

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Neuropathic pain, which can be caused by nerve irritation, damage, or destruction of the nervous system, is one of the six classes of chronic pain. It may be associated with abnormal sensations (dysesthesia), an exaggerated pain sensation (hyperalgesia), and pain produced by normally non-painful stimuli (allodynia). The mechanism of neuropathic pain is not yet fully understood, and it is believed that a central or peripheral mechanism may be involved. Neuropathic pain is usually unresponsive to normal drug therapy, and there is a limited range of treatment available to patients [1,2].
Glutamate (glu) is the main neurotransmitter present in the terminals of afferent neurons specialized in pain transmission. The activity of glutaminergic neurons in the spinal cord is greatly increased by inflammation and neuropathic pain conditions. Exaggerated glu activity through NMDA receptors is responsible for central sensitization [3,4].
It has been reported that the transplantation of the adrenal medullary gland into the subarachnoid space is accompanied by reduced pain-related behaviors in neuropathic animals [5,6]. Catecholamines are the main products secreted by the adrenal medulla. It has been shown that the injection of α- adrenergic antagonists after transplantation of the adrenal medulla does not eliminate the analgesic effect of the transplant in the chronic phase of a formalin test. It has therefore been suggested that other factors secreted by this tissue play a role in the analgesic effect [6].
Histogranin with anti-NMDA activity is a peptide extracted from the chromaffin cells of the adrenal medulla. Histogranin is responsible for the partial analgesic effects of adrenal medullary transplantation in the spinal cord of neuropathic rats [6,7]. Several recent studies have reported a much higher efficacy from a precise multi-target combination therapy than from mono-therapy for the management of neuropathic pain [3,8,9]. A considerable advantage of using combination therapy is that the active ingredients act on different molecular targets, which enables them to act on more of the signaling cascades involved in pain. Another major benefit of combination therapies is that they reduce the development of drug resistance. The main aim of this study was to investigate the analgesic effect of histogranin and noradrenaline in reducing neuropathic pain.
Go to : 
MATERIALS AND METHODS
Male Sprague-Dawley rats (250-300 g) were housed in separate cages with free access to food and water, and were exposed to light and dark cycles of 12:12 hours. All the procedures were approved by the institutional animal ethics committee.
1. Surgeries
To induce chronic constriction injury (CCI) of the sciatic nerve, the animals were anaesthetized with a mixture of intraperitoneal ketamine and xylasin (80 mg/kg and 10 mg/kg, respectively) and the skin of their left hind paw was cleaned with 70% alcohol. The sciatic nerve was exposed at the mid-thigh portion, and was isolated from the surrounding tissue. Four loose ligatures of the 4-0 chromic gut were tied around the sciatic nerve, one millimeter apart on the proximal part of the trifurcation. The wound was immediately closed with silk sutures, and a topical antibiotic was applied on top of the wound. One week after the surgery, the animals' Basso-Beattie-Bresnahan (BBB) scores were assessed to confirm the CCI model induction. The rats with a BBB score over 2 points were excluded (the success rate was 96.3%). After confirmation of the CCI induction, for cannulation, the animals were anaesthetized with the same anesthetic mixture. Their heads were fixed in a stereotaxic device and their hair was removed at the junction of the scalp and the first spinal vertebra. A 7.5 cm PE 10 tube (Braintree Scientific, INC. Braintree, MA, USA) was carefully placed through a puncture in the middle of the atlanto-occipital membrane to the lumbar level of the spinal cord, and the wound was closed and treated with a topical antibiotic ointment. The rats were returned to their cages and were left to recover for 3 days. On the day of the drug injection, the forelimbs and hind limbs were monitored to check the motor deficits. The animals displaying neurological deficits were excluded from further studies and were euthanized. The motor dysfunction and pain threshold was assessed 10 days after the surgery.
2. Behavioral assessment
An acetone test was used for the evaluation of cold allodynia. The rats were placed in a transparent plastic cage on a metal mesh surface for a habituation period of 20 min. A drop of acetone was then squirted onto the mi-plantar surface of their hind paws. Brisk withdrawal, licking, or biting of the hind paw was defined as a positive response. The test was repeated 5 times at 5 min intervals. The frequency of the foot withdrawal was expressed as a percentage: (number of trials accompanied by brisk foot withdrawal) × 100 / (number of total trials).
For evaluation of the thermal pain, a paw immersion test was used. The hind paws of the animals were carefully dried and immersed in a cup of freshly filled water at a temperature of exactly 44℃. The withdrawal time, i.e., the time between the immersion of the hind paw in the hot water and the withdrawal reaction, was recorded. A cut-off time of 20 sec was considered. The test was repeated twice, and the average withdrawal time was evaluated as the withdrawal latency.
The motor reflexes were evaluated through grasping and placing reflexes. For the evaluation of the grasping reflex, a horizontal stainless steel surface containing several bars measuring 2 mm in diameter and placed 1 cm apart was used. The rats were restrained with towels and were kept close to the surface, so that their hind paws touched the bars. The tonic grasp of the rats' hind paws was tested. The trial was repeated 5 times, and the number of positive grasping responses was recorded.
For evaluation of the placing reflex, the rats were restrained with a towel and were kept close to the edge of a table, so that their hind paws were located slightly beneath the surface of the table. In the case of a positive placing reflex, the animal put the hind paw on top of the table. The experimenter recorded whether reflexive placing of the hind paws on the table surface occurred. The experiment was repeated 5 times, and the number of positive responses was recorded.
3. Experimental design
Ten groups of rats (80 rats in total) were used to examine the analgesic effects of the administrated drugs. Four groups received intrathecal injections of different doses (0.5 and 1 microgram) of noradrenaline and serine histogranin (SHG). Four different groups of animals received simultaneous injections of both drugs to investigate the effect of combination therapy. One group remained intact (control group), and another group received normal saline as a vehicle. The behavioral assessment was conducted (pre-injection) ten days after the induction of the nerve injury (3 days after cannulation), when the level of the pain was maximal, and the drugs were then injected intrathecally.
Fifteen minutes after the drug injection, the animals underwent a behavioral test (post-injection). The sequencing of the behavioral test was the same for all experimental groups, and the same individual, who was blind to the treatment, administered the drugs and tested the animals. Eight animals were used in each group.
4. Drugs
Noradrenaline was purchased from the Sigma-Aldrich Company and SHG was purchased from Bachem, Torrance, CA. All drugs were dissolved and diluted in saline, and were injected in a volume of 10 µl. The catheter was then flushed with 10 µl of sterile saline. In the vehicle group, 20 µl of normal saline were injected. In the groups receiving injections of both drugs, noradrenalin was injected immediately after injection of the SHG.
In order to investigate the additive or synergistic effect of noradrenaline and SHG, the effectiveness of each drug alone and in combination was determined by subtracting the post-injection values from the pre-injection values. To assess the theoretical additive effect of the two drugs, the values obtained from the subtraction for the groups receiving noradrenaline or SHG alone were summated. To evaluate the synergistic effect, the theoretical values of the additive effect were compared with the experimental values when administrated in combination.
5. Statistical analysis
All the data were presented as mean ± SEM. The statistical analyses were performed using the SPSS software (version 16). A paired sample t-test was used to compare the variables between the groups, and an independent sample t-test was used to determine the synergistic effect. A P value < 0.05 was considered significant.
Go to :
RESULTS
1. Effect of SHG and noradrenaline alone or in combination on the acetone test
The injury of the sciatic nerve significantly increased the response to acetone droplets (P < 0.01). The administration of 1 µg of noradrenaline, but not of 0.5 µg, significantly increased the percentage of response to the acetone drops (P < 0.01). Both doses of SHG significantly alleviated the allodynic response to the acetone droplets (P < 0.05 for 0.5 µg and P < 0.001 for 1 µg). No significant difference between the pre- and post-injection values was observed in the vehicle group (P = 0.4) (Fig. 1A). The combination therapy in all doses effectively decreased the cold allodynia induced by the acetone drops. The combination of noradrenaline and SHG in all doses brought about a significant increase in the percentage of responses (P < 0.01) (Fig. 1B). Fig. 1C shows the comparison between the theoretical effectiveness and the effectiveness of the combination therapy. A significant difference was observed between the co-administration of 1 µg of noradrenaline with 1 µg of SHG and the theoretical effectiveness. In the case of simultaneous administration, the percentage of response to the acetone test was significantly lower than the theoretical effectiveness (P < 0.01) (Fig. 1C).
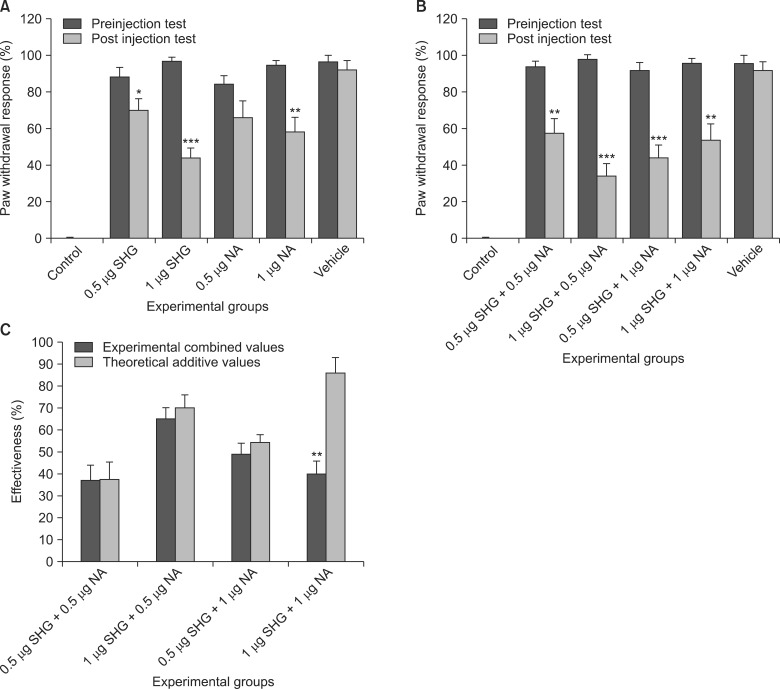 | Fig. 1Percentage of withdrawal response to the acetone drops in the drug-treated CCI groups, vehicle-treated CCI group, and control animals (A, B). The comparison between the theoretical effectiveness and the effectiveness of the experimental combination therapy is shown in (C). The combination therapy decreased the effectiveness of the treatment. The results are expressed as the mean ± SEM of the 8 animals in each group. *P < 0.05, **P < 0.01, ***P < 0.001; NA: noradrenaline, SHG: serine histogranin.
|
2. Effect of SHG and noradrenaline alone or in combination on the withdrawal latencies from the 44℃ water
The injury of the sciatic nerve significantly decreased the paw withdrawal latency response to the 44℃ water (P < 0.001). When administrated alone, both doses of SHG (P < 0.05) and 1 µg of noradrenaline (P < 0.05) significantly increased the withdrawal latency. The injection of 0.5 µg of noradrenaline had no significant effect (P = 0.19). The vehicle injection did not change the withdrawal response (P = 0.71) (Fig. 2A). In the groups receiving 1 µg SHG + 0.5 µg noradrenaline (P < 0.01) and 0.5 µg SHG + 1 µg noradrenaline (P < 0.05), a significant increase in the withdrawal latency was observed. In the animals that received 0.5 µg of noradrenaline + 0.5 µg of SHG (P = 0.94) and 1 µg of noradrenaline + 1 µg of SHG (P = 0.11), no significant difference was observed between the preand post-injection values (Fig. 2B). However, in the comparison between the theoretical effectiveness and the effectiveness of the combination therapy, a significant difference was observed in the groups that had received 0.5 µg of noradrenaline + 0.5 µg of SHG (P < 0.05) and 1 µg of noradrenaline + 1 µg of SHG (P < 0.05) (Fig. 2C).
 | Fig. 2Withdrawal latencies in response to the 44℃ water in the drug-treated CCI groups, vehicle-treated CCI group, and control animals (A, B). The comparison between the theoretical effectiveness and the effectiveness of the experimental combination therapy is shown in (C). The effectiveness was significantly reduced in the case of combination therapy with equal doses. The results are expressed as the mean ± SEM of the 8 animals in each group. *P < 0.05, **P < 0.01; NA: noradrenaline, SHG: serine histogranin.
|
3. Effect of SHG and noradrenaline alone or in combination on the motor reflexes
The chronic constriction of the sciatic nerve significantly blocked the animals' grasping and placing reflexes, and a significant reduction of those reflexes was observed on the second week following CCI (P < 0.001). The injection of vehicle, noradrenaline, or SHG alone or in combination did not improve the reflexes (P > 0.05), and no significant difference was observed in the number of grasping and placing reflexes between the pre- and post-injection of the drugs (P > 0.05) (Fig. 3). In the comparison between the theoretical effectiveness and the effectiveness of the combination therapy, no significant difference was observed (P > 0.05) (not shown).
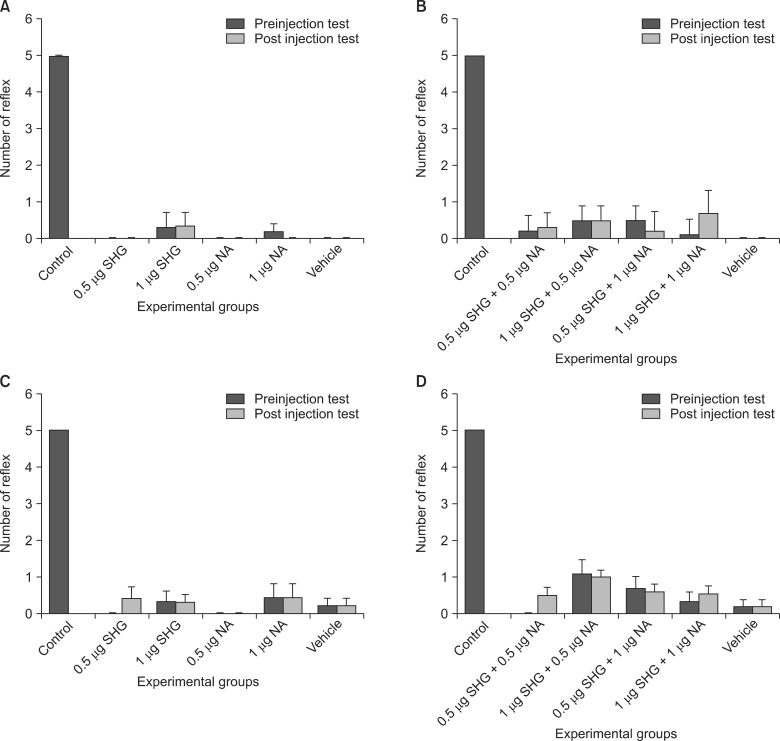 | Fig. 3Changes in the number of positive grasping (A, B) and placing reflexes (C, D) after intrathecal injection of noradrenaline (NA) or serine histogranin (SHG), alone or in combination, in the different experimental groups. The drug therapy did not improve the motor reflexes. The results are expressed as the mean ± SEM of the 8 animals in each group.
|
Go to :
DISCUSSION
Noradrenaline and SHG are two substances secreted by the adrenal medulla. The results of the present study show that both compounds can block the maintenance of CCI-induced allodynia. Moreover, the results of this study confirm that loose constriction of the sciatic nerve produces motor and sensory disorders in the affected limb(s). The grasping and placing reflexes disappeared following sciatic nerve injury, and the injection of SHG or noradrenaline alone or in combination did not enable recovery of the reflexes. The key finding of the present study is that the simultaneous administration of SHG and noradrenaline does not have a synergistic effect in increasing the pain threshold. This was made clear by the two compounds administrated in equal concentrations in the CCI model. The data show that in equal doses, noradrenaline and SHG have a sub-additive effect or antagonize one another's effect (Fig. 2C).
Histogranin has been shown to have anti-NMDA activity. NMDA antagonists have an analgesic effect in acute and chronic pain models and can augment opioid analgesia and reduce the development of tolerance to opioids [10]. It is known that the intrathecal injection of SHG, the stable analog of SHG, in a concentration of 1 microgram attenuates the hyperalgesia and allodynia resulting from chronic constriction injury of the sciatic nerve in rats. The administration of 2 and 4 micrograms of SHG has a lower analgesic effect in the CCI model [7]. This means that higher doses of SHG are not substantially more potent than lower doses in the neuropathic pain model, which indicates a dual role (agonist -antagonist) of the peptide.
The noradrenaline transporter in the spinal cord increases at the lumbar level of the spinal cord after a nerve injury [11], which shows that the level of noradrenaline in the lumbar level decreases following nerve injury. Therefore, it seems that the decrease in the content of noradrenaline in the spinal cord in the neuropathic pain condition is one of the main mechanisms in the pathophysiology of neuropathic pain [12]. Chronic nerve injury produces neuropathic pain by increasing the excitability of the dorsal horn neuron of the spinal cord, and this excitability can be reduced by an alpha 2 receptor agonist [13].
There has been growing interest in using drug combination therapy for the alleviation of chronic pain [3,4,8,9]. The effect of the two drugs in combination could be super additive or synergistic if the results of their actions were higher than the results expected from their individual potencies and efficacies. In contrast to synergism, some drugs may act antagonistically when their simultaneous administration shows subadditivity [14,15]. Among antinociceptive drugs, NMDA antagonists have been the main center of attention for the treatment of neuropathic pain. However, due to their side effects when administrated alone and in effective doses, they are not the first choice for the treatment of neuropathic pain syndromes.
It has been reported that the burning pain and allodynia observed in complex regional pain syndrome could be treated with the administration of an alpha 2 agonist, dexmedetomidine, and an NMDA antagonist such as ketamine. No side effects have been reported for this combination therapy [16]. Adrenergic receptor agonists respectively activate and inhibit K+ channels and voltage-dependent Ca++ channels, and alter the firing rates of neurons [17]. From the results obtained in this study, it appears that the single administration of noradrenaline or SHG can be sufficiently effective to block nociception, with no adverse effects. It seems that when administrated in combination, SHG and noradrenaline do not show a superadditive effect in the chronic constriction model of the sciatic nerve. The mechanism of the interaction between the adrenergic system and the NMDA receptors remains to be elucidated. The changes in the pharmacokinetics of each drug may be caused by their co-administration. For example, noradrenaline may induce vasoconstriction and decrease the spinal blood flow, thereby influencing the pharmacokinetics of other drugs [18]. A second possibility is that the two substances act on the same site. Subadditive interaction usually occurs when two compounds have affinity for one receptor and affect different critical points along a common pathway. The third possibility is that one compound affects the release of the other. Glutamate receptors, which are located presynaptically, generally mediate the control of neurotransmitter release [19]. The release-enhancing glutamate receptors are isolated from the noradrenergic nerve terminals [20]. The mutual interactions between glutamate receptors and NMDA receptors have been investigated by several researchers [21,22]. Presynaptic NMDA receptors have been found on the neocortical noradrenergic nerve terminals of rats and humans [23]. Therefore, it seems likely that presynaptic NMDA receptors and metabotropic glutamate receptors interact to modulate the noradrenaline release from noradrenergic terminals. Luccini et al. showed that NMDA receptors enhance noradrenaline release when in combination with metabotropic glutamate receptors [22]. The authors' results demonstrated that in a Mg2+ free solution, NMDA agonists directly act on the noradrenergic axon terminals at the level of the presynaptic NMDA receptors, and enhance the release of noradrenaline. According to the results of the present study, it is likely that SHG prevented or decreased the secretion of noradrenaline by the nerve terminals, an effect mediated by presynaptic NMDA receptor inhibition. There seems to be a mutual relation between the NMDA receptors and the adrenergic receptors. It has been reported that exogenous alpha agonists have a neuroprotective effect in retinal excitotoxicity models. Alpha 2 receptors located postsynaptically are able to modulate the NMDA receptor function. This mechanism is responsible for the neuroprotective effect of exogenous alpha 2 agonists [24].
With regard to the interactions of the adrenergic and NMDAergic systems, Nishiyama et al. reported a synergistic effect on the pain threshold from an alpha adrenergic agonist and an NMDA antagonist, going against the results of this study. In Nishiyama et al., clonidine was used as the alpha 2 adrenergic receptor agonist, and AP-5 as the NMDA receptor antagonist [25]. In addition, in two previous studies, Horvath et al. showed that ketamine and S(+)-ketamine, but not R(-)-ketamine (an NMDA antagonist), exhibited a similar effectiveness in potentiating the antinociceptive effects of dexmedetomidine (an α2-adrenoceptor agonist) [26,27]. As NMDA receptors have multiple agonist binding sites on the various NMDA receptor subunits, using different substances may exert different effects. Moreover, the types of behavioral tests used in the experiments may explain the differences in the results between the two studies. In Horvath et al.'s study, a tail flick and formalin test was used for the behavioral evaluation. This is the most traditional test of nociception and is based on stimulus intensity. The tail flick test evaluates phasic, short-lasting pain behavior, and is therefore unsuitable for the evaluation of tonic or chronic pain, which are modulated differently in the central nervous system. The pain induced by formalin injections is a more temporary kind of tonic pain, which presents a distinct mechanism from chronic pain.
In conclusion, the intrathecal administration of noradrenaline or SHG as an adrenergic receptor agonist and an NMDA receptor antagonist, respectively, increases the pain threshold in the neuropathic pain model induced by chronic constriction injury of the sciatic nerve. The simultaneous administration of both compounds however does not produce synergistic analgesia, and no effect has been observed on motor behavior. These results suggest that combination therapy using adrenergic and NMDAergic systems may not be a good approach to the treatment of chronic neuropathic pain syndrome.
Go to :
 XML Download
XML Download