

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
As examples of efficacy, a single-dose combination of methylprednisolone and etoricoxib was demonstrated to reduce both postoperative pain and nausea following laparoscopic cholecystectomy [1], an example of visceral nociceptive pain; and preoperative treatment with dexamethasone and dipyrone but not dipyrone alone prevented sensory hypersensitivity following third molar extraction [2], an example of neuropathic pain.
Minor orthopedic procedures are examples of somatic nociceptive pain and are frequently scheduled as outpatient surgery. Therefore, it is commanding that the patient can get home in the same day with efficient analgesia along with no adverse effects, and non-opioid drugs combinations represent a good alternative for safety. Because epidural dexamethasone has been previously demonstrated to be competent after orthopedic surgeries [3,4,5] or back pain [6], we evaluated different intravenous (IV) non-narcotic analgesics combined to epidural dexamethasone under spinal bupivacaine anesthesia in patients scheduled to minor orthopedic surgeries.
Go to : 
MATERIALS AND METHODS
The Ethical Committee of The Teaching Hospital of the School of Medicine of Ribeirão Preto from the University of São Paulo approved this protocol (Protocol number 3420/2005). After gaining the subjects approval and written informed consent, 91 ASA status I and II patients undergoing minor orthopedic surgery were computer randomized to one of seven groups (n = 13) and prospectively evaluated using a placebo-controlled double-blind design to examine analgesia and perioperative adverse effects. The concept of a visual analogue scale (VAS), which consisted of a 10-cm line with 0 equaling "no pain at all" and 10 equaling "the worst possible pain" was introduced to the subjects before surgery. Exclusion criteria included diabetes and psychiatric disease.
The patients were premedicated with 0.05-0.1 mg/kg IV midazolam immediately before going to the operating room (OR). Hydration consisted of a rapid infusion of 10 ml/kg lactate solution before surgery and 10 ml/kg/hour after spinal anesthesia. Combined spinal/epidural anesthesia was performed in the operating room at the L2-L3 (epidural) and L3-L4 (spinal) interspaces in the sitting position. One anesthesiologist prepared the test drugs, while a different one performed the spinal/epidural punctures. The epidural test drug was either saline or 10 mg dexamethasone diluted in saline (to a final volume of 10 ml) injected as a bolus. Just after epidural drugs administration, spinal bupivacaine was injected at 1 ml per 7 seconds through a 25-gauge spinal needle (Table 1). All patients received 15 mg hyperbaric bupivacaine. Patients were placed supine immediately after the spinal/epidural punctures. Subsequently, the IV test drugs (1 gr dipyrone or 40 mg paracoxibe) administered are described in Table 1, and were also injected blindly, diluted in saline to a final 10-ml volume.
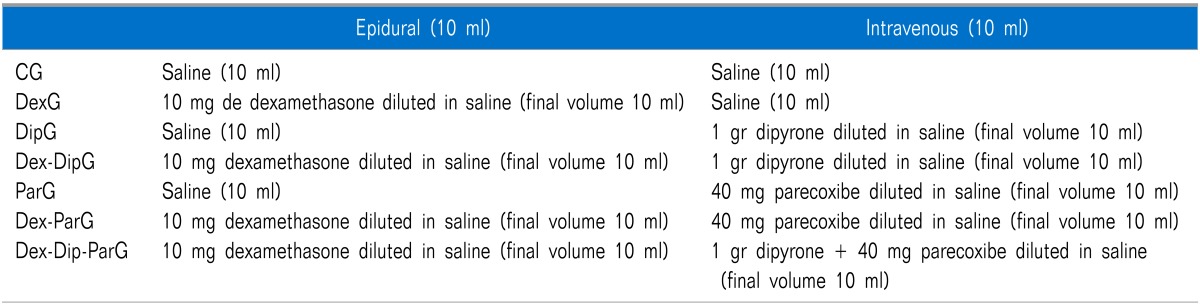
Patients were located at seven groups: 1) Patients from the Control group (CG) received epidural and IV saline as the test drugs. 2) Patients from the Dexamethasone group (DexG) received epidural dexamethasone and IV saline. 3) Patients from the Dipyrone group (DipG) received epidural saline and IV dipyrone. 4) Patients from the Dexamethasone-Dipyrone group (Dex-DipG) received epidural dexamethasone and IV dipyrone. 5) Patients from the Parecoxibe group (ParG) received epidural saline and IV parecoxibe. 6) Patients from the Dexamethasone Parecoxibe group (Dex-ParG) received epidural dexamethasone and IV parecoxibe. 7) Finally, patients from the Dex-Dip-ParG received epidural dexamethasone and IV combination of dipyrone plus parecoxibe. Further IV midazolam was given consistent with the anesthesiologist's perceptiveness, based on patient's wellbeing.
Intraoperative sensory loss valuation comprised the pinprick test at 5- and 10-min after the spinal anesthesia. Blood pressure was supervised non-invasively every 5 min all over surgery, and heart rate and oxyhemoglobin saturation were continuously overseen during the progression of the surgery. A decrease in mean arterial pressure greater than 15% below pre-anesthetic baseline was treated with incremental doses of ephedrine. Diminutions in heart rate below 50 bpm were handled with atropine, 0.25 mg IV, along with the anesthesiologist's judgment. Intraoperative nausea was scored by the patient using the 10 cm VAS. The numbers of patients with nausea (of any degree) or vomiting at any intraoperative time were noted. Nausea greater than 2/10 at any time or vomiting during the study was handled with 8 mg IV ondansetron, if necessary. For patients with more than one episode of nausea, the VAS scores were averaged.
Postoperative evaluation included duration of motor block (determined from spinal anesthesia until time to reach a Bromage 2 score [7], pain scores, the occurrence of fever, wound infection and wound dehiscence, heal at the 7th day, or any other adverse effects. Nausea and vomiting were assessed intraoperatively and at 24-hour after the spinal puncture by the same anesthesiologist, eyeless to the treatment.
Pain was assessed at the time of first rescue analgesic and 24 hours after the spinal puncture by the anesthesiologist who was blind to the study conduction, and patients were allowed to receive rescue analgesics at the time requested as IV 50 mg ketoprofen was accessible at 4-hour-interval. The duration of successful analgesia was determined as the time from the epidural puncture to the patient's first demand for analgesics either in the recovery room or infirmary, documented in minutes. The VAS at the time of first rescue analgesic was measured by means of 10-cm VAS. The 24-hour VAS pain score and VAS for nausea signified the patient's overall sense of the 24-hour following epidural injection.
1. Statistical analysis
The power of the study was based upon pilot data. We hypothesized that 10 mg of epidural dexamethasone would amplify the time to first rescue analgesic by 100% compared to the CG in the population considered, and estimated that the addition of IV drug would further increase the time to first rescue analgesic by 20% compared to the Dexamethasone group. If a standard deviation was estimated, an 80% and an alpha value of 0.05, these suppositions would require at least 10 patients in each group.
The normality of the distributions was judged using the Shapiro-Wilk's test. Groups were compared for demographic data (i.e., age, weight and height) and duration of surgery by one-way ANOVA. Incidence of adverse events, gender, ASA status and adjuvant drug use were compared among groups by Chi-square corrected for multiple comparisons. P < 0.007 was considered significant (i.e., 0.05 divided by the number of groups). Blood pressure, heart rate, level of anesthesia (by pinprick test) and VAS scores were compared among groups by two-way ANOVA for repeated measures. Tukey analysis was utilized to decrease the probability of type I error. The time to first rescue analgesics and the analgesic consumption (mg) in 24 hours were compared using the Kruskal-Wallis on ranks followed by the Student-Newmans-Keuls test. P < 0.05 was considered significant. Data are expressed as means ± SD, unless otherwise identified.
Go to :
RESULTS
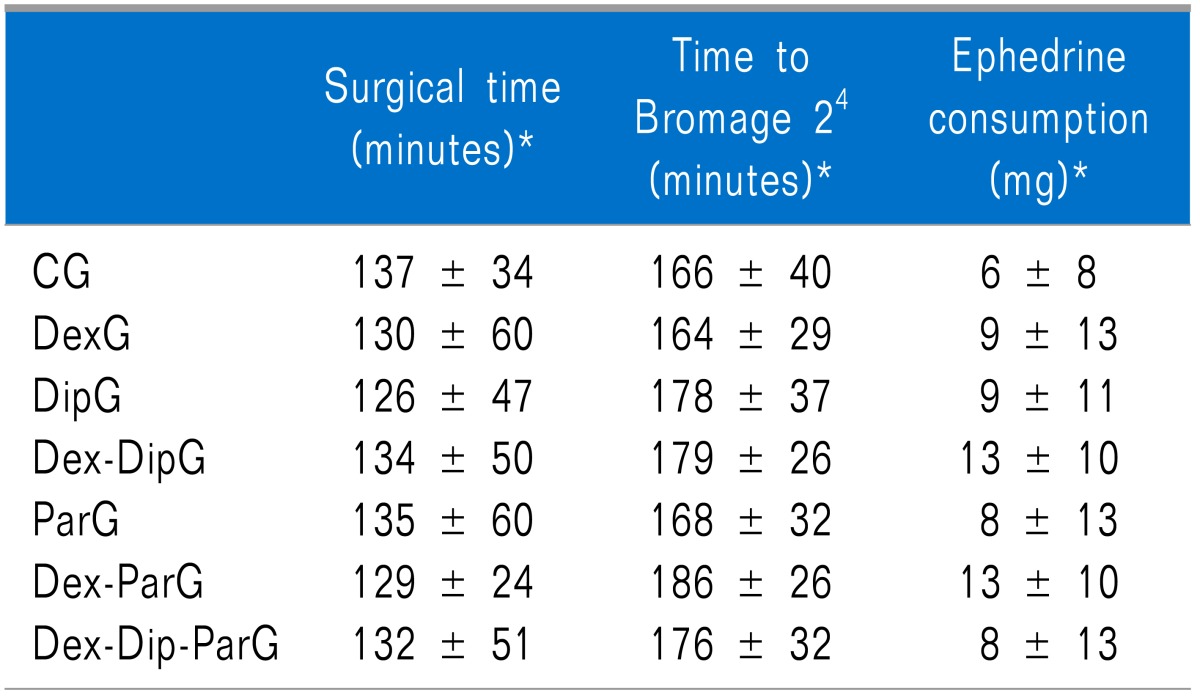
Eighty eight patients were evaluated. One patient from the CG, one from the DipG and one from the ParG were excluded due to incomplete data compilation. All patients underwent minor orthopedic surgeries (P > 0.05; Table 2). The groups showed no disparities regarding ASA status, gender, age, weight or height (P > 0.05, Table 3). The sensory level to pinprick at 5- and 10-min after the spinal puncture (P > 0.05; Table 4), surgical and anesthetic time, and intraoperative ephedrine consumption were similar among the groups (P > 0.05; Table 5). The intraoperative midazolam administration was also similar among the groups (2.5-5 mg, P > 0.05, data not shown).
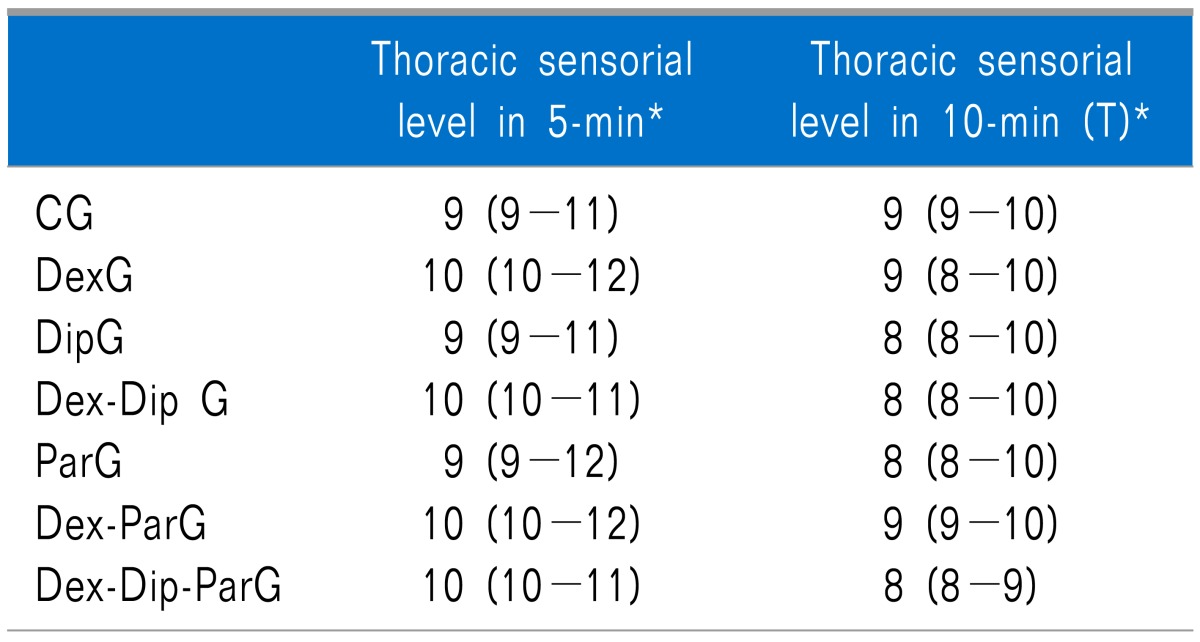
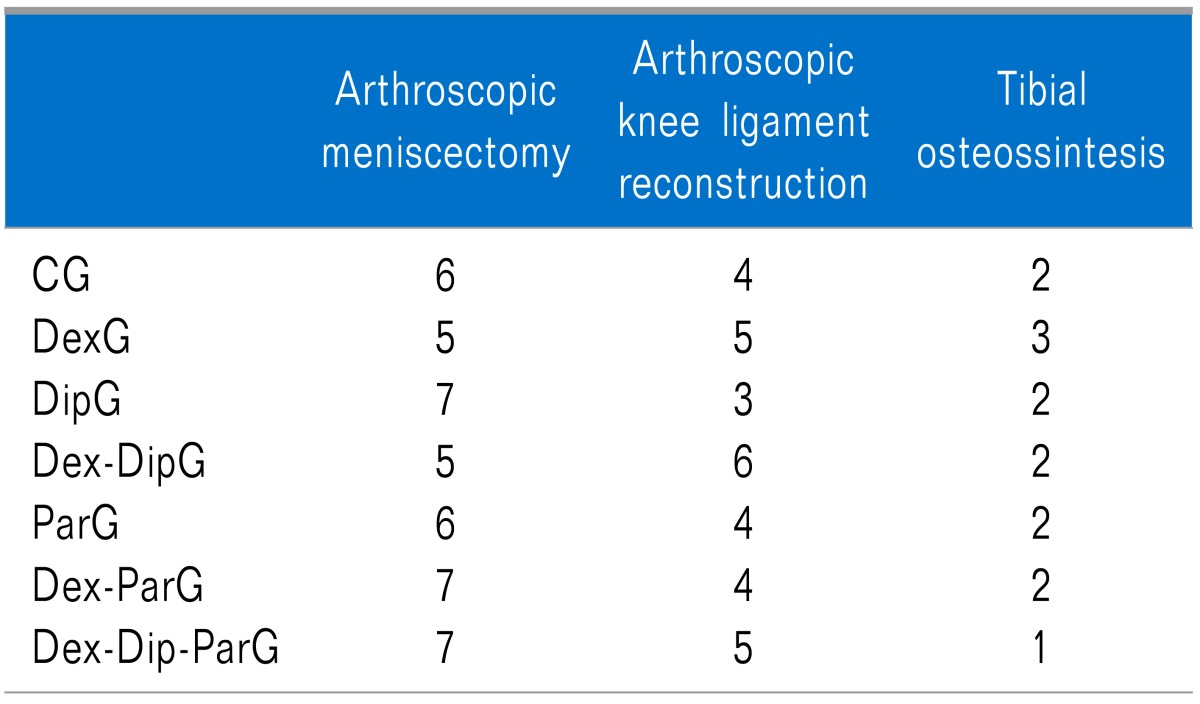
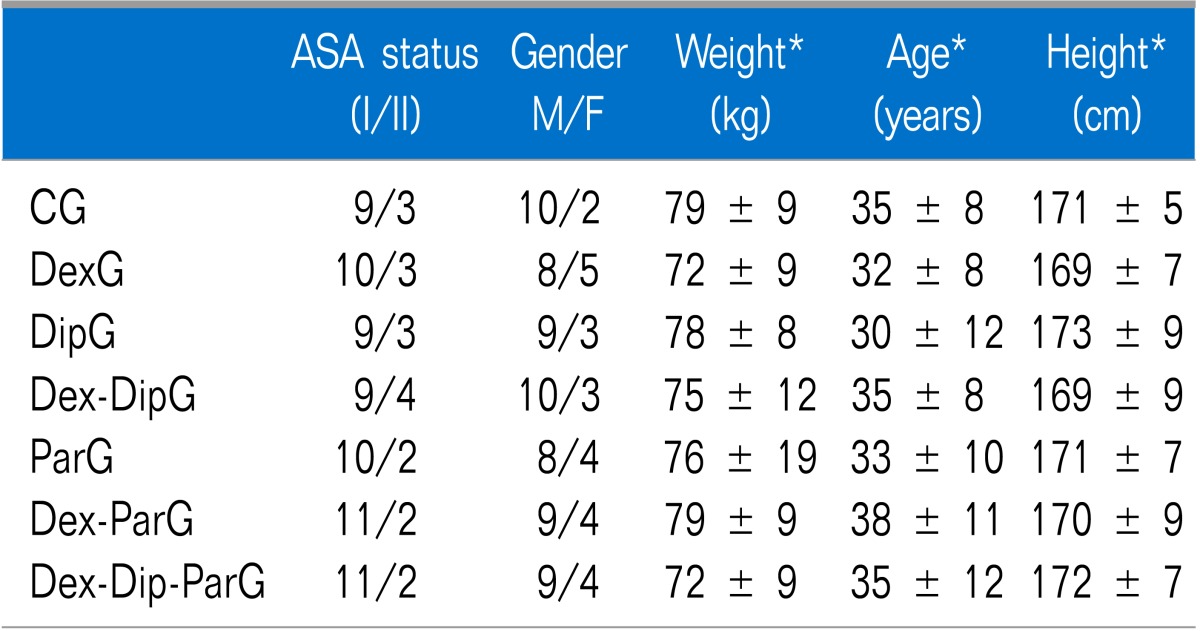
Table 4
Sensorial Level Evaluated by Pinprick at 5- and 10-Min after the Spinal Puncture. The Thoracic Dermathomes Varied from T1 to T12
P > 0,05. CG: control group, DipG: dipyrone group, DexG: dexamethasone group, Dex-DipG: dexamethasone-dipyrone group, ParG: parecoxib group, Dex-ParG: dexamethasone-parecoxibe group, Dex-Dip-ParG: dexamethasone-dipyrone-parecoxibe group, M: minutes. *Data expressed as median (25%-75% confident interval).
![]()
The postoperative data are exposed in Table 6. The pain VAS score at the time of first rescue analgesic medication was analogous among all groups (P > 0.05). The CG had the shorter period of time for first rescue analgesic since the epidural puncture (4 hours). The time to first rescue analgesic was similar to the DexG, DipG, ParG and Dex-ParG (7 hours; P > 0.05), even though longer when compared to the CG (P < 0.05), and shorter when compared to the Dex-DipG and to the Dex-Dip-ParG (17 hoours; P < 0.05), which were similar between them (P > 0.05). The time to first rescue analgesic was longer to the Dex-DipG and the Dex-Dip-ParG when compared to the CG (17 hours; 4 hours, respectively, P < 0.002). The number of rescue injections of IV ketoprofen (50 mg) in 24-hour evaluation was greater for the CG, compared to the others (P < 0.05). The analgesic consumption was similar to the DexG, DipG, ParG and Dex-ParG (P > 0.05), although greater when compared to the Dex-DipG and Dex-Dip-ParG (P < 0.05), which was similar between them (P > 0.05). The overall 24-hour pain felling was similar among all groups (P > 0.05).
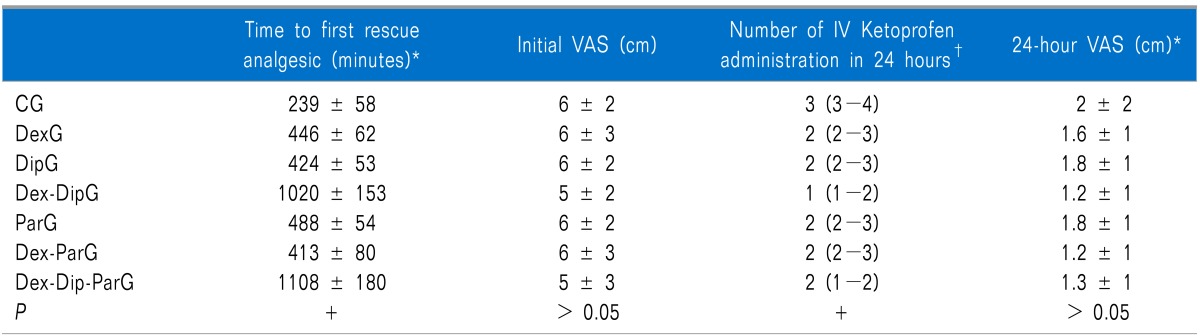
Table 6
Postoperative Pain Evaluation
CG: control group, DipG: dipyrone group, DexG: dexamethasone group, Dex-DipG: dexamethasone-dipyrone group, ParG: parecoxib group, Dex-ParG: dexamethasone-parecoxibe group, Dex-Dip-ParG: dexamethasone-dipyrone-parecoxibe group. +: CG<DexG (P < 0.05) = DipG = ParG = Dex-ParG < Dex-DipG = Dex-Dip-ParG (P < 0.002). *Data expressed as mean ± SD. †Data expressed as median (25%-75% confident interval).
![]()
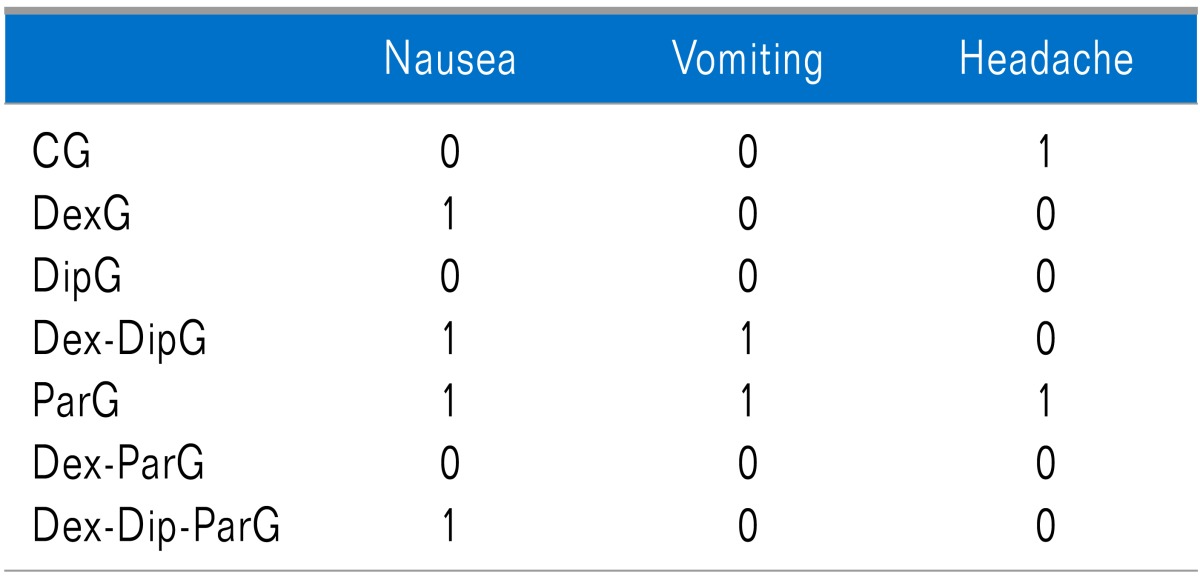
The occurrence of perioperative adverse effects in 24-hour observation was similar among groups (P > 0.05; Table 7). The occurrence of fever, wound infection and wound dehiscence was similar among all groups. In fact none of these adverse effects occurred. Healing at the 7th postoperative day post-surgery was similar among groups. Postoperatively, one patient from each of the following groups: DexG, Dex-DipG, ParG, Dex-Dip-ParG had complained of postoperative nausea, however only the patient from the ParG and the one from the Dex-DipG had vomited once after dinner; though no pharmacological treatment was mandatory. One patient from the CG and one from the ParG complained of transient headache. These patients preferred only to rest because of history of past headache. No other adverse effects were perceived.
Go to :
DISCUSSION
We revealed that epidural 10 mg dexamethasone resulted in similar analgesia to either IV 1 gr dipyrone alone or to IV 40 mg parecoxibe alone (7 hours); while the association of epidural dexamethasone and IV dipyrone resulted in enhanced analgesia (17 hours) in the population studied. Intriguingly, the association of IV parecoxibe to epidural dexamethasone had no gain to either drug alone in this current evaluation.
The reason for the epidural route of dexamethasone administration instead of the IV was based in its historically positive effect in orthopedics [4,5,6,7,8]. It may be acting at spinal sites by inducing the synthesis of the phospholipase-A2 inhibitory protein lipocortin [9]. The inhibition of phospholipase A-2 reduces prostaglandin and leukotriene synthesis, suppressing hyperalgesia associated to acute nociception during surgery. In addition, high levels of glucocorticoid receptor and mineralocorticoid receptor are co-localized in the substantia gelatinosa [10], suggesting that the pain pathways are strongly regulated by these receptors. Dexamethasone was also shown to downregulate cyclooxygenase (COX)-2 mRNA, an important step for its anti-inflammatory action [11]; to inhibit the Nox- (a subunit component of NADPH oxidase) dependent reactive oxygen production, to inhibit oxide nitric release and finally inhibit the inflammatory reaction of activated microglial cells [12], to up regulate the N-methyl-D-aspartate receptor subunit 2B expression in the spinal dorsal horn [13] and to induce inhibition of glutamatergic transmission [14].
Indeed, fifty years have elapsed since the first publication of epidural dexamethasone for pain relief [8], and it has been used for orthopedics [4,5,6,7], for other surgicals [15,16,17,18] or pain [8,19] procedures. The non-particulate dexamethasone is the routine steroid used in our Pain Center for the past 25 years. Recently it has been demonstrated to be no inferior compared to particulate steroids [20]. In fact, dexamethasone has particles significantly smaller than red blood cells, with the least tendency to aggregation, and the lowest density and reduced the risk of embolic infarcts. These characteristics transform this drug as one of the safest for epidural administration [21]. The epidural dexamethasone dose varied in the literature from 0.1 mg/kg in children 15 to 10 mg in adults [6,19]. In our study, the decision for the association of epidural dexamethasone to spinal bupivacaine was based on previous positive effects in different postoperative types of pain [4,5,6,7,15,16,17,18]. Postoperative pain can normally be classified as nociceptive somatic, 2) nociceptive visceral, and 3) neuropathic pain. As examples, steroids have been previously demonstrated to benefit the neuropathic pain [5,6,7,8] and the nociceptive visceral pain [15,16,17,18]. Another point in favor to the decision of epidural dexamethasone would be its benefit in reducing backache after lumbar epidural anaesthesia [22] and its protective in vitro effect over spinal bupivacaine neurotoxicity [23].
Customarily we combine epidural dexamethasone to spinal opioid analgesia for upgrading perioperative analgesia following major orthopedic operations. It was suggested that epidural bupivacaine-dexamethasone had almost the same analgesic potency as bupivacaine-fentanyl with opioid-sparing [15,16], produced antiemetic effects [16], decreased pain in the short term, abbreviated the length of stay after lumbar spinal surgery [7] and improved epidural methadone analgesia [19]. For the reason that intrathecal opioids are not the more proper analgesics for outpatient surgeries, other picks could be IV parecoxibe or IV dipyrone.
In this actual study, we evaluated postoperative pain after minor orthopedic surgeries, which is a representative of pure nociceptive somatic pain. Although dexamethasone's efficacy after neuropathic and visceral pain has been previously demonstrated, we found no benefit after epidural dexamethasone alone (DexG) over either IV dipyrone (DipG) or IV parecoxibe alone (ParG), as all groups (DexG, DipG and ParG) had 7 hours of analgesia. In addition, the combination of epidural dexamethasone and IV parecoxibe (Dex-Dip-ParG) also resulted in 7 hours of postoperative analgesia, demonstrating no benefit of this association.
Parecoxibe is a specific COX-2 inhibitor [24], with no effect on the spinal N-methyl-D-aspartate receptor subunit 2B [25], conversely from dexamethasone10. IV parecoxibe has been previously demonstrated to improve IV dexamethasone analgesia in outpatient anterior crucial ligament [26] and to result in 7 hours and 5 minutes of analgesia after orthopedic procedures [27], in accordance to our results (ParG). The lack of further analgesic effect of the Dex-ParG could be secondary to the minor tissue damage and smaller production of COX-2 in the patients evaluated, which would be even smaller secondarily to the inhibition of phospholipase A2 by dexamethasone, resulting in lesser central prostaglandin production. In this case, as central inhibition of COX is an important mechanism for IV parecoxibe [28], there would be not enough substrate for a clinical manifestation of analgesia. It seemed then, that dexamethasone and parecoxibe acted at the same final pain pathway, and were competitive. This competition would also occur at the periphery, as systemic effects of a single epidural dexamethasone injection could be demonstrated until the 7th day [29].
Interestingly, the association of epidural dexamethasone and IV dipyrone resulted in 17 hours of analgesia compared to 7 hours after each drug alone, suggesting a reciprocal enhancement of the final analgesic effect. In fact the results suggest at least summation of the analgesic effect of both drugs, exemplifying multimodal analgesia.
Active metabolites of dipyrone inhibit COX activity by sequestering radicals which initiate the catalytic activity of this enzyme or through the reduction of the oxidative states of the COX protein [30]. The active metabolites of the prodrug dipyrone could also inhibit COX-3 at the dorsal root ganglion [31] and represent a primary central mechanism by which dipyrone decrease pain and fever [32]. In addition, the metabolites arachidonoyl amides were positively tested for cannabis receptor binding type-1 and -2; suggesting that the endogenous cannabinoid system may play a role in the effects of dipyrone against pain [33].
Apart from COX-1, -2 and -3 inhibition and cannabis agonist, dipyrone causes antinociception by activating endogenous opioidergic circuits along the descending pain control system [34]. In rats, responses of dorsal spinal wide-dynamic range neurons to mechanical noxious stimulation were strongly inhibited by intravenous dipyrone, an effect abolished by naloxone into the periaqueductal gray matter, into the nucleus raphe magnus or by direct application onto the spinal cord [34]. Lastly, but not less important, the suggested teleantagonism was also demonstrated after dipyrone. Intrathecal glutamate, N-methyl-D-aspartate, or prostaglandin E-2 induced sensitization of the primary nociceptive neuron which was inhibited by peripheral dipyrone, a pharmacodynamic phenomenon referred to as teleantagonism [35].
Related to the adverse effects, none of the patients had serious complains. In this study, dipyrone and dexamethasone were used as part of the protocol. One of the points addressed was that fever was an adverse effect evaluated in the postoperative period, however, dipyrone is well known thermo regulator and dexamethasone has been demonstrated to alleviate temperature elevation, an effect attributed to the decrease of interleukin-6 levels [36]. However, none patients felt fever. As part of exclusion criteria, diabetes patients did not participate due to the possibility of peripheral neuropathy and interference with results, although it has been recently demonstrated that epidural steroid efficacy was independent of the presence of type-2 diabetes [37]. Although flushing is more common with epidural dexamethasone and in women, it seems innocuous and self-limiting [38] and was not evaluated.
In conclusion, the analgesia secondary to epidural dexamethasone was exacerbated by IV dipyrone, while no effects were observed by the addition of IV parecoxibe suggesting that dexamethasone and parecoxibe may have acted at the same final pain pathway, and were competitive, while dipyrone mechanisms of action summated to dexamethasone's ones.
Go to :
 XML Download
XML Download