identical in terms of using an approach through the lower regions of the C6 level compared to the existing ISB.
Owing to the advances in procedural techniques and the application of ultrasound technology, several studies have reported that the use of local anesthetics can be reduced when performing ISB. However, most of these studies limit their scope to shoulder surgeries, which are irrelevant to the block of the inferior trunk (C8-T1, ulnar nerve) [67,8]. It has been known that the ulnar nerve is not affected in about 30-50% of ISBs performed with the classic approach [1]. Furthermore, it has been reported that the ulnar nerve was not blocked in about 7-33.3% of the cases that took the classic approach ISB and used 30 ml of local anesthetics on the caudal side of the C6 nerve root [910]. Hence, in the present study, we used 40 ml of local anesthetics to ensure a quick onset and complete block of the ulnar nerve.
LISB is known to involve a short effect distance (from the C5 nerve root to the C8 nerve root) and to diffuse local anesthetics via the deep cervical fascia. In addition, LISB has been reported to bring about appropriate sensory and motor blocks required for upper limb surgeries even with a single injection [10]. Against this backdrop, the present study was planned and conducted.
Moreover, according to Plante et al., [9] who compared two groups of patients who were injected with local anesthetics either in the upper region of the C5 nerve root or the lower region of the C6 nerve root during an ultrasound-guided interscalene brachial plexus block for analgesia in arthroscopic shoulder surgeries, the group of patients who received local anesthetics in the lower region of the C6 nerve root had appropriate sensory blocks in all of the nerves; they reported that the sensory and motor blocks were especially noticeable in the ulnar nerve and that there was a rapid onset in the ulnar nerve. The results of this study showed that the sensory block in the ulnar nerve was 2.8 ± 2.6 on a 10-point scale at five minutes after LISB and 1.1 ± 1.8 at fifteen minutes after LISB. About 82.1% of motor neurons were blocked at five minutes, but 100% were blocked after fifteen minutes. In addition, there were no additional injections of analgesics during the surgery. Therefore, it can be said that the ulnar nerve was appropriately blocked via LISB.
Meanwhile, ISB is known to induce a temporary paralysis in the ipsilateral hemidiaphragm due to phrenic nerve palsy. The phrenic nerve is located within 2 mm of the brachial plexus of the cricoid cartilage and divides 3 mm per 1 cm as it descends caudally. Thus, it can be predicted that the incidence of phrenic nerve palsy-induced hemidiaphragmatic paralysis can be reduced if ISB is performed more caudal to the C6 level or on the superior trunk [1112]. In the present study, there were no signs of dyspnea or hemidiaphragmatic paralysis. In addition, LISB is known to reduce the damage to the dorsal scapular and long thoracic nerves, both of which split from the C5 nerve root [4]. Although we did not assess whether any such damages occurred in the present study, none of the patients experienced any such problems.
As mentioned above, there were no complications in the current study. We presume that we were able to reduce the risk of complications, such as vascular injection or nerve injury, by using an ultrasound nerve stimulator in addition to the inherent merits of the LISB method.
In the present study, the motor block in the median nerve was shown to be about 71.4% at five minutes after the procedure was performed. The block increased to 92.8% at fifteen minutes, and there were no additional analgesics injected and no additional block was performed. Other studies have also reported similarly slow blocks in the median nerve within fifteen minutes [9], which is thought to be due to the fact that the median nerve innervates all of C5, C6, C7, and T1.
There are a few limitations to this study. First, we did not have a large pool of subjects. Second, we could not observe the diffusion of local anesthetics through injecting contrast medium. Third, we did not compare the procedure of interest with other approaches. Thus far, studies on LISB are only in the form of case reports or brief reports; hence, in the future, LISB should be compared with other approaches, and cases of LISB using different doses of local anesthetics should be compared as well.
In conclusion, the present study confirmed that the nerves in the upper extremities, including the ulnar nerve, were appropriately blocked fifteen minutes after the performance of LISB, and that there were no complications induced by the block.
Go to :
 XML Download
XML Download