

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Pain is one of the most common symptoms affecting surgical patients during the postoperative period. Since pain is very subjective and a highly personal experience, it is affected by many factors related to each individual's special characteristics [1]. Despite the evolution of anesthesia and analgesics, one third of the patients still complained about moderate to severe pain after surgery [23]. Effectively controlling the postoperative pain is desirable for various reasons. The postoperative course of the patients should be as comfortable as possible and cause the least possible distress. Failure to adequately control pain may lead to unfavorable postoperative course, long hospitalization, and even chronic pain [345].
Many efforts have been made to identify predictors of postoperative pain [13]. Unfortunately, the factor of "educational status" has not been studied extensively. It has, however, been found that low education is associated with a higher incidence of painful conditions [6]. The few studies that assessed the association of the educational status with the postoperative pain were inconclusive. They either showed no association [78] or in one case a negative association ( i.e. the higher the education, the lower the pain) but this was based only on 40 patients [9]. To our knowledge though, there is no study that actually addressed directly this issue since the aforementioned studies had a different aim. Moreover, we are not aware of any other study performed in a large number of general surgery patients like ours.
On the other hand, a lot of effort has been made to educate the patients preoperatively about the operation and the associated sequellae in order to effectively control the pain. Even in cancer patients, this approach seems to be effective as this was shown in a recent meta-analysis of randomized controlled trials (RCT) [10]. Similar results were presented previously by others [11]. Generally speaking, the structured preoperative education has been found to have a beneficial effect on postoperative pain, anxiety, and recovery; hence, this approach has been used extensively to alleviate the postoperative complications [12]. Various methods of education have been used in an attempt to universally educate the patients before the operation, and these depend both on the delivery method and the ability of the recipient comprehend and interpret the necessary information.
We believe that the educational status of the patients is a significant predictor of pain. In the absence of sufficient evidence, we designed this study in order to assess if there is indeed an association, and which other factors should be taken into account preoperatively in order to have the optimal results in terms of pain management. Our aim was to identify the group of patients at risk for a higher pain score, based on their educational status in order to find a way to offset this handicap, if any.
Go to : 
MATERIALS AND METHODS
The study was approved by the ethical review board of the hospital. We prospectively enrolled 400 consecutive general surgery patients who were operated on within 6 months. Patients who remained intubated or were admitted to the intensive care unit were excluded from the study. Moreover, we excluded a small number of patients (not native speakers) who could not adequately comprehend well and comply with our instructions. On admission, they were asked if they wanted to participate and if they agreed, they were interviewed by a doctor of the study group. The interview was predesigned based on the known factors related to postoperative pain. It included, apart from the demographics, questions about the educational status, the level of preoperative pain, the use of analgesics or other medications related to pain or mood control, the smoking history, the previous experience with surgery, the psychological state, the type of operation, the type of incision and finally, if the operation was an emergency procedure or elective.
The psychological state was assessed with the Hospital Anxiety and Depression Scale (HADS) [13] which is a fourteen item scale with a score ranging from 0-21 for each. Seven of the items relate to anxiety and seven relate to depression. It is a self-assessment scale for detecting symptoms of anxiety and depression in non-psychiatric patients from a medical department. A review on the validity and reliability of HADS confirmed the assumption that HADS performs well in screening for the separate dimensions of anxiety and depression [14].
Based on the score we can classify the psychological status of the patients (anxiety, depression) as: normal (0-7), mild (8-10), moderate (11-14), and severe (15-21). Scores for the entire scale (emotional distress) range from 0-42, with higher scores indicating more distress. We then further classified the patients in two major groups according to the psychological state: normal (0-7) and with a significant level of anxiety or depression (> 8).
For the assessment of pain we used two methods: (a) The visual analogue scale (VAS) which is a psychometric response scale where the patient has to indicate a position along a continuous line between two end-points (no pain and maximum pain) [15] and (b) the numeric rating scale (NRS) which is a segmented numeric version of VAS in which the patient indicates the number (0-10) that best reflects the intensity of their pain. Both tests are easily obtained, reliable, valid and able to detect changes over time [15]. We used both tools in order to minimize the chance of under- or overestimating the pain.
Pain intensity was assessed preoperatively and for the first 7 postoperative days. The patients were visited by the responsible doctors 3 times a day during the ward rounds and were asked about the pain intensity and the need of analgesia. The highest pain intensity score of the day was eventually recorded. The type and amount of analgesia required was also recorded from the 1st to the 7th postoperative day. We classified the analgesia requirements into 3 major groups: 1.NSAIDS (1-2 doses every day), 2.Tramadole HCL 100 mg or pethidine 50 mg (1-2 doses every day), and 3.Tramadole HCL 100 mg or pethidine 50 mg (more than 3 doses every day). We further classified the patients into 2 groups 1.NSAIDS and 2.Opioids/Stronger painkillers.
We did not record the pain on the day of the operation on purpose and we neither recorded the analgesia given since this was highly dependent on the anesthesiologist's preferences. Nevertheless, from postoperative day one and onwards, the analgesia was given on the patient's demand and was recorded by our team.
The educational status was classified as: up to junior school, up to high school, and university. Based on that, we classified the patients into 3 distinct groups. After the initial analysis (since there were no differences between the medium and the high education groups), we further classified the patients into two groups based on the educational status: Group A: Low education (up to junior school) and Group B: high education (from the high school and above).
1. Statistics
The statistical analysis was carried out using SPSS for Windows version 19 software package (Statistical Package for Social sciences; Inc, Chicago, IL).
For categorical variables, we used the Pearson Chi-square test and Fisher's exact test. In tables bigger than 2 × 2, when the null hypothesis for independence was rejected, (i.e. the variables in the x axis were dependent from the variables in the y axis) we compared the observed frequencies with the expected frequencies (standardized residual) for each cell in order to identify which comparisons led to significant outcomes. In order to do this, we compared the size of the standardized residuals to the critical values that correspond to an alpha of 0.05 (±1.96) to identify the observed values which were significantly more or less than the expected values.
For the continuous variable, we used independent sample t-test for equality of means to assess if there were any statistically significant differences between the means of the outcome values.
For comparisons involving more than 2 groups, we used analysis of variance (ANOVA) to identify statistically significant differences between the means of the outcome values of the groups.
Having rejected the Null hypothesis (i.e. statistically significant effect in ANOVA), we further applied follow-up tests (post-hoc) to assess which groups were different from which other groups or to test various other focused hypotheses. The "Tukey's" and "Bonferroni" post hoc tests were used. We considered significant differences those with P < 0.05. Binary logistic regression was used to assess if there were significant predictors of binary outcomes.
Go to :
RESULTS
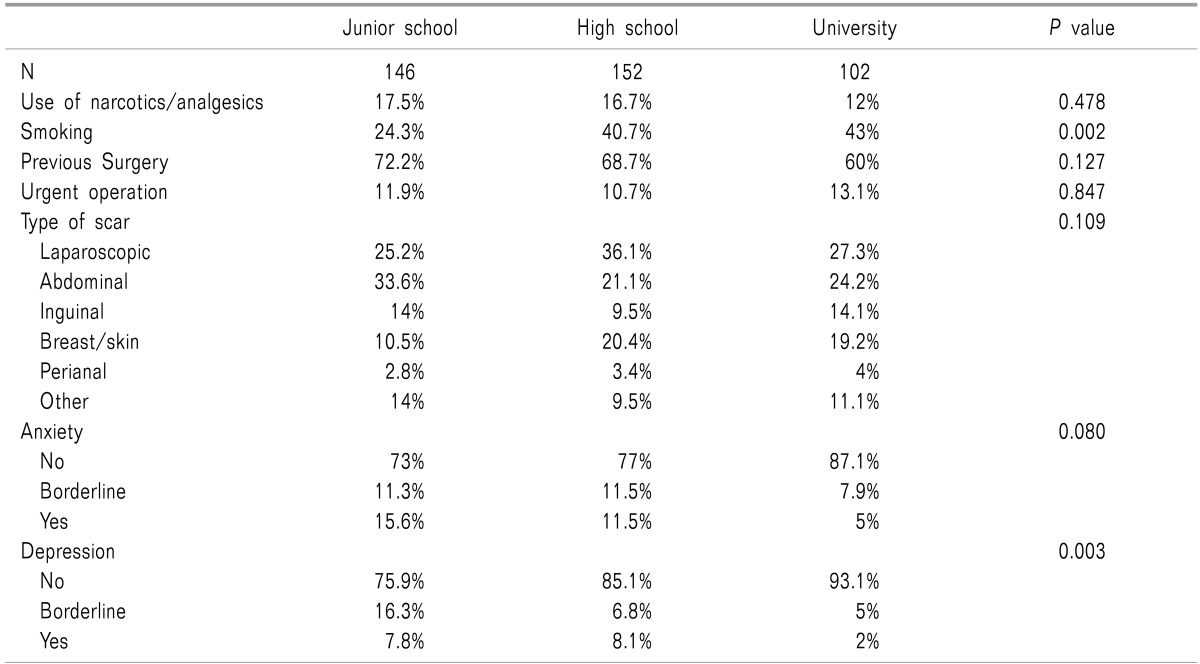
During the study period, 400 patients were enrolled, 180 male (45%) and 220 female (55%) with a mean age of 57 ± 18.4 years. The mean weight was 75.4 ± 15.3 kg and the mean height was 168 ±9.2 cm. In our sample, 35.3% were smokers, and 67% had previous surgery. In terms of educational status, 36.5% went to junior school, 38% to high school and 25.5% to university. The vast majority did not have any analgesia before the operation (81%) and did not use any narcotics (84%). In terms of anxiety, 78% were classified as normal while 22% had a certain level of anxiety. In terms of depression, 84% were classified as normal and 16% had a certain level of depression. None of the patients were officially diagnosed with anxiety or depressive disorder although, as mentioned above, some patients were under mild anxiolytic medications. The vast majority of the patients underwent an elective operation (88%). The demographics of the patients based on the 3 groups of the educational status are included in Table 1 and 2. Although 67% of the patients had a history of hospitalization and/or previous surgery, there was no statistically significant difference for this factor between the educational groups, and so it was excluded as a confounding factor. From the known predictors of pain the univariate analysis showed that the age, the anxiety and the depression were significantly different between the 3 groups. The lower the educational status was, the higher the anxiety and the depression were. The junior school graduates scored the highest scores and the university graduates the lowest scores. Moreover, patients with low education (junior school) were older than the two other groups. There was no statistically significant difference in the type and quantity of the analgesia required between the groups during the study period.
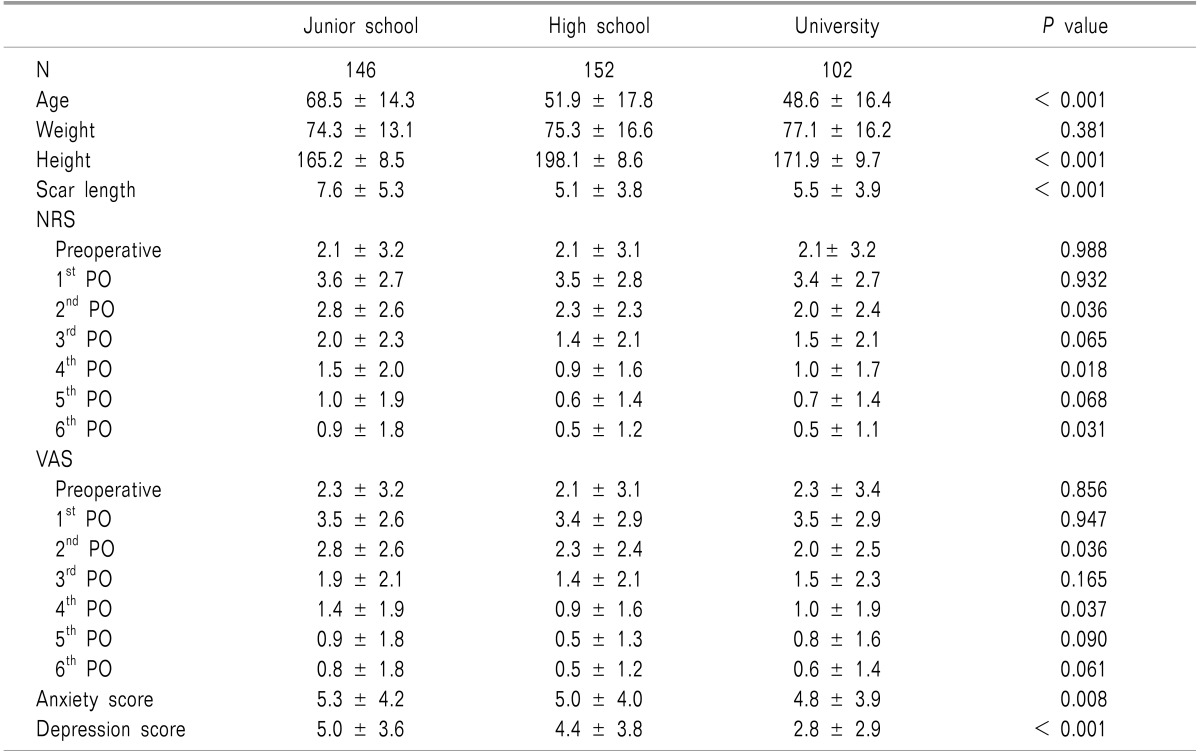
Since all differences found were between the junior school and the other two categories (high school, university) and since there were no significant differences between the group of high school and the one of university (Table 1 and 2), for the purpose of the study and in order to facilitate the interpretation of the results we used a two group analysis: Group A = low education, up to junior school and Group B = high education including high school and university (Table 3 and 4).
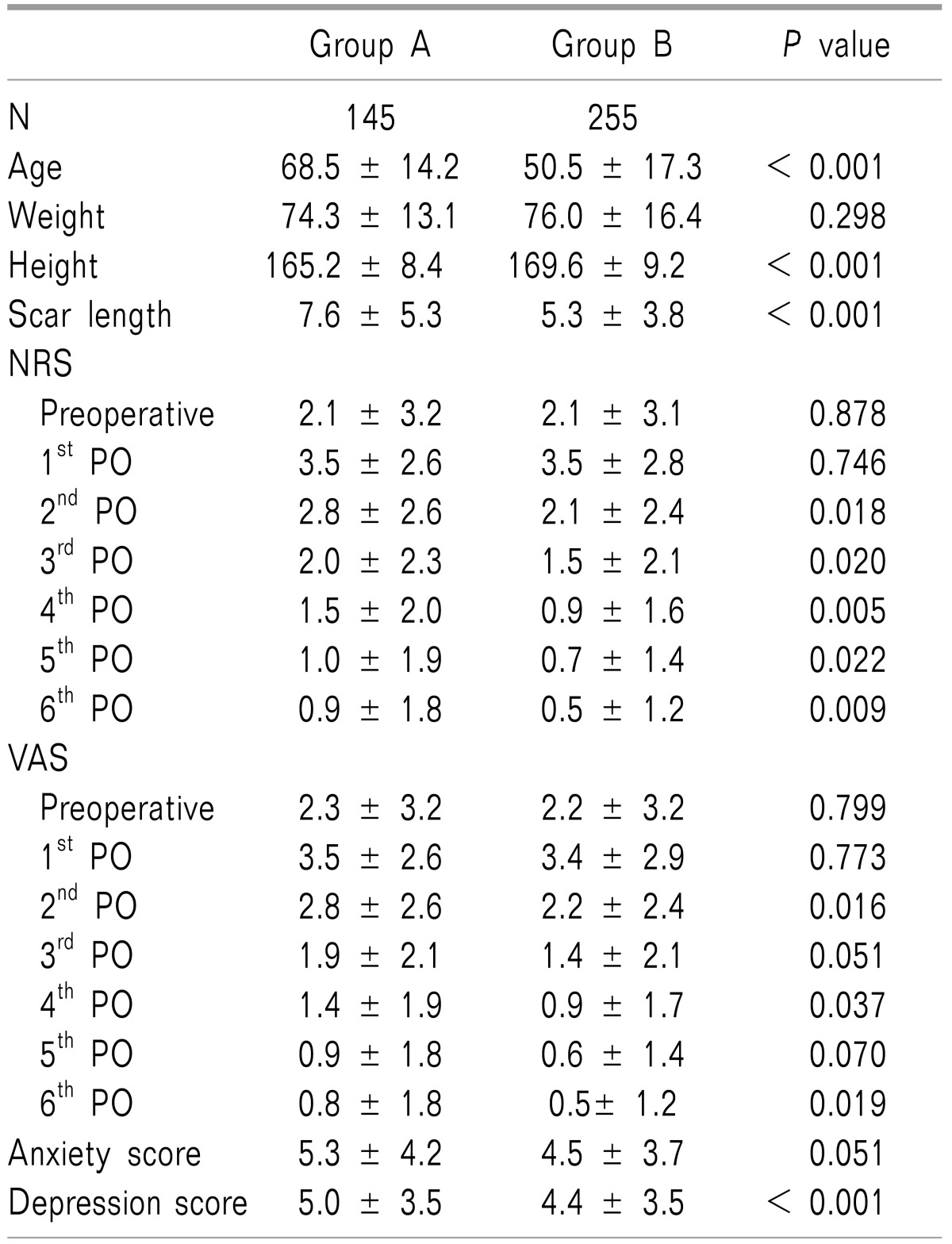
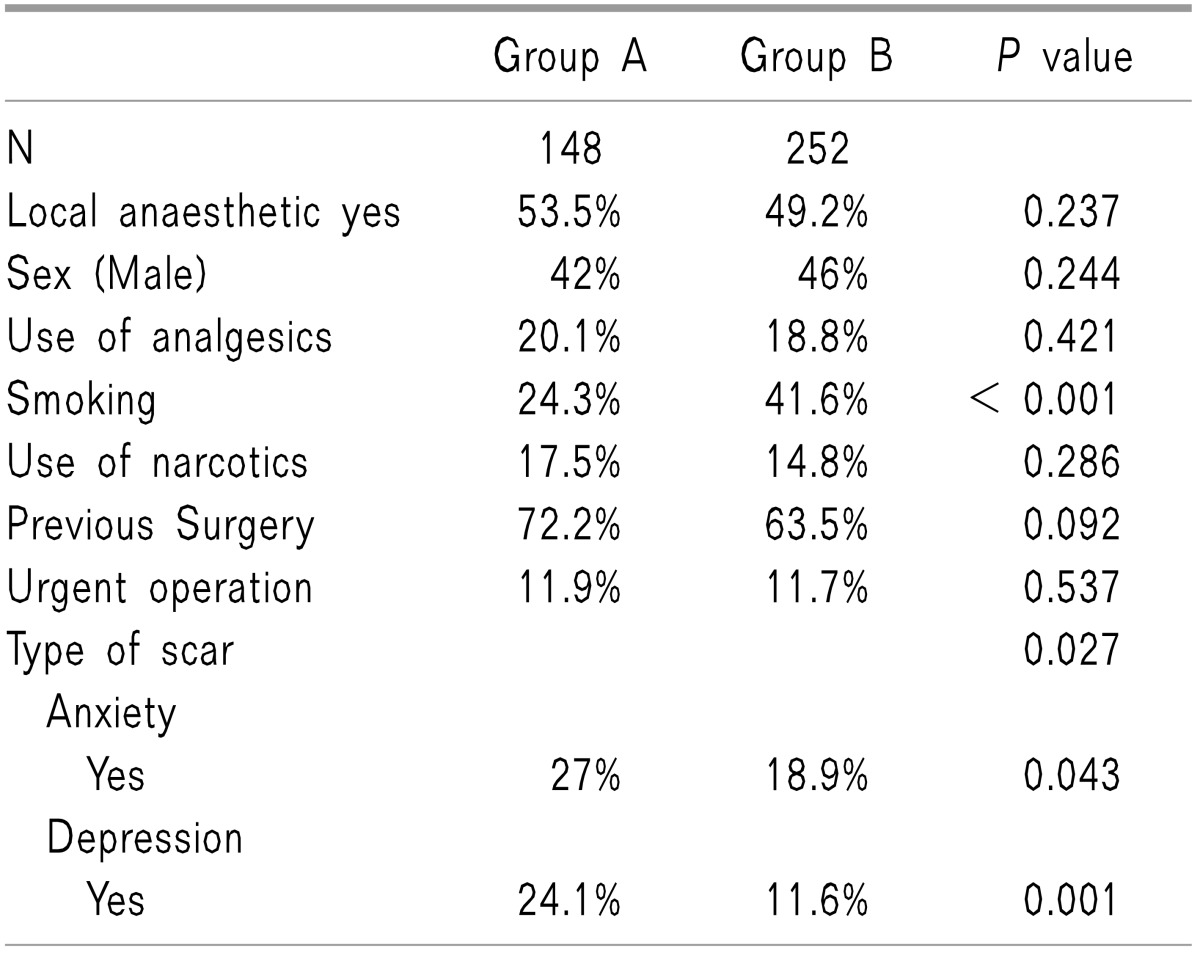
We found that patients of group A were older than patients of group B. There was no difference in the anxiety score but there was a higher depression score in group A (Table 3). When we compared the 2 groups in terms of being normal or having a level of anxiety or depression, we found that group A had significantly a higher percentage of psychological conditions (Table 4).
The type of scar was found to be significantly different between the groups (P = 0.027). This was mostly because more patients in Group A underwent an abdominal incision (33.6%) than patients in Group B (22.4%), (P < 0.05). Moreover, more patients in Group B had a breast/skin incision (19.9%) than patients in Group A (10.5%), (P < 0.05). No significant difference was found between the groups for the remaining type of scars: laparoscopic, inguinal, perianal and other.
In terms of the outcomes, despite the fact that there was no significant difference in the preoperative pain and the pain on the 1st PO day, there was significantly higher pain score in group A from the PO day 2 onwards (Table 3). In terms of the analgesia, there was no significant difference between the 2 groups in neither the type nor the quantity of the analgesics used.
The multivariate analysis (binary logistic regression), where all the known predictors of pain were included, showed that the 2 groups were significantly different only for the presence of depression.
Nevertheless, based on the fact that there were differences between the groups in terms of age, anxiety and depression, we conducted a subgroup analysis based on these factors.
1. Depression (this predictor was found to be significant in both the multivariate and the univariate analysis)
1) No depression
When we compared Group A with Group B for patients who did not have depression, we found that there were still significant differences in the weight, height and length of scar but no difference in their weight and the anxiety score. More specifically, patients of Group A were older (66.6 years vs. 50.5 years, P < 0.001), shorter (165.7 cm vs. 169.8 cm, P < 0.001) and had a longer scar (6.9 cm vs. 5.4 cm, P = 0.003). There were no differences in the preoperative and postoperative pain. More people of group B were smokers (41.1% vs. 23.3%, P = 0.002) but otherwise there were no differences in the sex, in the use of analgesics or narcotics before the operation, in the experience of previous operations, in the percentage of urgent operations, in the type of the scar, and in the anxiety score. Furthermore, there were no differences in the type and quantity of the analgesia required postoperatively.
2) Depression
People of Group A were older (73 years vs. 52.3 years, P < 0.001) and had a longer scar (9.5 cm vs. 4.4 cm, P = 0.001) but otherwise there were no differences in the weight, height, preoperative pain and anxiety score. Despite the fact that there were no differences during the 1st PO day, significant differences were observed during the postoperative period in terms of the pain intensity between the groups. More specifically, a higher pain score was observed in Group A for the 2nd PO day (3.7 vs. 2.0, P = 0.12), the 3rd PO day (2.6 vs. 1.5, P = 0.049), the 4th PO day (1.9 vs. 0.7, P = 0.015), the 5th PO day (1.5 vs. 0.4, P = 0.011) and the 6th PO day (1.3 vs. 0.3, P = 0.013).
There were no differences in the sex, use of analgesics/narcotics before the operation, smoking, previous surgery, urgent operation, and anxiety. Furthermore, there were no differences in the type and quantity of the analgesia required postoperatively.
2. Anxiety (this predictor was found to be significant only in univariate analysis)
1) No anxiety
There were more patients with depression in Group A (11.7% vs. 4.5%, P = 0.02) but otherwise no other significant differences were found in the qualitative factors. Moreover, no differences were observed in the type and quantity of the analgesia required postoperatively. Patients of Group A were older (66.4 years vs. 50.2 years, P < 0.001), shorter and with a longer scar (7.6 vs. 5.7, P < 0.001) and had a higher depression score (3.8 vs. 2.8, P = 0.002) but there were no other differences in the quantitative factors. In terms of postoperative pain, there was a higher pain score during the 2nd PO day for Group A (2.7 vs. 2.0, P = 0.026) but otherwise no other differences were observed.
2) Anxiety
Patients of Group A were older (73 years vs. 52.9 years, P < 0.001), and shorter (161.9 cm vs. 166.2 cm, P = 0.015) but there were not any other differences in the other quantitative factors or in the level of postoperative pain. There were no differences between the groups for any of the qualitative factors including the postoperative use of analgesia.
3. Age (this predictor was found to be significant only in univariate analysis)
Since age was found to be significantly different between the 2 groups, we did a subgroup analysis based on 3 age groups: the patients under 40 years old (N = 84), patients from 40-60 years old (N = 128) and patients over 60 years (N = 188).
1) Age under 40 years
There were no significant differences in any of the factors studied hence, no confounding factors. Moreover, there was no difference in the preoperative pain. On the other hand, significant differences were observed between the 2 groups during the postoperative day 2 and 3. More specifically, Group A had a higher pain score on the 2nd PO day (3.7 vs. 1.6, P = 0.005) and on the 3rd PO day (2.4 vs. 1.0, P = 0.016). Moreover, Group A required more and stronger analgesia for the 1st (P = 0.029), 2nd (P = 0.035) and 4th PO days (P = 0.005) while there were no differences for the 3rd, 5th and 6th PO day.
2) Age 40-60 years
There were no significant differences in any of the factors studied. Moreover, there was no difference in the preoperative pain and on postoperative pain. On the other hand, there were significant differences in the analgesia required. Group A required more and stronger analgesia for the 1st (P = 0.013), 3rd (P = 0.045), 4th (P = 0.038) and 6th PO days (P = 0.027), while there were no differences for the 2nd, and 5th PO day.
Go to :
DISCUSSION
In this study we found that the educational status is a significant predictor of pain. Moreover, we found that patients who had lower education were more prone to experience depression or anxiety. All these 3 factors seem to be dependent on each other.
Despite the fact that there are no similar studies in the literature (based on general surgery patients), there is data in the literature supporting our findings. More specifically, a study on heart failure patients showed that patients with low education experienced more pain than patients of higher education during the first 6 months [16].
On the other hand, it has been shown that there is indeed a strong association between educational status and mood disorders. A study investigating this association in more than 10,000 people from the general population showed that the relative risk for anxiety was significantly higher for persons with lower education and this was more pronounced in females. Moreover, the same was true for depression where it was found that the lower the education, the higher the relative risk [17]. In the aforementioned study, people of lower education were found to have differences in their socioeconomic status and the material factors. The differences in the socioeconomic status (SES) in patients with lower education are most likely responsible for the higher incidence of mood disorders in this population.
Low SES has been constantly related to mood disorders [1819]. Nevertheless, education is an independent factor influencing rather than being the result of the SES, since it is offered free in most countries (at least in Greece) and precedes occupation and income, which are factors influencing the SES thereafter. Obtaining a good education increases the odds to succeed in western society and achieve goals associated with good emotional well being. Studies have shown that there is a cumulative protective effect of high education on mood disorders, especially depression, and a subsequent advantage on physical health. The HUNT study investigated if the higher education protects against anxiety and depression. In this study, like us, they used the HADS to assess the mood conditions. It was shown that the lowest educational level was associated with higher anxiety/depression scores and this is in line with our findings [20]. The association of low education with anxiety is important since anxiety, when excessive, may have a negative impact on the course and recovery of the surgical patients. It has been widely supported that the anxiety about the anticipated pain and the feeling that there is lack of control of that, sensitizes the individual to the pain stimuli by increasing the reactive pain [2122]. It has been shown that gaining control or understanding better the anticipated condition leads to better adaptation and improved tolerance of it, since the condition may be rendered less threatening. This can be achieved by properly educating the patients and depends on the level of education and the way the medical personnel approaches the patients. Educating patients about the medical actions that will take place should not be a passive process with no confirmation of whether the information is comprehended. On the contrary, it should be an interactive process, with confirmation that learning has taken place [21]. Nevertheless, the patients can be classified in two categories according to the desired level of preoperative education and the amount of information they want to be given: the vigilant and the avoidant [23]. Therefore, information should be tailored to suit each individual's general level of understanding, education and cultural background [24]. Eventually, patients who understand more about their condition will comply with their care needs and will facilitate their recovery and minimize the hospitalization need [21].
A systematic review on the impact of the preoperative education on the postoperative pain showed that this intervention is indeed effective but none of the studies compared the effects of preoperative education and 'no form of education,' and therefore the actual impact may have been underestimated. Nevertheless, sufficient evidence was found to support the effectiveness of preoperative patient education in the improvement of postoperative outcomes [25].
In our study it is important that there was no difference in the preoperative pain between the groups and that the groups were not different in most of the known confounding factors such as sex, use of narcotics/analgesics, previous experience with surgery, urgency of the operation and weight. Patients of lower education experienced more pain than the rest of the patients during the 1st PO week. There was a correlation of the educational status with psychological factors; i.e. anxiety and depression which are known predictors of postoperative pain. It is possible that these factors may have contributed to the results of our study. Indeed, when we did a subgroup analysis including only the patients who did not score high enough for depression (normal), the differences in the intensity of pain between the 2 groups were eliminated. In this subgroup analysis the difference in the mean age between the 2 groups was still significant as was the length of the scar. It is important that there were no differences in the anxiety level which could have acted as a confounding factor. Based on these findings, we may conclude that the educational status is not a "handicap" if we manage to alleviate or control the "subclinical" depression of these patients, and this should be our aim as clinicians. This can be achieved with a proper structured preoperative education and a psychiatric consultation for those patients who score high in the HADS.
On the other hand, when we included only the patients who had a level of depression, the lower education group had a higher pain score on the PO day 2 onwards and this matched the overall results of the analysis. Based on this, we may assume that patients who have lower education cannot effectively manage their subclinical depression during the perioperative period, as opposed to patients of higher education. On the other hand, if the patients have no psychological issues, the educational status has no impact on the perception of pain. When we did a subgroup analysis based on the state of anxiety, we did not find any further differences between the groups, hence the anxiety only mildly affected the results.
Based on the fact that one out of four patients with a lower level of education had some form of depression, this should be taken into account when trying to educate the patients preoperatively.
Although all patients were informed about their operation in the same way by the same trained medical personnel, it is possible that patients of lower education either failed to correctly interpret the information given or hesitated to ask for clarifications when in doubt. This may explain the fact that despite the fact that they had higher pain scores, they did not receive additional or stronger analgesia available on demand by the nursing staff.
Finally, age is known to influence the perception of pain and indeed there were differences between the educational groups. When we stratified the patients according to their age we found that the impact of educational status was very pronounced in the younger patients (i.e. < 40 years), less pronounced in the middle age group (40-60 years) and was eliminated in the elderly (> 60 years). Interestingly when we stratified the patients in 3 age groups, all differences between the groups in all confounding factors were eliminated and the two groups were perfectly matched. Henceforth, in this subgroup analysis all differences found in the main outcomes can only be attributed to the impact of the level of education. Even if anxiety and depression are confounding factors, and one can speculate that they have interfered with our results, there is no doubt that the educational status is an independent predictor of pain based on the subgroup analysis for age groups.
Nevertheless, our study has limitations. The type of anesthesia and the type of intraoperative analgesia varied from patient to patient and may have influenced our results. Since this effect is limited to the early postoperative period, we did not record the pain intensity and the analgesia requirements during this time to avoid this confounding factor. There is a chance though that more extended effect may have influenced our results. Furthermore, the educational status is just an indicator of the actual cultural and social status of a person. Classifying the patients based on validated questionnaires may have been more appropriate in future similar studies.
Despite these limitations, we believe that the educational status should always be taken in account during the preoperative assessment of the patients. If the patients are of lower education, they should further be assessed for depression and anxiety (e.g With HADS) and if not found to be entirely normal, special effort and extra care should be given in educating them properly and alleviating their psychological distress. This seems to be more useful for young and middle-aged patients.
If we manage to do so, we will likely succeed to compensate for their "handicap", minimize the impact of the lower education on the postoperative pain and allow them to have a better, more comfortable and less stressful recovery from the surgery. Further RCT should be done in order to provide better evidence about the success of this approach.
In conclusion, the educational status may be a significant predictor of postoperative pain due to various reasons, including the poor understanding of the preoperative information, the level of anxiety and depression caused by that and the suboptimal request and use of analgesia. Younger patients (< 40), and patients with subclinical depression are mostly affected while there seems to be no impact on patients over 60 years old.
Go to :
 XML Download
XML Download