

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Chronic low back pain (CLBP) is associated with many aspects of a poor quality of life [1]. Insomnia is becoming increasingly recognized as a clinically important symptom in patients with CLBP [2]. Recent studies have reported that self-reported sleep disturbance affects up to 55% of people with CLBP [3,4,5].
Most often, insomnia is defined by the presence of an individual's report of difficulty with sleep [6]. Insomnia is associated with reduced sleep duration and quality, increased time to fall asleep, poor daytime function, and greater sleep dissatisfaction and distress [7]. Because insomnia has been shown to have negative effects on pain, mood, and physical functioning, it may also negatively affect the clinical outcomes of patients with CLBP [1]. The treatment of insomnia or depression may result in positive outcomes of CLBP [8]. However, pain clinics do not normally have the resources or expertise to provide a detailed sleep assessment for CLBP patients complaining of insomnia. Unfortunately, there have not been any published studies detailing the prevalence and severity of insomnia and/or factors associated with insomnia in CLBP using a large database in Korea.
The Insomnia Severity Index (ISI) is a brief instrument which measures patients' perceptions of their insomnia and the levels of severity [9]. The Korean version of the ISI has shown good psychometric properties, including good convergent validity, discriminate validity and test-retest reliability [10]. Since 2012, we have collected the ISI data in pain patients for the purpose of clinical audits.
The primary aim of this retrospective study is to determine the risk factors associated with clinical insomnia based on ISI scores in CLBP patients at a university hospital in Korea.
Go to : 
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Severance Hospital, and a written informed consent was waived. The sample population in this study was defined as CLBP patients who received treatment for their pain and completed the ISI between June of 2012 and June of 2013 at our outpatient clinic. CLBP was defined as pain, muscle tension or stiffness localized below the costal margin and above the inferior gluteal folds, with or without leg pain (sciatica). Chronicity was established by the persistence of pain beyond 12 weeks of symptoms. We excluded patients suffering from current infectious diseases, cancer, and psychiatric or neurologic disorders, which are known to affect sleep. Patients who reported that their insomnia predated the onset of back pain by more than 1 month and who were diagnosed with obstructive sleep apnea or peripheral neuropathy were also excluded.
The prevalence and severity of insomnia were assessed using the ISI data, which was recorded during an interview upon the first visit. The ISI consists of seven items which assess the following: the severity of sleep onset and sleep maintenance difficulties, satisfaction with one's current sleep pattern, the degree of interference with normal daily functioning, the degree of impairment attributable to sleep problems, and the degree of distress or concern caused by the sleep problems. Each compartment is graded on a five-point scale (0 to 4), and the global score ranges from 0 to 28 with higher scores indicative of more severe insomnia. Following the recommended score interpretation guidelines [9], a global score of 0-7 indicates "no clinically significant insomnia," 8-14 "sub-threshold insomnia," 15-21 "moderate clinical insomnia," and 22-28 "severe clinical insomnia." For the purpose of this study, clinical insomnia was defined as cases with a score higher than 15 on the ISI scale. Additional patient data that was collected includes age, gender, body mass index (BMI), duration of pain, pain score measured on a 0 to 10 numeric rating scale (NRS), the presence of leg pain, a previous spine surgery history, comorbid musculoskeletal pain conditions (musculoskeletal pain other than low back pain), symptoms suggesting neuropathic pain (patient-reported symptoms including dysesthesia or allodynia, burning or coldness, pins and needles sensations, numbness and itching, except for the low back region), and levels of anxiety and depression assessed by the 14 items on the Hospital Anxiety and Depression Scale (HADS) [11]. These 14 items, scored on a scale of 0 to 3 in each case, measure the degree of anxiety (seven items) and depression (seven items). Thus, the two subscales range from 0 to 21, with higher scores indicating an increased likelihood of an anxiety or depressive disorder being present. The cut-off value for the identification of suspected cases is generally considered to be 8 out of 21 points [11].
1. Statistical analysis
Continuous variables are shown as the mean ± standard deviation (SD), and categorical variables are shown as numbers (percentages). Logistic regression was used to compute crude odds ratios (ORs) with 95% confidence intervals (CIs) for variables associated with clinical insomnia (≥ 15 of the ISI score). The variables used for analysis included demographic data (age, gender, BMI), a history of hypertension or diabetes mellitus, and duration of pain (< 1 year or ≥ 1 year), pain score (< 7 NRS or ≥ 7 NRS), the presence of leg pain, previous spine surgery history, comorbid musculoskeletal pain, neuropathic pain components, and anxiety and depression (< 8 HADS or ≥ 8 HADS). Variables with a P value of less than 0.05 were included in the multivariate logistic regression analysis which estimated adjusted ORs with 95% CIs. Statistical analysis was performed with the Statistical Package for Social Sciences (SPSS, version 18.0; SPSS Inc., Chicago, IL, USA). Values of P < 0.05 were considered as statistically significant.
Go to :
RESULTS
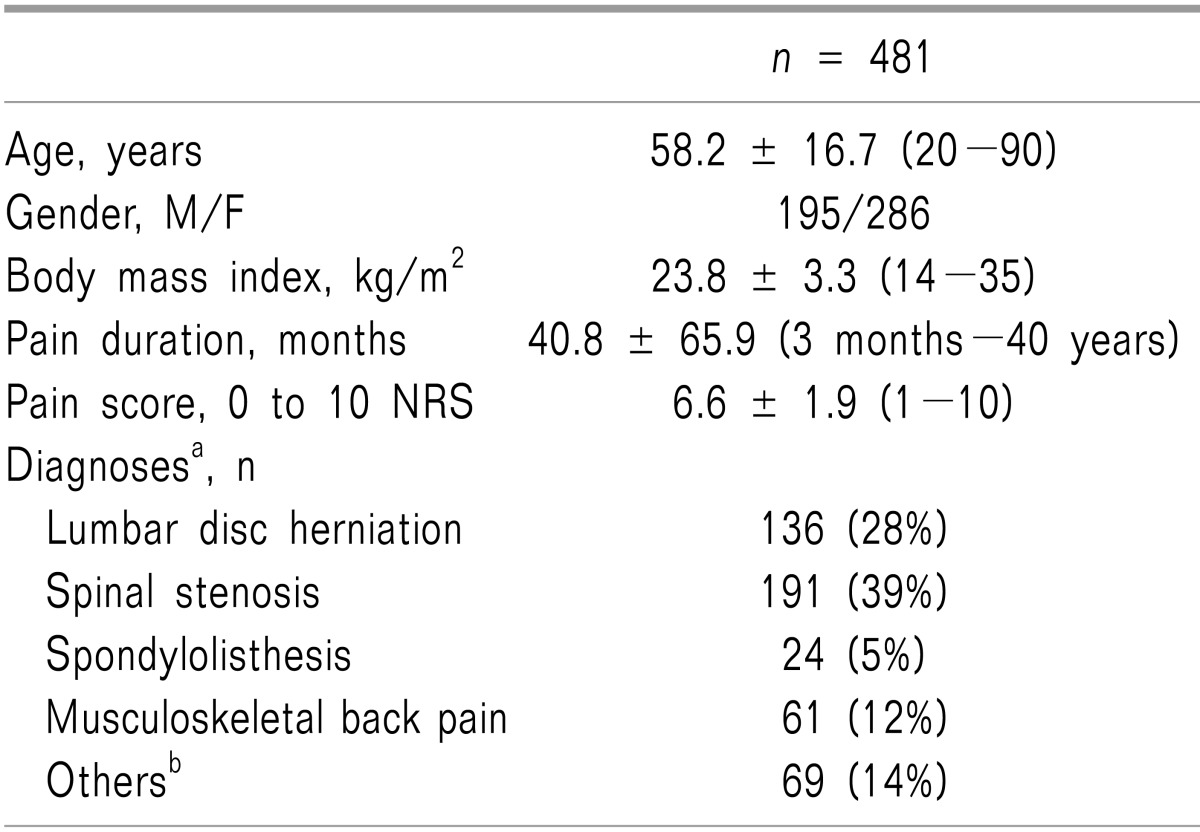
A total of 481 patients with CLBP satisfied the study inclusion criteria and were included in the analyses. The patients' demographics and CLBP characteristics are shown in Table 1. Most of the patients suffered from mechanical back pain, including lumbar disc herniation (28%) and spinal stenosis (39%).
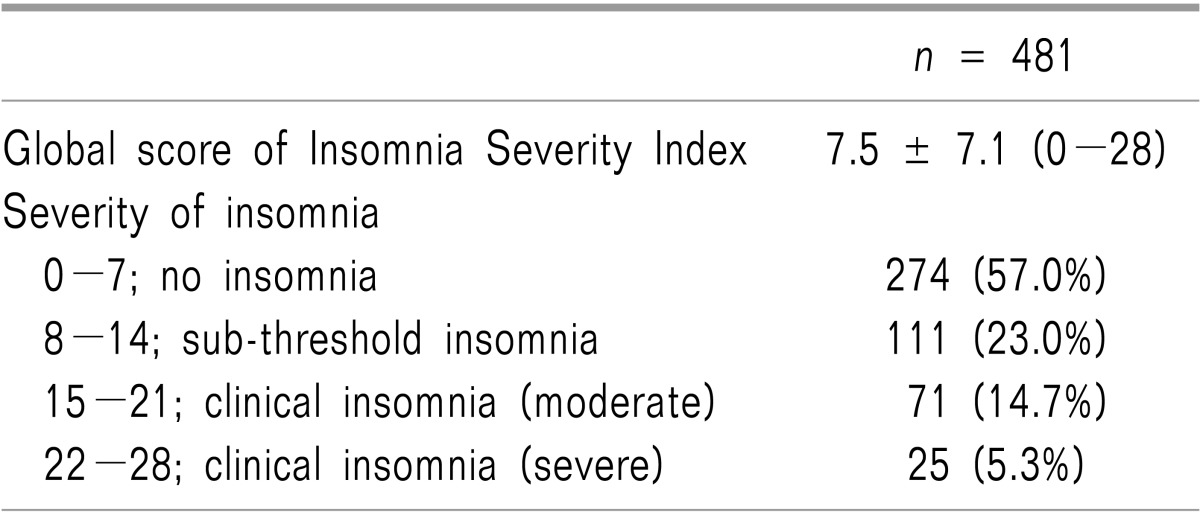
The mean global ISI score was 7.5 with a wide variation, and 43% of patients reported mild to severe insomnia (ISI score ≥ 8) after the development of back pain. Clinical insomnia of a moderate to severe severity level as measured by the ISI was found in 20% of patients (Table 2).
In the univariate analysis, we found that a high pain score with NRS ≥ 7, the presence of comorbid musculoskeletal pain, the presence of neuropathic pain symptoms, and high levels of anxiety and depression with HADS ≥ 8 were significantly associated with clinical insomnia (Table 3). The multivariate logistic regression analysis revealed that a high pain score with NRS ≥ 7, the presence of comorbid musculoskeletal pain, the presence of neuropathic pain symptoms, and high levels of depression with HADS ≥ 8 were significantly associated with clinical insomnia in our study population (Table 3). Among the aforementioned findings, the presence of comorbid musculoskeletal pain other than back pain was the strongest determinant, with the highest odds ratio of 8.074 (95% CI 4.250 to 15.339) for predicting clinical insomnia.
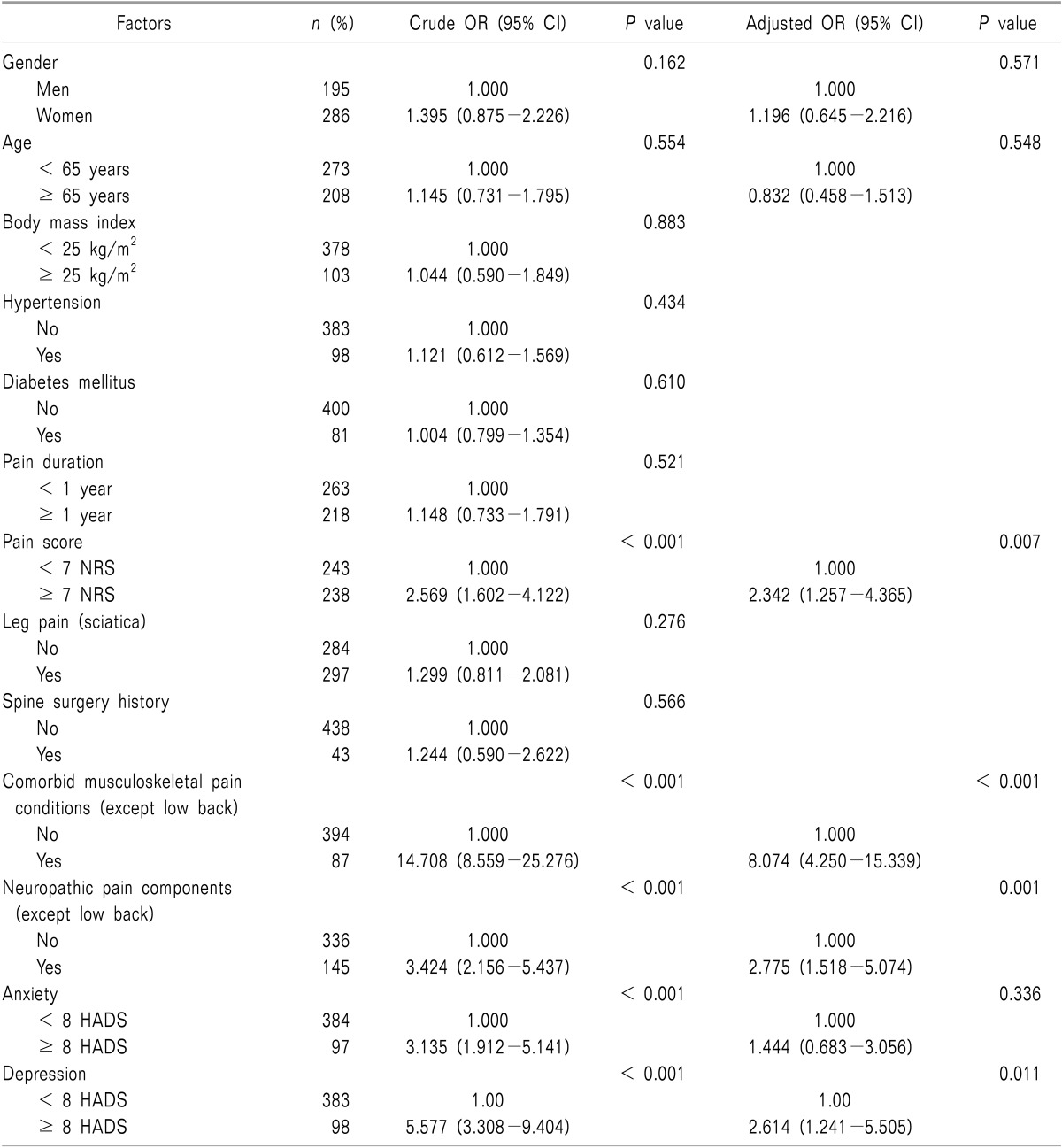
Table 3
Factors Associated with Clinical Insomnia (≥ 15 Insomnia Severity Index Score) in Chronic Low Back Pain: Results of the Logistic Regression Analysis
Significant variables (P < 0.05) in univariate analysis were selected for multivariate analysis. Age and gender were included in the multivariate analysis because these are identified demographic risk factors for insomnia in the general population [6]. OR: odds ratio, CI: confidence interval, NRS: numeric rating scale, HADS: Hospital Anxiety and Depression Scale.
![]()
Go to :
DISCUSSION
In the present study, our finding confirmed that insomnia is not uncommon in CLBP patients. We found that high pain intensity, the presence of comorbid musculoskeletal pain and neuropathic pain components, and the depression level were strongly associated with clinical insomnia in this population.
The ISI was used in the current study to determine the presence or absence of clinical insomnia. Twenty percent of patients in this study were suggestive of clinically significant insomnia (ISI ≥ 15). This proportion is approximately two times lower than the percentages of 44% to 53% from two previous studies involving European CLBP patients [3,4]. These two studies were conducted with small populations of less than 100 patients. The sample size, clinical setting and cultural differences may account for the discrepancy in the prevalence of clinical insomnia. However, the prevalence of insomnia (ISI ≥ 8) based on a subjective measure using the ISI in CLBP in this study was 43%. This prevalence is higher by approximately fivefold compared to a large cohort study in a general Asian population without CLBP which included Koreans [12].
In the present study, comorbid musculoskeletal pain other than low back pain was revealed to be, among various factors, the strongest risk factor for insomnia in CLBP patients. Although all patients reported low back pain as a chief complaint in this study, nearly 20% of patients complained of comorbid musculoskeletal pain at sites such as the neck, shoulders, arms, and joints, which may require medical attention. Instances of chronic musculoskeletal pain in the neck [13], shoulder [14], or knee joint [15] were closely linked to insomnia in previous studies. Patients with musculoskeletal chronic pain have an increased risk of poor mental health and a diminished quality of life [16]. One interesting study recently showed that the number of pain sites was a strong independent predictor of an individual's lower ability to work, indicating an impairment of social functioning [17]. Also, patients who present in primary care with multiple areas of regional pain have characteristics similar to those associated with chronic widespread pain and fibromyalgia [18]. Chronic pain sufferers generally appear to focus on the area that is most intense or that causes the greatest functional limitation. Other bodily pains seem small in contrast and are deemphasized when the patient initially describes the nature and locations of their complaints. However, an initial single site of chronic pain may cause central sensitization, thereby increasing the risk of experiencing pain in other body regions. Collectively, our study suggests that CLBP patients with comorbid multiple pain sites are highly susceptible to developing insomnia.
Similar to our study, most previous studies consistently reported that high pain intensity is significantly associated with insomnia in CLBP patients [3,4,5]. Marin et al. reported that there was a significant relationship between pain and sleep, with a 55% increase in the proportion of patients reporting restless or light sleep after the onset of pain [5]. Also, a bidirectional relationship between pain and sleep was reportedly associated with CLBP [19]. A disrupted sleep cycle can exacerbate pain, creating a vicious cycle in which insomnia caused by pain further aggravates the pain.
In this study, 30% of CLBP patients reported symptoms suggesting neuropathic pain other than the lower back. This result is similar to that of a large cohort study [1]. On the other hand, we found no significant relationship between leg pain (sciatica) which may be caused by nerve root compression or irritation and insomnia. This indicates that the central mechanism of neuropathic pain may predominantly affect insomnia rather than a peripheral mechanism acting on an affected spinal nerve, although causes of neuropathic pain other than lower back could not be clearly determined in this study. Recent animal studies also demonstrated that neuropathic pain-like stimuli suppress the GABAergic transmission with increased GABA (γ-aminobutyric acid) transporters located on activated astrocytes in the cingulate cortex related to insomnia [20,21].
Centrally mediated symptoms such as anxiety, depression and sleep disturbance are frequently observed in chronic pain conditions [19]. In a univariate analysis, both a high level of anxiety and a high level of depression (HADS 8 ≥ in both cases) were significantly associated with clinical insomnia in CLBP, although only depression remained an independent factor associated with clinical insomnia after adjusting for other factors in this study. Approximately 40% of adults with insomnia have a diagnosable psychiatric disorder, in most cases depression and/or anxiety, which may be a consequence of sleep deprivation as well as a risk factor for its development [22]. Also, Artner et al. reported a 54% prevalence of a psychological disorder in CLBP patients despite their receiving multimodal pain management [23]. Moreover, Chiu et al. demonstrated that depression and sleep disturbance are independently associated with a reduced pain threshold [24]. Thus, CLBP patients with depression are highly susceptible to insomnia, and insomnia may be considered an independent symptom when devising treatment strategies for this subgroup, which is more prone to poor clinical outcomes.
Another key aspect of this study is the set of patient demographic factors, may not relatively affect insomnia in CLBP compared to other clinical characteristics. In the general population, age and gender are the most clearly identified demographic risk factors for insomnia, with an increased prevalence in women and older adults [6]. However, these demographic factors appear to be modest during insomnia in CLBP patients. In several studies dealing with insomnia in CLBP and in our study, no relationship between insomnia and age, gender, or BMI has been reported [3,4,5].
This study has several limitations. First, the study was conducted in a single clinical setting including a selected study population with a homogeneous racial background. Secondly, our findings are cross-sectional in nature; thus, a causal relationship between insomnia and current pain or sleep treatments cannot be determined definitely. Also, the ISI does not contain parameters for measuring the frequency and duration of insomnia, or medication use, which may play unknown roles in determining the severity of insomnia. Finally, this study was based on a subjective assessment of insomnia. Although the ISI has obvious advantages over other available measurements of insomnia in busy clinical settings, it appears to be important to incorporate an objective assessment of sleep with polysomnographic or actigraphic evidence [25].
In conclusion, we have demonstrated that CLBP patients who have high pain intensity, comorbid musculoskeletal pain and neuropathic pain components, and high level of depression are strongly linked to clinical insomnia. Insomnia should be addressed as an integral part of pain management in CLBP patients with these risk factors, especially in patients suffering from CLBP with comorbid musculoskeletal pain.
Go to :
 XML Download
XML Download