

 PDF
PDF Citation
Citation Print
Print


The 12th rib syndrome is a disease that causes pain in the upper abdomen and the lower chest, and its pathophysiology has not been clearly identified. However, it is assumed that the impingement on the intercostal nerves causes pain in the lower chest, upper abdomen, and flank [1]. The syndrome can be diagnosed using a patient's medical history and a simple physical examination, but without the full understanding of this syndrome, it can often go unnoticed. In this study, the authors provide a case-study of a 74-year-old female patient who was diagnosed with 9th rib syndrome, which is similar to 12th rib syndrome and a literature review.
CASE REPORT
A 74-year-old female patient visited a pain clinic, complaining of pain in her back, and left chest wall.
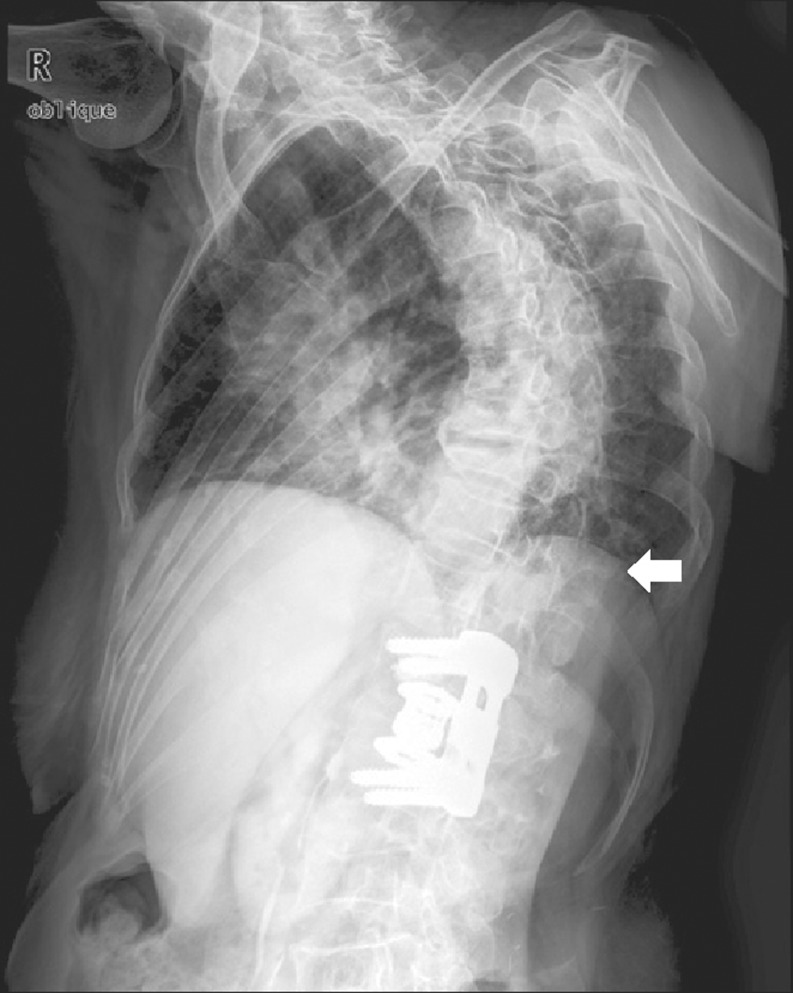
Six years earlier, the patient had a lateral fixation at T12, L1, and L2, due to a compression fracture at L1. Two years after this operation, the patient had osteoporotic compression fractures at T6 and T9. For the past three months, the patient had complained about pain at an NRS 7 on the left chest wall, which started without any serious trauma. After the patient was diagnosed in the neurosurgery department, with compression fractures at T8 and T9, she was scheduled to undergo vertebroplasty. On the physical examination, the patient stated that the left paraspinal muscles at the height of T8-T10 were tender when compressed, but did not have any percussion pain or facet joint tenderness. The patient did not complain of movement-associated pain (Fig. 1). When the spine was bent forward, the patient complained about a sharp pain in the left mid-axillary line and radiating pain toward the abdomen. However, the patient did not have any tenderness in her ribs, and the pain was not elicited when she took a deep breath or coughed. On palpation, the 10th rib was not felt, and the rib-cage image confirmed that the left 10th rib was severed (Fig. 2). We had determined that perhaps the 10th rib was severed during the last operation 6 years previous. When applying pressure to the 10th rib from the legs to the lower margin of the 9th rib of the patient (the Hooking maneuver), the pain was reproduced. Therefore, we assumed that the patient had 9th rib syndrome, similar to 12th rib syndrome, and ultrasound-guided 9th and 10th intercostal nerve blocks using 2 ml of 0.25% ropivacaine and 10 mg of triamcinolone were performed around the tips of the severed 10th rib. In addition, 2 ml of 0.25% ropivacaine and 10 ml of triamcinolone were administered into the muscles beneath the 9th rib at the point of the greatest tenderness. The patient's pain was reduced to 0-10 NRS 2. No additional procedures were performed, but the patient was instructed to avoid postures that could cause pain. The pain has not occured again up to date, and the patient is only receiving only the treatment for osteoporosis.

Go to : 
DISCUSSION
Cyriax reported in 1919 that pain could be caused by impingement on the intercostal nerves [2], and in 1922 it was named the slipping rib syndrome by Davies-Colley [3]. Depending on the locations of the impinged intercostal nerves and the authors writing about the syndrome, various names were used to refer to the syndrome, including 12th rib syndrome [45], slipping rib syndrome [3], rib tip syndrome [6], clicking rib syndrome [7], Cyriax's rib syndrome [8], and painful rib syndrome [9].
The mechanism that causes pain in the intercostal nerves is a hypermobile rib impinging on the intercostal nerve of the rib one level above due to the loosening of the costochondral cartilages of the lower rib [210]. Therefore, pain can be triggered or made more severe when patients perform lateral flexion and rotation of the trunk [10].
The prevalence of these syndromes is not widely known. Slipping rib syndrome is a common disorder, and shows a higher prevalence among women than men by a ratio of 3:1 [11]. While the 12th rib syndrome occurs more frequently among women than men by a ratio of 4:1 [12]. Scott et al. [9] conducted a study targeting 76 patients with painful rib syndrome. The mean age of the patients at presentation was 48 years, and the mean duration of pain at presentation was 32 months. Seventy percent were female. Forty-three percent of the subjects had pain in the left side, 45% had pain in the right side, 4% had pain in both sides, and 7% had pain in the xiphoid area. Among the entire study population, 43% said that they already underwent various tests, including barium meal, barium enema, endoscopy, ultrasound scanning, intravenous urography, and spinal radiology; some patients had laparotomy and non-curative cholecystectomy in combination with them [9].
If a patient tests positive using the hooking maneuver, the syndrome is suspected. If tender spots causing pain are felt upon palpation, and the pain can be relieved when intercostal nerve blocks are performed, this confirms the diagnosis of the syndrome [1]. Imaging tests such as CT, MRI, or bone scan do not offer much help, and if a differential diagnosis is deemed necessary, tests for biliary tract pathology, peptic ulceration, and urological pathology can be performed. Scott et al. [9] stated, "With firm reassurance and explanation, the pain either disappears usually within three months, or the patient learns to live with it as a minor nuisance. If the pain does not settle within three months it will become chronic in the vast majority". If a physician approaches patients without suspecting 12th rib syndromes, diagnosis will be delayed. So the patients' activities will be limited by pain, the patient may lead to depression and anxiety, due to prolonged pain without knowing the cause, and the patient may suffer financial burdens due to unnecessary medical tests.
The most important aspect of medical treatment is that physicians provide accurate information on diseases, give reassurance, and advise patients to refrain from physical activities, which may cause pain. If pain is not controlled by medication, an intercostal nerve block with local anesthetics and long-acting steroid infiltration to the tip of the affected rib can be performed. If the pain relief effect is not sustained, an intercostal nerve cryotherapy, costo-vertebral blocks, and a percutaneous dorsal root ganglion radiofrequency thermos-coagulation can be performed. If the pain is not controlled by the above procedures, a rib resection can be performed [1].
In this case-study, it is suspected that the patient had a partial resection of the left 10th rib in the past, and subsequent compression fractures at T8 and T9 led to the deformation of the rib cage (Fig. 3), causing the tip of the remaining 10th rib to impinge on the 9th intercostal nerves, causing pain.

Go to :
 XML Download
XML Download