

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
It has been reported that the prevalence of neuropathic pain in community-dwelling adults is 9.8% [1], and that 21.4% of emergency patients and 24.5% of post-surgical patients have or might have neuropathic pain[23]. Many studies have tried to reduce neuropathic pain in animal studies [456]. However, controlling neuropathic pain following nerve injury is still difficult, and severe neuropathic pain contributes to a decrease in quality of life.
Olanzapine, a thienobenzodiazepine, is a recently developed atypical anti-psychotic drug for schizophrenia and bipolar mania, with a safer side effect profile than traditional neuroleptics [78]. Its antinociceptive and anti-neuropathic properties have been evaluated in animal models and clinical case studies [910111213141516]. However, to our knowledge, the preventive treatment effects of olanzapine have not been investigated in a neuropathic pain model.
Thus far, many studies have reported that microglia of the spinal cord play an important role in the pathogenesis of nerve injury-induced pain [1718]. Intrathecal injection of microglial inhibitors, for example, inhibited allodynia in diabetic pain and other neuropathic pain models [1920]. Furthermore, chronic intraperitoneal injection of a microglial inhibitor, but not an astroglial inhibitor, diminished neuropathic pain symptoms in a peripheral neuropathic pain model [21].
In the present study, we examined whether olanzapine pre- and post-treatment inhibits the development of mechanical allodynia in the partial sciatic nerve ligation model and whether its effects are dose-dependent. In addition, we examined whether olanzapine treatment inhibits activities of microglia in the ipsilateral dorsal horn of the lumbar spinal cord.
Go to : 
MATERIALS AND METHODS
1. Animals
All experimental procedures were approved by the Institutional Animal Care and Use Committee of the University of Tsukuba and adhered to the guidelines of the Committee for Research and Ethical Issues of the International Association for the Study of Pain. Adult male Sprague-Dawley rats (250-350 g) were used in all experiments, and housed under controlled conditions (14- and 10-h light/dark cycle; room temperature, 23-24℃) with free access to food and water.
2. Surgical procedures
All rats were anesthetized with isoflurane (2-2.5%). The partial sciatic nerve ligation model was prepared in a sterile manner according to the procedure of Seltzer and colleagues [22], with minor modifications. The right sciatic nerve was exposed at the thigh-high level. An 8-0 silicon-treated silk suture was inserted into the nerve and tightly ligated so that the dorsal 1/3-1/2 of the nerve thickness was trapped in the ligature. The wound was then closed with 2 muscle and 3 skin sutures (4-0 cotton). In sham-operated rats, the nerve was exposed without ligation.
3. Mechanical allodynia test
A traditional Dixon up-down method was used to measure mechanical allodynia. Rats were individually placed into chambers over a mesh table and acclimatized for 15 min before the onset of the examination. Withdrawal threshold was determined using a series of von Frey filaments with incremental stiffness (0.4, 0.6, 1, 1.4, 2, 4, 6, 8, 10, 15, and 26 g; Stoelting, Wood Dale, IL), beginning with the 2 g filament. Filaments were applied vertically to middle of the plantar surface of the ipsilateral hindpaw before and 7 days after the surgery. A cut-off pressure of 26 g was set to avoid tissue damage. The observer was blinded to all test conditions.
4. Experimental protocols
1) Pre-treatment effect
In the first stage of the study, groups of rats were injected intraperitoneally with olanzapine (10 mg/kg) or normal saline (10 ml/kg) to investigate the pre-treatment effect of the drug in preventing allodynia.
Twenty-two rats were divided into 3 groups: a sham group (n = 6), a normal saline group (n = 8), and the olanzapine group (n = 8). The olanzapine group rats were injected intraperitoneally with 10 mg/kg olanzapine 1 h before the surgery. Olanzapine (Eli Lilly and Company, Indianapolis, IN) was dissolved in normal saline (1 mg/ml). The sham and normal saline group rats were injected intraperitoneally with normal saline (10 ml/kg) 1 h before the surgery. The dosage of olanzapine used in the present study was based on a previous report, in which an injection of 10 mg/kg showed the maximum antinociceptive effect in the mouse tail-flick assay [9]. Mechanical allodynia was measured before and 7 days after the surgery. Each animal was sacrificed for Iba-1 immunohistochemical analysis after the last behavioural study.
2) Post-treatment effect
In the second stage of the study, groups of rats were injected intraperitoneally with 10 mg/kg olanzapine or 10 ml/kg normal saline to investigate the post-treatment effect of the drug in preventing allodynia. Twenty rats were divided into 3 groups: a sham group (n = 6), a normal saline group (n = 7), and the olanzapine group (n = 7). Olanzapine (10 mg/kg) or normal saline (10 ml/kg) was injected intraperitoneally 1 h after the surgery. Other protocols were the same as described for the pre-treatment study.
3) Dose-dependency
In the last stage of the study, groups of rats were injected intraperitoneally with 2.5 mg/kg or 50 mg/kg olanzapine to investigate the dose-dependency of the drug in the present study procedure. Fifteen rats were used because three rats of the large-dose group had died. A small-dose olanzapine group (n = 6) and large-dose olanzapine group (n = 9) was injected intraperitoneally with 2.5 mg/kg and 50 mg/kg olanzapine, respectively, 1 h after the surgery. The small and large doses of this experiment were based on a previous report, for which 2.5 mg/kg and 50 mg/kg were the minimum and maximum doses, respectively [9]. Olanzapine used in the small-dose group was dissolved in normal saline (0.25 mg/ml). In the large-dose group, it was dissolved in normal saline (2.5 mg/ml) because of the solubility limit.
5. Immunohistochemical staining
Under deep pentobarbital anesthesia (60 mg/kg i.p.), animals were perfused via the ascending aorta with 500 ml of phosphate-buffered saline (PBS; pH 7.4), followed by 500 ml of 4% paraformaldehyde fixative in a 0.1 M phosphate buffer. After perfusion, the lumbar spinal cord was removed and post-fixed in the same fixative for 2 h at 4℃. Ten or twenty sections (40 µm thick) were sliced, and these sections were processed for Iba-1 immunohistochemistry using the avidin-biotin peroxide complex (ABC) method. The tissue sections were washed with 3% hydrogen peroxide for 30 min at room temperature and were then incubated at 4℃ in PBS containing the primary antibody to Iba-1 (rabbit, 1:160,000, 15 h; Wako, Osaka, Japan). The samples were then processed according to the standard protocol employed for the ABC method (Vectastain Kit; Vector Laboratories, Burlingame, CA), using diaminobenzidine tetrahydrochloride as a chromogen. A quantitative analysis of Iba-1 density was performed using a constant parameter set (exposure time, gain, and post image processing). We measured the area of Iba-1 staining within the dorsal horn using the freely available software Image J (developed at the U.S. National Institute of Health). Throughout the data collection phase, the investigator was blind to the conditions of the animals.
6. Definition of catalepsy
We neither forced the rats into unusual postures nor measured the latency for the animals to remove themselves from uncomfortable postures. Olanzapine injected rats lost their voluntary movements, touched the floor with their abdomen, and kept the posture until they were interfered with. We defined these conditions as catalepsy.
7. Statistical analysis
Sample size calculation was based on a pilot study. Comparisons of body weight data were performed using analysis of variance (ANOVA) and the Tukey post-hoc test. The Kruskal-Wallis test and the Steel post-hoc test were used to assess mechanical allodynia and the immunohistochemical data. A P value of less than 0.05 was considered statistically significant.
Go to :
RESULTS
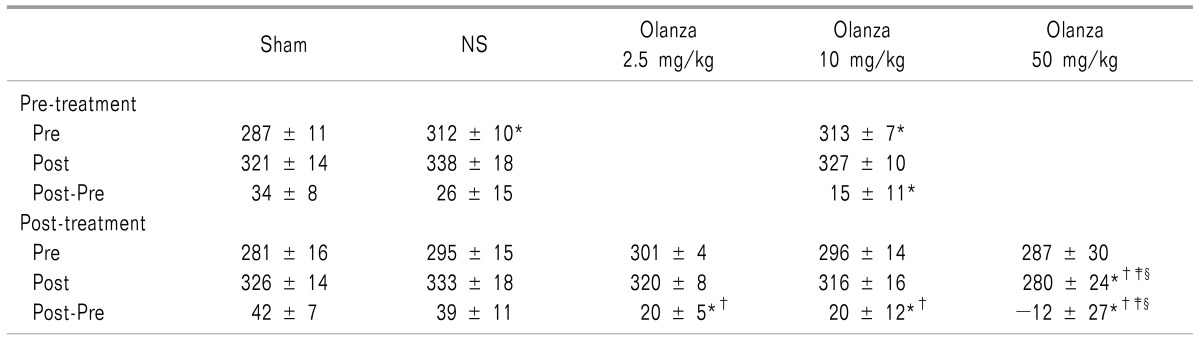
The rats given olanzapine temporarily decreased their intake of food and water because of catalepsy. Body weights of rats in the 2.5 mg/kg and 10 mg/kg olanzapine groups increased again toward the end of the study and did not differ from those of the normal saline and shamoperated groups on the 7th day after surgery (Table 1). Large doses of olanzapine significantly impaired body weight increase. We speculated that three rats from the 50 mg/kg olanzapine group died from starvation. The catalepsy continued for 1 to 3 days after the injection. None of the rats showed allodynia before the surgery.
1. Behavioural features
In the pre-treatment study, the median withdrawal threshold of the normal saline group (12.3 g) was significantly lower than that of the sham-operated group (26 g) (P < 0.05) (Fig. 1). However, the median withdrawal threshold of the olanzapine group (26 g) did not differ from that of the sham-operated group.
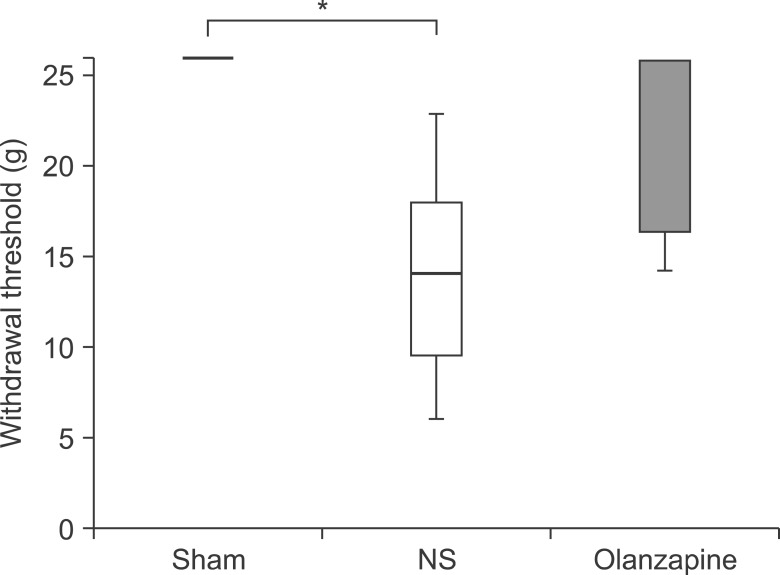 | Fig. 1Mechanical withdrawal threshold of pre-treatment groups on the 7th day after partial sciatic nerve ligation (pSNL). Sham, NS, and Olanzapine indicate sham-operation + vehicle (normal saline), pSNL-operation + vehicle (normal saline), and pSNL-operation + olanzapine (10 mg/kg) groups, respectively. Median thresholds are indicated with horizontal bars. The vertical bars indicate the range and horizontal boundaries of the boxes represent the first and third quartiles. *P < 0.05 vs. Sham-operation group.
|
In the post-treatment study, the median withdrawal threshold of the normal saline group (15.2 g) was also significantly lower than that of the sham-operated group (26 g) (P < 0.05) (Fig. 2). No significant difference in the median withdrawal threshold was found between the olanzapine group and the sham-operated group.
 | Fig. 2Mechanical withdrawal threshold of post-treatment groups on the 7th day after partial sciatic nerve ligation (pSNL). Sham, NS, and Olanzapine indicate sham-operation + vehicle (normal saline), pSNL-operation + vehicle (normal saline), and pSNL-operation + olanzapine (10 mg/kg) groups, respectively. Median thresholds are indicated with horizontal bars. The vertical bars indicate the range and horizontal boundaries of the boxes represent the first and third quartiles. *P < 0.05 vs. Sham-operation group.
|
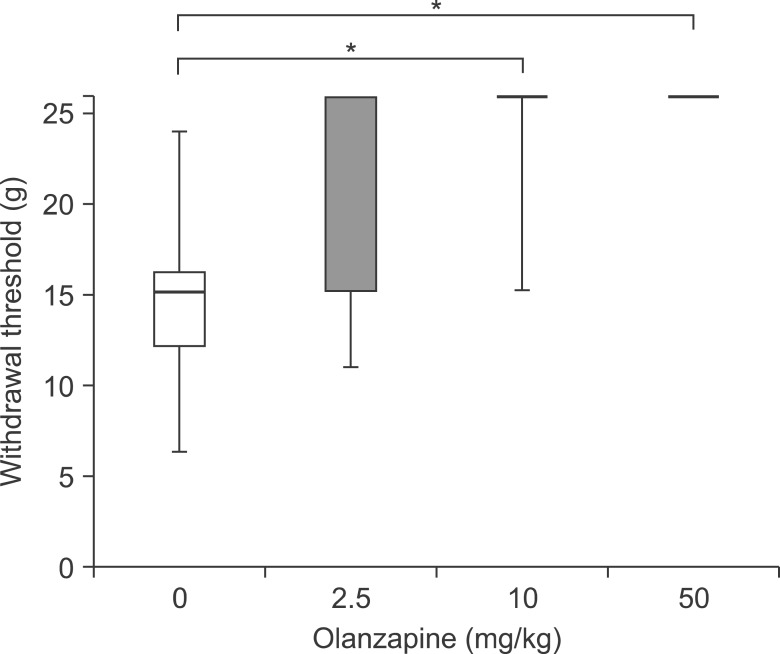
In the dose-dependency study, the median withdrawal thresholds of the 10 mg/kg and 50 mg/kg olanzapine groups were higher than that of the normal saline group. However, there was no significant difference between the withdrawal threshold of the 2.5 mg/kg olanzapine group and that of the normal saline group. Fig. 3 summarizes the median withdrawal threshold in the post-treatment studies.
2. Immunohistochemistry
Typical Iba-1 staining of the ipsilateral dorsal horn of the lumbar spinal cord is shown in Fig. 4. No significant differences in the density of Iba-1 staining were found between the olanzapine and normal saline groups in pretreatment and post-treatment experiments (Fig. 5). The densities of Iba-1 staining in the olanzapine and normal saline groups were higher than those of the sham-operated groups in the dorsal horn in the ipsilateral side of lumbar spinal cord.
 | Fig. 4Typical Iba-1 staining of the pre- and post-treatment groups in the ipsilateral dorsal horn of the lumbar spinal cord (L5). Sham, NS, and Olanza indicate sham-operation + vehicle (normal saline), partial sciatic nerve ligation (pSNL) + vehicle, and pSNL + olanzapine (10 mg/kg) groups, respectively. Scale bar = 100 µm.
|
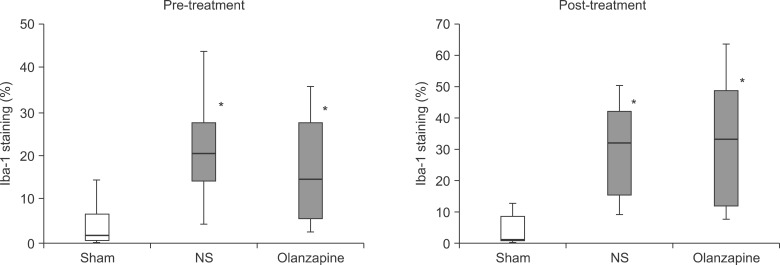 | Fig. 5Percentage of Iba-1-immunoreactive area of the pre- and post-treatment groups in the ipsilateral dorsal horn of the lumbar spinal cord (L5). Sham, NS, and Olanzapine indicate sham-operation + vehicle (normal saline), partial sciatic nerve ligation (pSNL) + vehicle (normal saline), and pSNL + olanzapine (10 mg/kg) groups, respectively. *P < 0.05 vs. Sham-operation + vehicle (normal saline) group.
|
Go to :
DISCUSSION
Intraperitoneal administration of 10 mg/kg olanzapine inhibited the development of allodynia in the rat partial sciatic nerve ligation model. The effects were observed in cases of both pre-treatment and post-treatment with olanzapine. In the post-treatment study, the anti-allodynic effect of olanzapine was dose-dependent; however, a ceiling effect and strong catalepsies were observed at the maximum dose (50 mg/kg). Contrary to our expectations, olanzapine-induced inhibition of microglia activities was not identified by Iba-1 staining in the ipsilateral dorsal horn of the lumbar spinal cord.
Olanzapine is an atypical antipsychotic that was released in the United States in 1996 [23]. In 2001, it was reported that olanzapine decreased pain symptoms in two patients with fibromyalgia [10]. To our knowledge, this was the first clinical report of the antinociceptive effects of olanzapine. To date, olanzapine is known to have exhibited treatment effects in headaches [12], cancer pain [11], and chronic pain after traffic accidents [13]. In a basic research study by using mouse tail-flick assay, olanzapine was reported to exert its antinociceptive properties on the basis of its alpha-adrenergic effects [9]. Another animal study reported that dopamine 1 and 2 receptor activity might also be relevant to the antinociceptive effects [24]. A recent animal study showed that olanzapine inhibited thermal hyperalgesia 1 h after in a sciatic nerve ligation model [16]. Previous animal studies have focused on the effects of olanzapine immediately after its administration; however, our aim in the present study was to evaluate the preventive effects of olanzapine in the development of allodynia after nerve injuries. Our novel finding is that olanzapine attenuated mechanical allodynia of Seltzer model rats at 1 week after it had been injected.
The half-life of olanzapine (single oral dose of 6 mg/kg) in plasma and the brain were reported to be 2.5 h and 5.1 h, respectively [25]. Therefore, olanzapine in plasma and nerve tissue was considered to be undetectable at 7 days after injection. Why did olanzapine attenuate mechanical allodynia in the present study? We think there are two possible answers. Olanzapine has been reported to increase cerebral cortex allopregnanolone and serum corticosterone levels in rats [26]. Allopregnanolone, a neurosteroid, reduced cell death, gliosis, and functional deficit after traumatic brain injury [27]. In mechanical and chemical nerve injury models, allopregnanolone has shown protective effects [2829]. So, olanzapine might repair the nerve damage induced by the ligation via neurosteroid production and/or a high level of corticosterone. The other possibility is that olanzapine might inhibit initial formation or intensification of supra-spinal pain perception. The spinal cord has been recognized as an important structure involved in the development of allodynia. However, the thalamus, anterior cingulate cortex (ACC), central nucleus of the amygdala (CeA), and descending inhibitory systems are also reported to be related to the development of allodynia [30]. Olanzapine is absorbed from plasma and accumulated in the brain [31]. If these supra-spinal regions are the main targets of olanzapine, pathological changes in the spinal cord must be small. This second hypothesis might agree with the result of Iba-1 staining in the present study.
Our study has some limitations. First, antinociceptive effects in the early period were not evaluated because of the catalepsy. Second, thermal allodynia was not measured in the present study. Therefore, our data are not directly comparable with previous data. We preferred to investigate mechanical allodynia because mechanical hyperalgesia was reported to occur more than thermal hyperalgesia in clinical situations [32]. Third, the time course of post-treatment effects was investigated at only 1 h after the nerve ligation. Therefore, the time limit of post-treatment is unknown and needs further validation. Fourth, effects of olanzapine in the supra-spinal area were not evaluated. Future studies are also needed to investigate the supraspinal area, for example ACC or CeA.
The present study showed that olanzapine attenuated mechanical allodynia in the rat Seltzer model even if it was injected after the nerve ligation. Since severe catalepsy, a side effect of olanzapine, was observed in the highest dose group, close medical observations and/or intensive care might be essential for its clinical use. However, our result indicates the possibility that olanzapine treatment might be useful for preventing the development of allodynia in patients with severe nerve injuries.
In conclusion, we found that olanzapine attenuated mechanical allodynia in the partial sciatic nerve ligation model. This effect was confirmed even with post-surgery administration of olanzapine. The anti-allodynic effect of olanzapine increased in a dose-dependent manner; however, a ceiling effect and catalepsy risks were observed at the largest dose. Since microglial activity of the ipsilateral dorsal horn of the lumbar spinal cord was not significantly affected by olanzapine, the responsible sites and mechanisms of the anti-allodynic effect require further analysis.
Go to :
 XML Download
XML Download