

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Complex regional pain syndrome (CRPS) is a refractory pain disease that usually manifests after a minor injury [1]. CRPS is characterized by 4 categories of signs and symptoms: sensory change, vasomotor change, pseudomotor change, and motor change. The diagnosis of CRPS is based on examination of the presence of these signs and symptoms [2,3,4]. Since the diagnostic criteria for CRPS was established in the 1994 by International Association for the Study of Pain [5], several adjustments have been made by further studies, until the 2007 Budapest criteria was organized [2]. However, the Budapest criteria also have its weaknesses in that a simple dichotomous categorization method is not sufficient to examine interatient differences and identify the disease progress in a patient over the course of time [6,7]. In an effort to overcome these weaknesses, the CRPS severity score (CSS) was developed based on the Budapest criteria [8]. The CSS became a useful tool to compare the effect of treatment on a patient and to compare the severity of the disease among patients, which was not possible through the former dichotomous criteria. The CSS comprises a total of 17 items (8 items for patients' subjective symptoms and 9 items regarding the physical examination findings). Each checked item is counted as 1 point, and the total added score constitutes the CSS (Table 1).
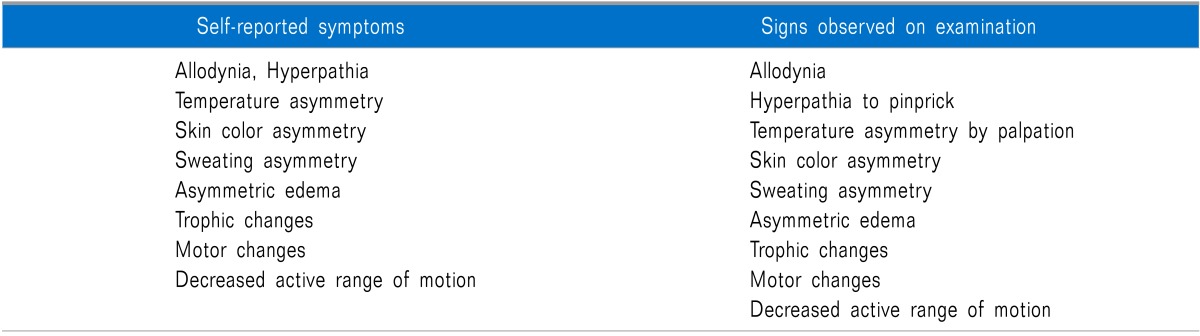
Table 1
Diagnostic Signs and Symptoms Included in the Complex Regional Pain Syndrome Severity Score [8]
![]()
Physicians make a diagnosis of CRPS by combining the patient's subjective symptoms and the objective signs. Hence, the objectivity of the diagnosis has been considered one of the most important factors to establish. To secure the objectivity of the diagnosis, several diagnostic criteria have been developed and a number of laboratory examinations have been used as complementary diagnostic tools. Infrared thermography (IRT) is a method for detecting abnormality by measuring the skin temperature. It has been widely used to complement the diagnostic process as it is noninvasive, user-friendly, and effective for visualizing the subjective pain. Skin temperature asymmetry greater than 1.0℃ is considered significant [8], but other researchers have also suggested different temperature standards, such as 0.6℃ [9] or 2.2℃ [10].
Nevertheless, there has been no research on whether the CSS and degree of skin temperature asymmetry are viable in reflecting the severity of the patient's subjective symptoms. Thus, we aimed to examine whether the CSS and degree of skin temperature asymmetry have any correlation with the patient's subjective pain.
Go to : 
MATERIALS AND METHODS
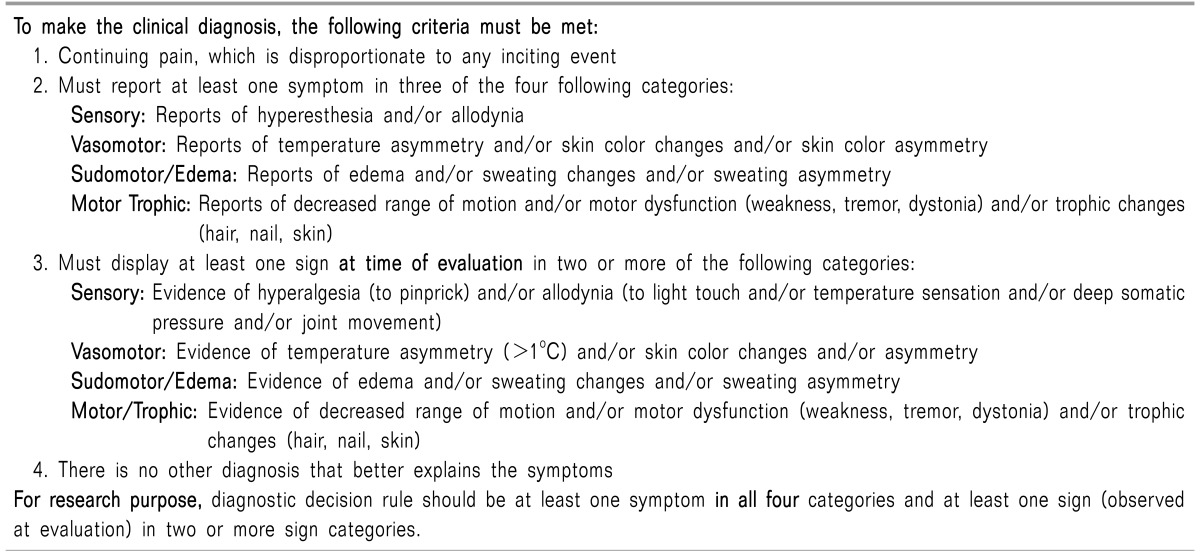
This study was approved by the institutional review board of the authors' affiliated organization (IRB NO: B-1312/230-114). The inclusion criteria was the patients who had visited our pain center from March 2010 to August 2013 and had been diagnosed with CRPS in the ipsilateral limb based on the Budapest research criteria (Table 2) [2]. Of these patients, any patient with a history of sympathetic neurolysis, who had received a sympathetic block or epidural block within 3 months of the hospital visit, who had been administered ointment on the injured area, or who was taking vasodilators was excluded from the subject pool. The CSS was assessed and an IRT was performed on the participants. The IRT was performed in accordance with the method established in a previous study [11]: the patient was placed in a closed examination room with a constant temperature of 23℃, blocked from external light and heat. After 20 minutes of adaptation to the room, the patient was positioned 1 m from the IRT equipment IRIS®-5000 (Medicore Co., Korea) in an upright position. We then took infrared images of the frontal, posterior and lateral areas of the affected limb, its symmetrical region on the other limb, and the sole (according to our needs).
For evaluation of the IRT images, the skin temperature of the area of the patients' most severe pain and the symmetrical area on the other limb were measured, and the ΔT was calculated. The CSS and visual analogue scale (VAS) scores were calculated as well. The VAS score was measured using a 10 cm-long tool and the range of the scale was from 0 with "no pain", to 10 with "the worst possible pain ever imagined". The ΔT was defined as follows.
For the statistical analysis, IBM SPSS statistics® version 17.0 (IBM Corporation, NY, USA) was used and a Shapiro-Wilk test was used to perform a normality test on the ΔT, CSS and VAS scores. In cases that showed abnormal distribution, Spearman's non-parametric correlation analysis was performed. The primary outcome was set as the correlation between the ΔT and VAS score, and the secondary outcome was set as the correlation between the CSS and VAS score. P values of less than 0.05 were determined to be significant.
Go to :
RESULTS
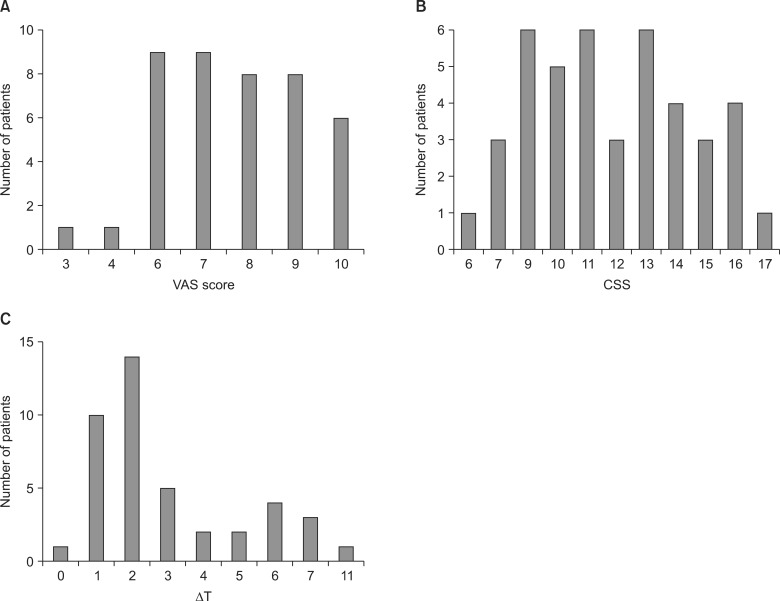
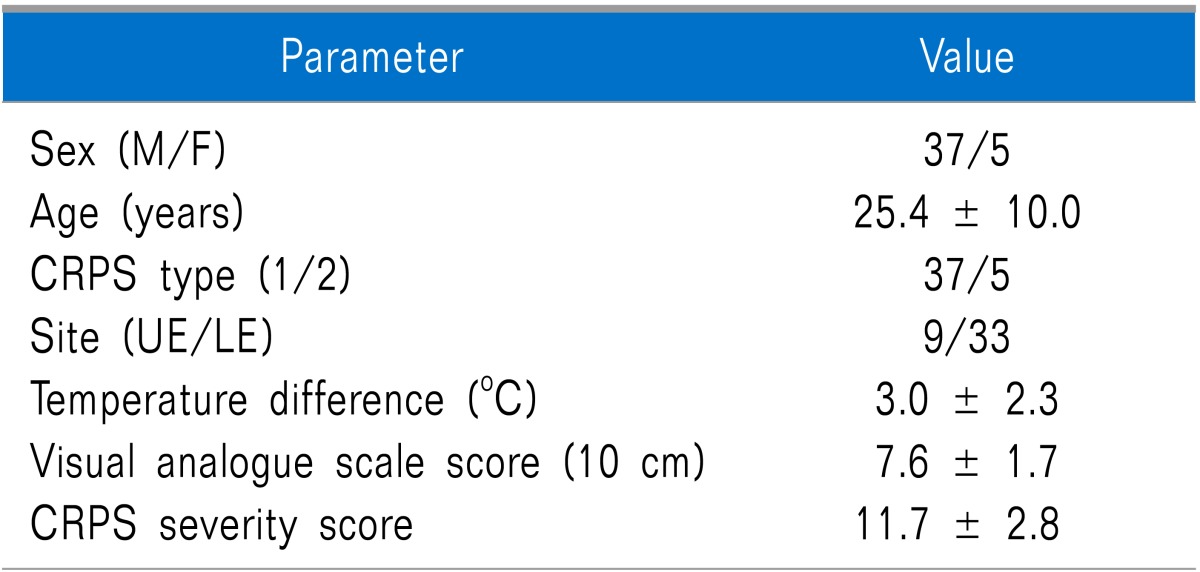
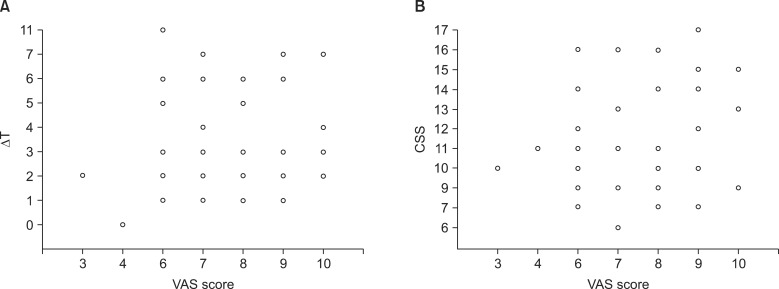
A total of 42 patients participated in this study, and the demographic data is illustrated in Table 3. The ΔT calculated from the IRT measurement was 3.0 ± 2.3℃; the VAS score (10 cm) was 7.6 ± 1.7, and the CSS was 11.7 ± 2.8. The distribution of the VAS score, CSS and ΔT is shown in Fig. 1.
The Spearman's rho of the correlation analysis of the ΔT and VAS score was 0.066 (P = 0.677) with no significant correlation. There also was no significant correlation between the CSS and VAS score (Spearman's rho = 0.163, P = 0.303). The distribution of these three variables is illustrated in a scatter plot in Fig. 2.
Go to :
DISCUSSION
As the pathophysiologic etiology of CRPS has not yet been determined, the diagnosis is based on signs and symptoms [4]. Likewise, even the most widely used CRPS diagnostic criteria-the Budapest criteria-is based on patients' subjective pain, as it is used to determine the presence of sensory change, vasomotor change, pseudomotor change, and motor change [2]. The presence of subjective pain is the most fundamental checklist item in the diagnosis of CRPS. In other words, CRPS cannot be diagnosed without a patient's perception of pain. Because the presence or the severity of pain cannot be directly objectified in any case, several studies have attempted to find an objective method indirectly related to the presence or severity of pain. Pleger et al. [12] reported that following behavioral treatment, CRPS patients experienced a decrease in pain and an increase in the 2-point discrimination thresholds as well as a concurrent change in the cortical map size of their primary and secondary cortex. Moreover, Kemler et al. [13] tried to establish a correlation between the degree of vasodilation measured using laser doppler flowmetry and pain mitigation effects of spinal cord stimulators, but failed to discover any significant correlation. Similarly, this study did not find any specific correlation between the CSS and VAS score, and also ΔT and VAS score, indicating that the CSS and ΔT do not offer objective representations of subjective pain.
Although the indicators of severity are not measurements with absolute objectivity, they are recognized as methods that can offer a certain degree of objectivity in classifying patients or determining the effects of treatment. Therefore, the suggested CSS is used in the clinical practice. The CSS comprises 17 criterias corresponding with the signs and symptoms and includes all the Budapest criteria which is highly related to the currently-used CRPS diagnostic criteria. It is supposed that the higher the CSS, the higher the pain intensity, emotional stress and impaired function, which restricts movement and induces a large difference in the skin temperatures of both limbs [8].
However, we could not find any significant correlation between the CSS and VAS score and also between CSS and ΔT. This may have resulted because CRPS is affected by several factors including peripheral, central, sympathetic mechanism and emotional factors [14,15]. And, because of these different influential factors, the difference in skin temperature between both limbs and the VAS score can be affected. Therefore it cannot determine the overall severity of CRPS.
There are various opinions on the relationship between CRPS and temperature difference. Some studies have reported that the early stages of CRPS display a "warm regulation type", which turns into a "cold regulation type" as the conditions become chronic [16,17], while others argue that the duration of the disease is irrelevant [18]. As mentioned before, the temperature difference is an important factor in the diagnosis of CRPS, although it is difficult to set a standard of a certain temperature. Therefore, the ΔT can vary greatly at various points in time, so that the degree of temperature asymmetry alone is insufficient to be used as a scale for the severity of the disease. Krumova et al. [10] reported that when the skin temperature is measured, the specificity is higher for the difference in the skin temperature reactions to external temperature changes than for the absolute skin temperature changes in CRPS patients. There were attempts to measure the body's changes of reaction to cold stress tests based on these results and to use them in the diagnosis of CRPS [19,20].
This study used an absolute value for the analysis instead of an actual value measured by thermography. This decision was based on previous study results showing that an absolute value is diagnostically more valuable in the diagnosis of CRPS than the actual value of the patients' skin temperature differences [21].
This study had limitations in that the sample size was small. However, it still holds great significance given the fact that it is difficult to recruit CRPS patients due to the rarity of the disease. Furthermore, because the correlation coefficients between the variables of this study were very low (0.066-0.163), it is proper to believe that a larger sample size would not display a higher correlation effect.
In conclusion, there was no correlation between CRPS patients' subjective pain, degree of skin temperature asymmetry and CSS. The degree of skin temperature asymmetry and CSS do not represent the severity of patients' subjective pain and should be cautious in evaluating CRPS patients.
Go to :
 XML Download
XML Download