

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Although minimally invasive ASS is commonly performed, the procedure is associated with severe postoperative pain [1,2]. Therefore, appropriate pain control methods in the early postoperative period can improve rehabilitation and recovery [2]. The opioid requirements for this pain are known to be similar to those following gastrectomy or thoracotomy [3]. While the administration of parental opioids is considered for severe postoperative pain control, the use of opioids can lead to complications including nausea, vomiting, pruritus, ileus, confusion, urinary retention, hypotension, and respiratory depression [4].
Therefore, nerve block procedures for shoulder surgeries have been studied. The ISB is regarded as an effective analgesic method for ASS. Previous studies have reported that ISB is excellent due to both its pain control and morphine-sparing effects in the first 24 hours following surgery, compared to either a suprascapular nerve block or a single injection of a local anesthetic especially in shoulder surgeries. In addition, more effective postoperative pain control is achieved through a combination of ISB and local analgesic injection [2,3,5]. An intra-articular injection (IA) is performed by the surgeon at the end of surgery just before wound closure. With the use of IA, additional procedures for pain control are not needed by patients and the procedure is as effective as an ISB [3]. Also, a continuous cervical epidural block (CCE) is known to provide excellent pain relief for patients undergoing upper extremity surgery. Epidural analgesia with a local anesthetic, an opioid or both is regarded as the treatment of choice for postoperative pain control in various surgeries (e.g., total knee arthroplasty, thoracotomy). However, a cervical epidural catheter is not commonly used and is in fact rarely utilized in shoulder operations [6]. Despite the severe pain associated with arthroscopic shoulder surgery, comparisons between a neuraxial block such as CCE and other analgesic methods such as ISB and IA are very rare. Therefore, the aim of this study is to compare postoperative pain control in an ISB group compared to that in CCE and IA groups.
Go to : 
MATERIALS AND METHODS
1. Patients
The study protocol was approved by the ethics committee of the Jeju National University Hospital and was registered as a clinical trial (2012-04-002-004). The study was carried out according to the principle of the Declaration of Helsinki 2000, and written informed consent was obtained from all participants before their inclusion in the trial. Between May of 2012 and April of 2013, a total of 57 consecutive patients undergoing elective ASS under general anesthesia at our hospital were enrolled. The exclusion criteria were allergy to any medication in this study, a history of hypertensive disease, a grade of an American Society of Anesthesiologists (ASA) class exceeding II, and an inability to understand the instructions concerning the study. All operations were performed by a single surgeon who used an arthroscopic repair technique. All patients were recruited into this prospective randomized study and randomized into one of three groups using a simple randomization technique : 1) ISB group; n = 19; 2) CCE group; n = 19; and 3) IA group; n = 19
1) ISB group
Patients in the ISB group received the block before the induction of general anesthesia in the operating room. After supine positioning with head rotation to the other side, ISB was performed with ultrasound and nerve stimulation. The brachial plexus was identified using a nerve stimulator (Stimuplex-S, B. Braun Melsungen AG, Melsungen, Germany) connected to the proximal end of the metal inner needle of a plastic cannula (Stimuplex-A, 25-G B. Braun Melsungen). The initial current output of the nerve stimulator was 0.7 mA. A linear high frequency 6-13 MHz ultrasound probe (Sonosite M-turbo, SonoSite, Inc., Bothell, WA, USA) was used. Upon contraction of the triceps muscle, the C5-6 nerve root or superior trunk was found, and 10 ml of 0.25% ropivacaine with 200 mcg of epinephrine was injected. Twelve hours after the operation, a fentanyl patch (12 mcg/hr) was applied to the patients.
2) CCE group
The procedure was performed one day prior to the surgery. After prone positioning of patients and sterile preparation, local anesthetics were injected at the insertion site. A 17 gauge Tuohy needle was inserted under fluoroscopic guidance at the C7-T1 interspace. After identification of the epidural space using the loss of resistance technique, an epidural catheter (Epidural Catheterization Set, 19-G, Arrow International, Inc., Asheboro, NC, USA) was inserted. The catheter reached the C4 or C5 epidural space on the ipsilateral side of the affected limb. Following confirmation of the catheter position with contrast medium, the catheter was sutured in place with naylon 3.0.
After the patients were transferred to the operating room, a 10 ml bolus of 0.25% ropivacaine was injected through the epidural catheter, after which an epidural PCA (patient controlled analgesia) infusion pump (ropivacaine 0.25%, total 250 ml, basal 3 ml, bolus 3 ml, lockout time 30 min) was connected to the epidural catheter prior to the induction of general anesthesia. The catheter was removed 48 hours after the completion of the surgery.
3) IA group
After the completion of the arthroscopic procedure, the surgeon inserted a catheter into the joint via an arthroscopy portal. The catheter was attached to a disposable PCA infusion pump (Accufuser®, Wooyoung Medical Co., Ltd., Chungcheongbuk-Do, Korea) containing 100 ml of 0.25% ropivacaine, with a continuous basal infusion of 2 ml/hour with patient-controlled boluses available at 4 ml/hour. The catheter was removed 48 hours after the completion of the surgery.
2. General anesthesia technique
General anesthesia was induced by the IV administration of thiopental (5 mg/kg) after manual ventilation with O2 at 6 L/min. Orotracheal intubation was facilitated with rocuronium (1 mg/kg). Anesthesia was maintained with O2 and N2O each at 1 L/min, and sevoflurane was maintained at a minimum of 1.0 vol%. A non-invasive blood pressure, electrocardiography, pulse oximetry and BIS values were monitored continuously. No additional intravenous analgesics including opioids were injected. After the completion of the surgery, glycopyrrolate and neostigmine were intravenously administered and the patients were extubated. The procedures were performed by one of the two co-authors of the study.
3. The studied variables
The primary outcome measure was the numerical rating scale (NRS) and rescue opioid dosages (ROD) during the first 48 hours postoperative. The severity of postoperative pain was evaluated by pain at rest and on movement and was assessed 30 minutes, 4 hours, 24 hours, and 48 hours after the operation with the NRS, with scores ranging from 0 = no pain to 10 = worst pain imaginable. If the NRS was higher than 7, patients were administered with rescue opioids such as fentanyl 25 mcg or pethidine 50 mg. The ROD was converted to the total morphine equivalent dose with an opioid converter. The rescue opiod analgesia dose and time of administration were recorded. All measurements were made and recorded by another investigator who was also blind to the procedure.
4. Statistical analysis
The sample size was determined from a previous study of ISB and IA groups. On the basis of previous studies [7,8], we hypothesized that we could observe a 50% reduction in the NRS immediately after anesthesia between the ISB and IA groups because there have not been reports on comparisons between ISB and CCE. A power analysis estimated that 15 patients would be needed in each group to provide a 90% chance of detecting such a reduction at the 0.05 level of significance. To compensate for possible dropouts, we recruited 19 patients per group. The normally distributed data were presented as the mean ± standard deviation, and the groups were compared using a one-way analysis of variance (one-way ANOVA) and a post-hoc Scheffe test along with Dunnett's T3 test for height, weight, and age and for the ROD. A P value of < 0.05 was considered to be statistically significant. All statistical analyses were performed using Stata, version 11.0 (StataCorp, College Station, TX, USA).
Go to :
RESULTS
There were no statistically significant differences in the demographic data among the three groups (Table 1).
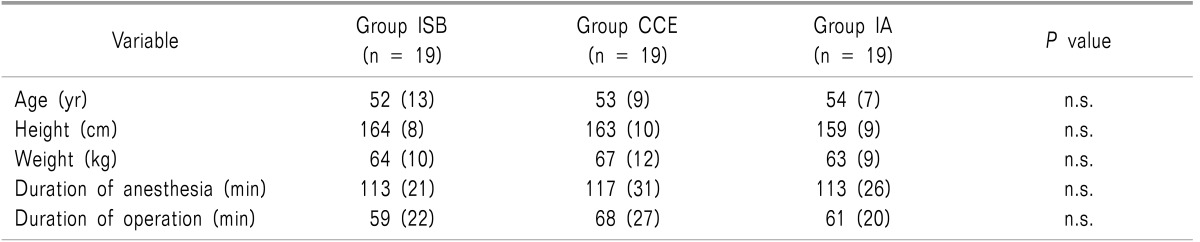
Table 1
Dermographic Data in the Three Groups
Result are expressed as mean (SD). No statistical difference isfound among groups. Statistical significance istested by one way ANOVA among groups. NRSR: numerical rating scale at rest, NRSM: numerical rating scale on movement, ISB: interscalene brachial plexus block, CCE: continuous cervical epidural block, IA: intraarticular injection, n.s.: nonsignificant (P > 0.05).
![]()
The NRS showed significant statistical differences among all three groups (P < 0.001). Postoperative NRSs were reduced in the ISB and CCE groups as compared to the IA group at rest and on movement at 30 min, 4, 24, 48 h. The ISB group showed reduced NRSs at rest and on movement compared to the scores of CCE and IA groups at 30 minutes postoperatively (Fig. 1) (vs. the CCE group, and vs. the IA group, P < 0.001). ROD were 1.6 ± 2.3, 3.0 ± 4.9 and 7.1 ± 7.9 mg morphine equivalent dose in groups CCE, ISB, and IA groups (P = 0.001), respectively, and statistically significant differences were noted between the CCE and IA groups (P = 0.01) but not between the ISB and CCE groups.
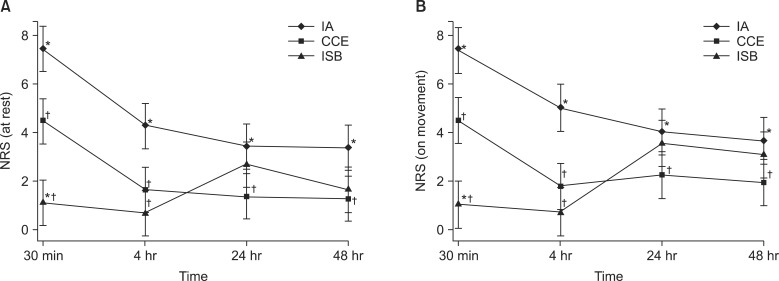 | Fig. 1Changes in NRS pain score at rest (A), on movement (B), NRS scores (mean ± SD) were measured at 30 minutes, 4 hours, 24 hours, 48 hours after surgery. ISB: interscalene brachial plexus block, CCE: continuous cervical epidural block, IA: intraarticular injection, *P < 0.05 compared with the CCE group; †P < 0.05 when compared with the IA group.
|
Go to :
DISCUSSION
We confirmed that an ISB is as effective an analgesic technique as CCE for postoperative pain control in patients undergoing ASS.
ASS is associated with severe postoperative pain. Analgesia for shoulder surgery includes subacromial or the intraarticular infiltration of local anesthetics, a suprascapular block with or without an axillary (circumflex) nerve block, a single-injection interscalene nerve block and a continuous interscalene nerve block [3].
ISB is one of the most common regional anesthesia techniques utilized, and many reports have described the effectiveness of and complications associated with ISB [2,4,9,10,11,12,13,14,15,16]. The recent use of ultrasound guidance for ISB has been shown to minimize adverse effects with an injection under the direct visualization of the target nerve and an injection of a lower dose of local anesthetics [16,17]. Improved postoperative pain control using the ISB method is linked to an earlier initiation of rehabilitation, as evident in other studies [18]. IA has been popular among surgeons because it is perceived as a simple and effective technique associated with improved analgesia, the reduced use of analgesics, and improved patients' satisfaction [3,19,20]. Savoie et al. demonstrated improved analgesia and reduced analgesic requirements with a continuous IA of 0.25% bupivacaine (2 ml/h for 48 h) in patients undergoing subacromial decompression under general anesthesia. In addition, Stephen et al. demonstrated that a single ISB plus a continuous IA of 0.5% ropivacaine at 2 ml/h improved analgesia [21]. Therefore, we used a continuous IA of 0.25% ropivacaine at 2 ml/h. CCE was reported in a few studies to provide excellent postoperative analgesia for patients undergoing upper extremity surgery [6,22,23]. Narouze et al. [24] reported that CCE was effective in the rehabilitation phase after shoulder surgery for adhesive capsulitis. Therefore, we presumed that cervical epidural analgesia may be effective as a means of postoperative pain control and rehabilitation following ASS. However, placement of a cervical epidural catheter is not a commonly used procedure. Rare but severe complications such as an epidural abscess and permanent spinal cord damage can be devastating, making CCE less attractive for general use [6]. Although lumbar and thoracic epidural analgesia has been studied in various surgical situations as an effective analgesic method in comparison with a peripheral nerve block in a number of reports [25,26,27], CCE has not been compared with other analgesic methods such as ISB and IA during ASS, as it is associated with severe postoperative pain as in open shoulder surgery. While there have been studies comparing ISB with IA with a focus on pain following ASS during surgery, there has been no research dealing with comparisons of these procedures with CCE. In our study, the severity of postoperative pain was compared among these three groups.
A few studies have reported that, IA was an effective alternative to ISB [3,19]. However, the results of the current study were identical to those of other studies, finding that ISB provided better pain control than IA [8]. Interestingly, NRSs at 30 minutes postoperatively were shown to be reduced significantly in the ISB group. It is well known that cervical epidural analgesia selectively blocks sympathetic fibers, then sensory fibers, and finally motor fibers with an increasing dose of local anesthetics. However, ISB may not achieve the effective separation of the motor and sensory block as sensory nerves are in the core bundle, surrounded by motor nerves [6,28]. Therefore, we anticipated that immediate postoperative pain control would be best achieved in the CCE group, but the NRSs of patients in this group were higher than those of the ISB group in the immediate postoperative period. This study showed, however, that the ROD was lowest in the CCE group. ISB was shown to be effective for 10-12 hours in controlling postoperative pain [12,14]. In order to control postoperative pain after 12 hours in the ISB group, a fentanyl patch was applied to the patients. Although an additional injection of analgesics after the 12-hour window of the ISB effect had statistically insignificant results, it appeared that the injected amount of analgesics was smaller in the CCE group.
Contrary to the IA, CCE and ISB were performed before surgical incision. Preemptive analgesia in procedures such as CCE and ISB could explain their superior analgesic efficiency compared to IA [5].
In our study, side effects were not evident in the ISB and CCE groups using ultrasonography and a C-arm device. Due to their requirement of highly skilled techniques, cervical epidural procedures are not commonly recommended. A cervical epidural block has always been viewed as a relatively safe procedure, with complication rates ranging from 0-16.8% [3]. Although CCE demands a high degree of skill, it should also be considered as an effective means of controlling pain after ASS due to its comparatively low incidence rates of complications and its pain-relieving effects.
The study has several limitations. First, the number of participants in each group is relatively small if seeking to claim strong statistical power. Second, due to the difficulties in evaluating actual blood concentrations of local anesthetics, it is difficult to conclude that equal anesthetic effects were achieved in the three groups despite the fact that identical anesthetic agents and dosages were administered. Third, evaluations of experimental factors such as pain scores were not performed blindly after the assignment of patients into the three groups. Since it is known that factors associated with incisions such as fibrosis and joint inflammation influence the operation time and types of anesthetics [29], future research will be required to study those factors.
In conclusion, ISB is as effective an analgesic technique as CCE for postoperative pain control in patients undergoing ASS.
Go to :
 XML Download
XML Download