

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Tramadol has become a familiar weak opioid analgesic using a µ-opioid receptor agonist and a serotonin and norepinephrine reuptake inhibitors mechanisms of action [1]. Acetaminophen added to the tramadol is also commonly prescribed to improve the efficacy of central analgesia. The mixture is unique in its action on the central nervous system (CNS), but is only effective in cases with no peripheral inflammatory reaction, in which cases non-steroidal anti-inflammatory drugs (NSAIDs) are preferable. However, tramadol has a significant abuse potential, an increased risk of convulsions of serotonin syndrome in chronic administration, as well as frequently causing initial dizziness, nausea, and somnolence [2].
Tapentadol, in a single molecule, is a novel analgesic with a dual mode of action as an agonist of the µ-opioid receptor (MOR), and as a norepinephrine reuptake inhibitor (NRI). Its analgesic merits begin quickly, at around 30 m for both acute nociceptive and chronic neuropathic pain [3]. The drug has a representative default, with the tablet containing both an MOR agonist and an NRI. This is similar to a mixture of salt and pepper making it difficult to season your food satisfactorily (Fig. 1).
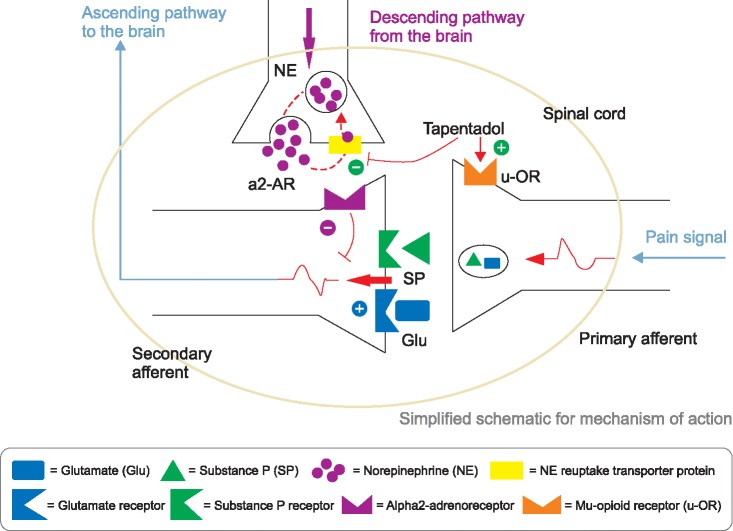 | Fig. 1A dual mode of action mechanism for tapentadol. (Modified from Tzschentke TM, Christoph T, Kögel B, Schiene K, Hennies HH, Englberger W, et al. (-)-(1R,2R)-3-(3-dimethylamino-1-ethyl-2-methyl-propyl)-phenol hydrochloride (tapentadol HCl): a novel mu-opioid receptor agonist/norepinephrine reuptake inhibitor with broad-spectrum analgesic properties. J Pharmacol Exp Ther 2007; 323: 265-76. Pertovaara A. Noradrenergic pain modulation. Prog Neurobiol 2006; 80: 53-83).
|
After the launch of tapentadol IR in United States, in June 2009, nonmedical diversion by college students was reported, using different administration routes and methods such as chewing and swallowing, as well as inhalation, instead of intact swallowing [4]. Some of the same authors, affiliated with the manufacturer, reported that the rates of tapentadol IR abuse and diversion were lower than those of oxycodone and hydrocodone, but similar to those of tramadol [5].
This review focuses on the pros and cons of dual analgesic mode and concern related to abuse/diversion, along with general drug information.
Go to : 
MAIN BODY
1. Brief history and clinical profile of tapentadol
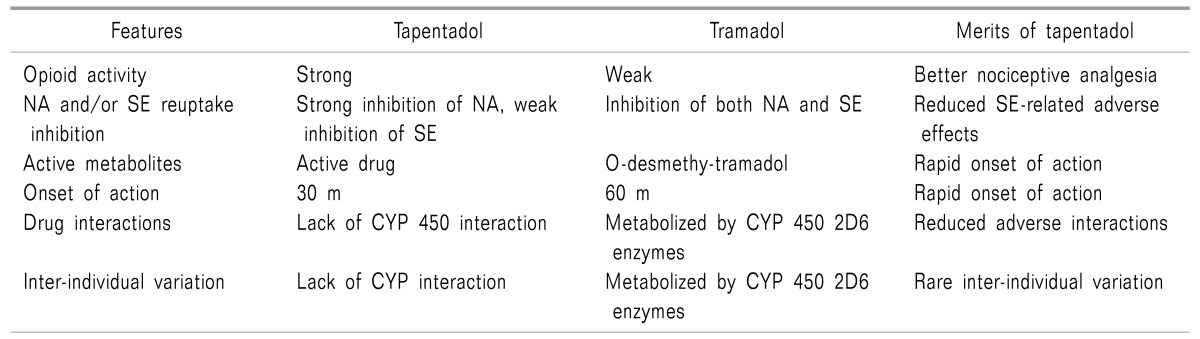
Tapentadol [(-)-(R, R)] was discovered in the late 1980s from morphine, tramadol, and a metabolite of tramadol [(-)-(S,S)-M-1] sequentially. The development of tapentadol from tramadol included these 4 steps: 1) opening of the cyclohexane ring; 2) changing from a prodrug to a direct acting drug; 3) selecting 1 enantiomer; and 4) replacement of the tertiary hydroxyl group (Table 1) [6].
Tapentadol hydrochloride IR was approved by the United States Food and Drug Administration (FDA) in 2008, for the treatment of moderate to severe acute pain [7]. Tapentadol ER also obtained FDA approval in the United States for management of moderate to severe chronic pain and neuropathic pain in 2011 and 2012, respectively.
Tapentadol binds to mu, delta, and kappa opiate receptors (Table 2) [7]. The smaller the inhibitory constant (Ki), the greater the binding affinity and the smaller amount of medication needed in order to inhibit the activity of the enzyme. It shows Ki values of 0.1 µM in a rat mu-opioid receptor binding assay and 0.5 µM in a rat synaptosomal norepinephrine reuptake assay [68]. In conclusion, the affinity of tapentadol for mu-opiate receptors is about 1/50 fold lower than that of morphine. In addition, tapentadol shows dose-dependent inhibition of norepinephrine reuptake, but only moderate increase in serotonin activity [79].

2. Various preparation and conversion of opioids
Currently available doses are 50, 75, and 100 mg of the IR form taken 4 to 6 times in a day and 50, 100, 150, 200, and 250 mg of the extended release (ER) form taken twice a day. Recommended maximal daily doses are 700 mg on the first day and 600 mg on subsequent days for IR, and 500 mg per day for ER formulations.
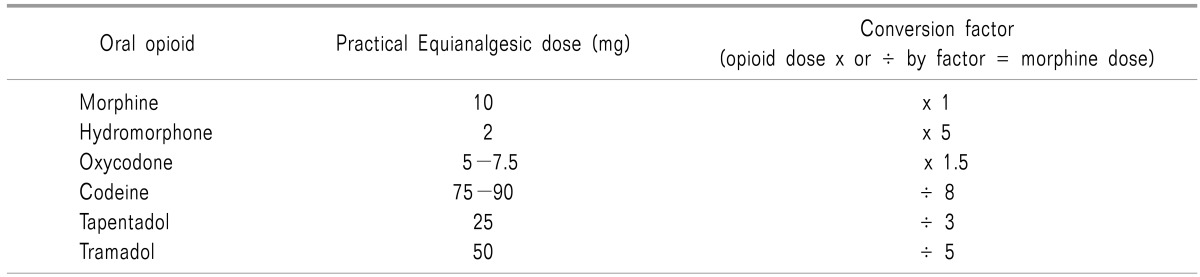
Fifty mg of tapentadol IR 4 times in a day can convert into100 mg of tapentadol ER twice a day. Based on 10 mg of oral morphine, an equianalgesic dose of oral tapentadol is 25 mg, compared to 5 mg of oxycodone. Twenty mg of oral morphine ER twice a day can be equivalent to 50 mg of tapentadol ER twice a day (Table 3).
3. Pharmacodynamics
Tapentadol has a dual mechanism of action: 1) inhibition of the ascending pain pathway related to agonists of MORs in the peripheral tissues, spinal cord, and brain; 2) potentiation of descending pain modulation related to NRI. It has 50 times less affinity to mu-opioid receptors than morphine; however, it is only 2-3 times less potent in its analgesic effect due to the NRI opioid-sparing effect [10].
In addition to primary tricyclic antidepressants (TCAs), the representative agents to potentiate inhibition of the descending pain pathway related to NRI and serotonin receptor inhibition. Nefopam acts as a triple neurotransmitter (norepinephrine, serotonin, and dopamine) reuptake inhibition [1112]. All these drugs, such as TCAs, tramadol [13], nefopam, and tapentadol, can be applied to neuropathic pain.
4. Pharmacokinetics
Absorption of tapentadol is rapid with a mean maximal serum concentration of 1.25-1.5 h after oral intake. It is present primarily in the form of conjugated metabolites, and excretes rapidly and completely up to 95% within 24 h and 99.9% within 5 d via the kidneys [1415]. Unlike tramadol, tapentadol is a single enantiomer with no active metabolites [16].
5. Contraindications
The absolute contraindications are impaired pulmonary function and paralytic ileus due to its opioid property, and concomitant use within 14 days of monoamine oxidase inhibitors (MAOI), due to its NRI property [15].
The safety and efficacy have not been established for use during pregnancy, labor, and delivery, or for nursing mothers, pediatric patients less than 18 years of age, and cases of severe renal impairment (creatinine clearance < 30 ml/m) and severe hepatic impairment (Child-Pugh score 10 to 15) [17].
6. Adverse events
The most common adverse events, reported by ≥ 10% in any immediate-release (IR) oral tablets were nausea, dizziness, vomiting, and somnolence. Constipation is less common than in users of oxycodone [18].
7. Abuse, diversion, and opioid doctor shopping
The risks of abuse and opioid doctor shopping were lower in the tapentadol immediate release than in the oxycodone immediate release group [1920]. However, these 2 studies were performed by pharmaceutical company, and it is difficult to ignore the relatively lower risk of abuse and shopping behavior.
The population-based rates of diversion were 0.03/100,000 for tapentadol IR and 0.001/100,000 for tapentadol ER compared to 1.495 for the other schedule II tablets, defined by the "United States Controlled Substances Act". Diversion rates based on drug availability were 0.03/1,000 (tapentadol IR), 0.016/1,000 (tapentadol ER), and 0.172/1,000 (other Schedule II opioid tablets) per prescriptions dispensed [21].
In another study for tapentadol abuse potential, prescription volume-adjusted relative risk for tapentadol ER was lowest compared to other comparatives, including fentanyl ER, tramadol ER, morphine ER, oxycodone ER, and oxymorphone ER, with the exception of hydromorphone ER. Tapentadol IR abuse prevalence was lower than all comparators except fentanyl IR [22].
The population-based rates and drug availability of the diversion of tapentadol ER were slightly lower than that of tapentadol IR, and much lower than those of other Schedule II opioid medications [21].
The endorsement ratio of recreational abusers for tapentadol was lower that of oxymorphone, but slightly higher than that of tramadol [23].
In summary, tapentadol shows a relatively lower risk for abuse, diversion, and opioid doctor shopping than those of the other opioids, but slightly higher than that of tramadol. Tamper-resistant technology may be a promising method to reduce diversion of tapentadol [24].
Go to :
CONCLUSIONS
Tapentadol has a unique synthetic opioid compound with an NRI property. It produces both acute nociceptive and chronic neuropathic analgesia. However, it is present primarily in the form of conjugated metabolites after glucuronidation, and excretes rapidly and completely via the kidneys.
The most common adverse reactions are nausea, dizziness, vomiting, and somnolence. Precautions against concomitant use of central nervous system depressants, or use of tapentadol within 14 days of the cessation of monoamine oxidase inhibitors, are advised.
The major concerns for tapentadol are abuse, addiction, seeking behavior, withdrawal, and physical dependence. The presumed problem for use of tapentadol is to control the ratio of MOR agonist and NRI.
In conclusion, tapentadol produces both nociceptive and neuropathic pain relief, but with worries about abuse and dependence.
Go to :
 XML Download
XML Download