

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Despite the advances in our understanding of the neurobiology of nociception, postoperative pain continues to be treated inadequately. There are many modalities that may provide effective postoperative analgesia, including systemic and regional analgesic options. A combination of analgesic agents in the postoperative period improves pain relief and minimizes opioid consumption and opioid associated side effects. Hence, multimodal analgesia facilitates patient recovery after surgery [1].
Postoperative pain and PONV are common symptoms in the postoperative period following laparoscopic cholecystectomy. Pain is the main complaint and the primary reason for prolonged convalescence after laparoscopic cholecystectomy [2,3]. The establishment of laparoscopic cholecystectomy as an outpatient procedure has highlighted the importance of reducing postoperative pain and PONV [4]. Opioids have been the mainstay for the treatment of postoperative pain; however, they are associated with PONV and other side effects. Therefore, the management of postoperative pain with opioid-sparing regimens may help to minimize both postoperative pain and PONV [5]. We feel that a multimodal approach targeting the reduction of postoperative pain with an opioid-sparing analgesic such as etoricoxib would minimize opioid consumption and its associated side effects, such as PONV; this along with a proven antiemetic medication like methylprednisolone should go a long way toward attenuating postoperative pain and PONV.
Preoperative glucocorticoid has been shown to decrease the PONV and postoperative fatigue associated with laparoscopic cholecystectomy [6,7]. Intravenous methylprednisolone 125 mg a day after surgery has been reported to have analgesic and opioid-sparing effects similar to those of non-steroidal anti-inflammatory drugs (NSAIDs) [8]. Romundstad et al. [9] observed that preoperative methylprednisolone reduces postoperative pain, emesis and fatigue after breast augmentation surgery. NSAIDs are recommended for routine use in patients undergoing laparoscopic cholecystectomy [10]. Etoricoxib, a selective cyclooxygenase-2 (COX-2) inhibitor, was found to reduce analgesic requirements after laparoscopic cholecystectomy during the postoperative period [11,12].
In the present clinical trial, we hypothesized that a combination of methylprednisolone and etoricoxib is more effective than either drug alone in the attenuation of postoperative pain and postoperative opioid consumption. The primary objectives of this study were to evaluate the effect of a preoperative single-dose administration of methylprednisolone + etoricoxib on postoperative pain and fentanyl consumption; secondary objectives were to evaluate its effects on PONV, fatigue, sedation, and respiratory depression.
Go to : 
MATERIALS AND METHODS
1. Study design
The present study was a prospective, randomized, double-blind and placebo-controlled clinical study. The study protocol was approved by the institutional ethical committee and written informed consent was obtained from all patients.
2. Inclusion criteria
Adult patients (20-65 yrs) of either sex of ASA physical status I or II scheduled for laparoscopic cholecystectomy under general anesthesia were included in the study.
3. Exclusion criteria
Patients with impaired kidney or liver functions, a history of drug or alcohol abuse, a history of chronic pain or daily intake of analgesics, uncontrolled medical disease (diabetes mellitus and hypertension), a history of intake of NSAIDs within 24 h prior to surgery, and those with the inability to operate a patient-controlled analgesia device were excluded from the study.
4. Randomization, study intervention and blinding
Patients meeting the inclusion criteria during the preanesthetic checkup were randomly assigned into four equal groups of 30 each with the help of a computer-generated table of random numbers. A random allocation sequence concealed in 120 consecutively numbered, sealed envelopes, determining group distribution, was computer-generated by a project nurse not otherwise involved in the trial. The envelopes were opened on the morning of surgery by a preoperative staff nurse not involved in the study; this nurse prepared the IV study drug formulation and handed it over to the research nurse along with the tablet to be administered to all of the patients. This research nurse, blind to the group allocation, administered the drugs to the patients as per the protocol below.
The methylprednisolone group received methylprednisolone 125 mg (Solu-Medrol™, Pfizer Manufacturing NV, Puurs, Belgium) intravenously (IV) plus a placebo tablet. The etoricoxib group received a sterile water IV and a 120 mg tablet of etoricoxib (Etorica-120™, Micro Eros Pharma Div, Bangalore, India). The combination group received methylprednisolone 125 mg IV plus a 120 mg tablet of etoricoxib, and the placebo group received a sterile water IV and a placebo tablet. The tablet formulations were administered orally with sips of water 1 hour prior to induction; the placebo tablets were matched with a tablet of etoricoxib and were supplied by the hospital pharmacy. The IV preparations were administered before the induction of anesthesia, with 10 ml of normal saline over 2 min. All study personnel and participants were blind to the group allocation for the duration of the study.
5. Anesthesia and analgesia protocol
All patients received oral lorazepam 0.04 mg/kg the evening before surgery and on the morning of surgery. The anesthesia technique was standardized in all groups. Patients were induced with 3 µg/kg of fentanyl by IV and by 2 mg/kg of propofol by IV; orotracheal intubation was facilitated by 0.08 mg/kg of vecuronium by IV. Anesthesia was maintained with a 100-200 µg/kg/min propofol infusion IV with 66% nitrous oxide in oxygen. At the end of the surgery, residual neuromuscular paralysis was antagonized with neostigmine at 0.04 mg/kg by IV and by glycopyrrolate at 0.01 mg/kg by IV. Following the recovery of self-respiration, the patients were extubated and shifted to the post-anesthesia care unit (PACU). In the PACU, patients received fentanyl by IV through a patient-controlled device (CADD-Legacy® 1 Pump Model 6400) with a patient-activated dose of 10 µg/ml and a lock out interval of 5 min, with the maximum allowable fentanyl dose being 2 µg/kg/hr.
6. Outcome measures and assessment
Primary outcomes were the severity of postoperative pain both at rest (static pain) and while coughing (dynamic pain) and postoperative fentanyl consumption; secondary outcome measures were PONV, fatigue, sedation, and respiratory depression. All of these measures were assessed by an anesthesia registrar blind to group allocation.
Assessment of pain was done by a 100 mm visual analogue scale (VAS); 0 = no pain, 100 = worst imaginable pain. The maximum pain scores (static and dynamic) were assessed on arrival to the PACU (0 hr) and at 2, 4, 8 and 12 hr postoperatively. The severity of the PONV was graded on a four-point ordinal scale (0 = no nausea or vomiting, 1 = mild nausea, 2 = moderate nausea, and 3 = severe nausea with vomiting); the severity of fatigue was also graded on a four-point ordinal scale (0 = no fatigue, 1 = mild fatigue, 2 = moderate fatigue, and 3 = severe fatigue). Rescue antiemetic ondansetron, 4 mg by IV, was given to all patients with a PONV of grade equal to or greater than 2. The Ramsay sedation scale (awake levels were as follows: 1 - anxious, agitated or restless, 2 - cooperative, oriented and tranquil, and 3 - responds to commands; asleep levels were dependent on each patient's response to a light glabellar tap or a loud auditory stimulus, as follows: 4 - brisk response, 5 - a sluggish response, 6 - no response) was used to assess the level of sedation; patients with a sedation scale of ≥ 4 were considered as sedated [13]. Respiratory depression was defined as a respiratory rate of ≤ 8 breaths/min and an oxygen saturation rate of < 90% without oxygen supplementation.
7. Sample size estimation
The sample size calculation was based on the primary outcome measures. Assuming that the therapeutic drug would reduce postoperative VAS scores by 30% as compared to the placebo (with an assumed mean postoperative VAS score of 45 mm and a standard deviation of 20 mm at all time points in the placebo group), a sample size of 25 patients was required in each group for the results to be significant (with α = 0.05 and power = 80%) [14]; on the other hand, a sample size of 26 patients in each group was required if we presumed that the study drug would reduce the mean total postoperative fentanyl consumption by 35% (with α = 0.05 and power = 80%). To account for drop outs we enrolled 30 patients in each group.
8. Statistical analysis
Demographic data were analyzed with a one-way ANOVA for continuous variables and chi-square test for categorical variables. The VAS pain scores and sedation scores were analyzed with the Mann-Whitney U test; the incidences of PONV, fatigue, sedation and respiratory depression were analyzed with Fisher's exact test with Bonferroni correction for multiple comparisons. The method of analysis was determined prospectively, and it incorporated the intention-to-treat principle. The software package SPSS 21.0 (SPSS Inc., Chicago, IL) was used for the statistical analysis. P < 0.05 was considered significant.
Go to :
RESULTS
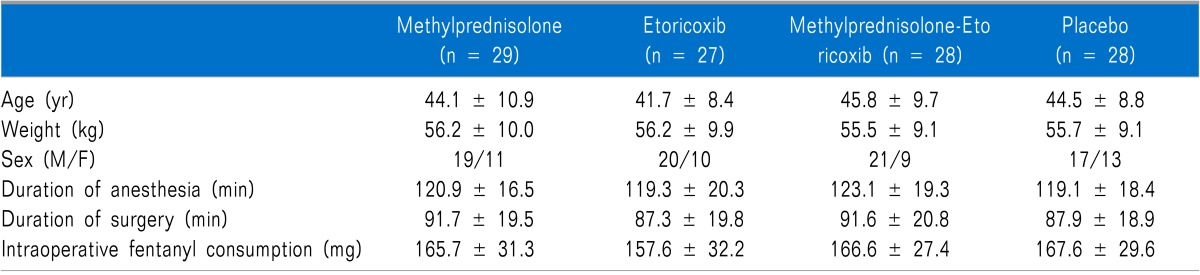
A total of one hundred and forty three patients were assessed for eligibility between October 2012 and September 2013, out of which 120 patients received the study medication following randomization, and 112 patients, i.e. 94%, completed the study (Fig. 1). The reasons for patients not being randomized were refusal to participate in the study (18 patients), chronic analgesic consumption (2 patients) and an inability to operate the patient-controlled analgesia device (3 patients). Eight patients were excluded from the study following the initial randomization process and were therefore not subjected to further analysis (7 underwent a conversion to open cholecystectomy and 1 needed re-exploration on account of postoperative bleeding). There were no differences amongst the groups with regard to age, sex, weight distribution, the duration of anesthesia, the duration of surgery or the level of intra-operative fentanyl consumption (P > 0.05) (Table 1).

Postoperative pain (static and dynamic) and fentanyl consumption were significantly reduced by methylprednisolone, etoricoxib and the combination groups as compared with the placebo (P < 0.05) (Table 2). The methylprednisolone + etoricoxib combination caused a significant reduction in postoperative pain and fentanyl consumption as compared to methylprednisolone or etoricoxib alone (P < 0.05) (Table 2); however, there was no significant difference between the methylprednisolone and etoricoxib groups in these respects (P > 0.05) (Table 2).
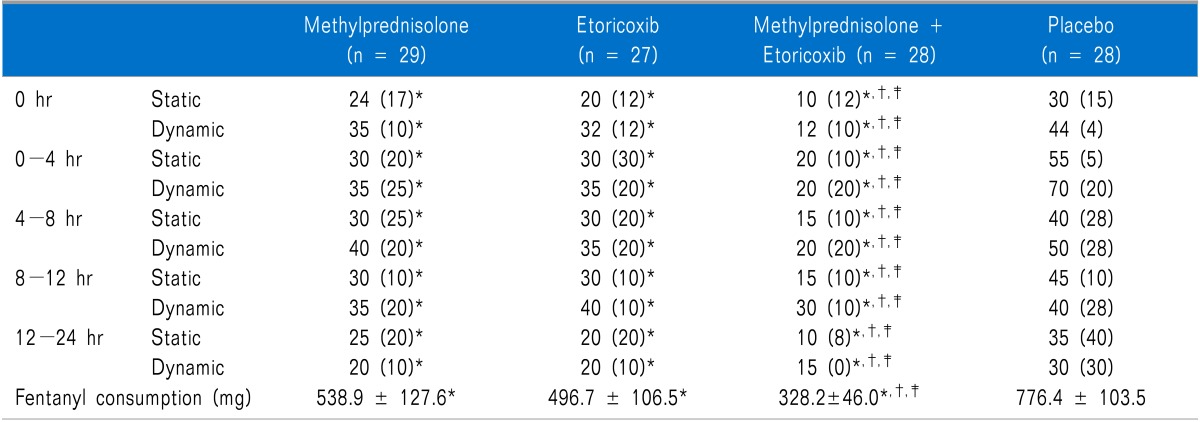
Table 2
Postoperative Pain (VAS scores) and Fentanyl Consumption
Data are presented as median (inter-quartile range) or mean values + SD; *P < 0.05 during intergroup comparison of placebo vs other groups, †P < 0.05 during intergroup comparison of methylprednisolone-etoricoxib vs methylprednisolone and ‡P < 0.05 during intergroup comparison of methylprednisolone-etoricoxib vs etoricoxib.
![]()
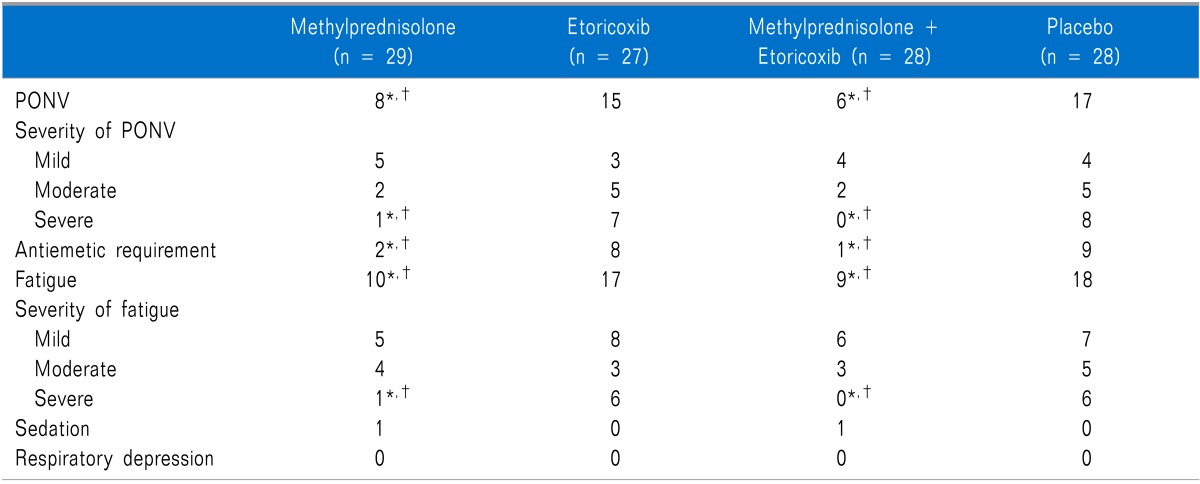
Methylprednisolone and the methylprednisolone + etoricoxib combination significantly decreased the incidence and severity of PONV, fatigue and the total number of patients requiring an antiemetic treatment when compared to a placebo and etoricoxib (P < 0.05) (Table 3). The incidence of sedation and respiratory depression did not differ among the four groups (P > 0.05) (Table 3).
Go to :
DISCUSSION
In the present study, we observed that a preoperative single-dose administration of a methylprednisolone + etoricoxib combination reduces postoperative pain (static and dynamic) along with PONV, fentanyl consumption, antiemetic requirements, and fatigue more effectively than either drug used alone in patients undergoing laparoscopic cholecystectomy.
Etoricoxib has been prescribed for the relief of chronic pain in osteoarthritis and rheumatoid arthritis, as well as acute pain. The drug is believed to be associated with fewer upper gastrointestinal adverse effects than conventional NSAIDs [15]. A preoperative 120 mg single dose of etoricoxib produces effective pain relief after surgery [15]. It has been found to reduce the analgesic requirements after a laparoscopic cholecystectomy in the postoperative period [12]. In the present study, etoricoxib at 120 mg was observed to be effective for reducing postoperative pain and fentanyl requirements.
Glucocorticoids are well known for their analgesic, antiinflammatory, immune-modulating, and antiemetic effects [16]. Several randomized, clinical trials in different major and minor surgical procedures have been conducted to examine the effects of a perioperative single-dose glucocorticoid administration on surgical outcomes. The overall results with regard to postoperative outcome have either been positive in favor of the glucocorticoid group or without differences between study groups, with PONV and pain as the most significantly improved outcome parameters [7,9,17,18]. Data from laparoscopic cholecystectomy have shown debatable effects with regard to pain, nausea, and vomiting, but with higher satisfaction levels and shorter stays in day-care units [5,6,19]. In the present study, combining methylprednisolone with etoricoxib not only improves pain relief and reduces postoperative opioid consumption but also reduces the incidence and severity of PONV; hence, this combination serves an important role of multimodal therapy against pain and PONV concurrently.
The potential side effects of perioperative glucocorticoid administration have been of much concern; the most important potential risks in the postoperative period include gastrointestinal bleeding, impaired wound healing, or increased susceptibility to infection [20]. In a meta-analysis of 51 studies including more than 1900 patients receiving doses of 15-30 mg/kg of methylprednisolone, no significant increase in the risk of any of these side effects was found [21]. Many of these studies were conducted in settings at even higher risk for complications than elective THA, such as cardiac, spine, and trauma surgery.
An increasing number of laparoscopic procedures, including laparoscopic cholecystectomy surgery, are now being performed on an outpatient basis [22]. Postoperative pain and PONV have been shown to affect the recovery process and delay the patient discharge significantly [23]. Pain is a key independent predictor of recovery and delayed discharge [24].
The concept of multimodal or balanced analgesia is well established and suggests that combinations of several analgesics of different classes and different sites of analgesic administration rather than a single analgesic or a single technique provide superior pain relief with reduced analgesic-related side effects [1,25,26]. A number of studies have shown that multimodal analgesia techniques reduce opioid consumption in the postoperative period [27].
Nausea often accompanies pain in the early postoperative period and can be relieved concomitantly with the pain [28]; PONV also increases the patient discomfort and may also contribute to pain [23]. Methylprednisolone has a proven track record for attenuating PONV; it has also been used for the management of postoperative pain [8,9]. Methylprednisolone, owing to its anti-inflammatory and membrane stabilization action, may be responsible for attenuating postoperative pain and may thus contribute to the concept of multimodal analgesia. This action of methylprednisolone has been widely used in interventional pain practices for chronic pain management [29] and therefore needs to be explored in relation to the management of postoperative pain.
The concept of multimodal analgesia is well established for the management of pain. We wish to take this further by suggesting that if methylprednisolone is combined with etoricoxib for the prevention of postoperative pain and PONV, then methylprednisolone can attenuate PONV and at the same time enhance the effectiveness of etoricoxib due to its anti-inflammatory and membrane stabilization action, thereby enhancing the opioid-sparing properties of etoricoxib by providing postoperative pain relief while also reducing postoperative opioid consumption and PONV.
A limitation of the present study is that a number of comparisons have been done in this study and the sample size is small. Future studies evaluating the role of methylprednisolone in combination with other analgesics to reduce postoperative pain and PONV are required.
In conclusion, the preoperative single-dose administration of a methylprednisolone + etoricoxib combination was most effective for reducing postoperative pain (static and dynamic), fentanyl consumption, PONV, the need for rescue antiemetics and fatigue in patients undergoing laparoscopic cholecystectomy. We therefore suggest that a combination of methylprednisolone and etoricoxib should be routinely administered preoperatively to all patients undergoing laparoscopic cholecystectomy to minimize postoperative pain, fentanyl consumption, PONV, antiemetic requirements and fatigue.
Go to :
 XML Download
XML Download