

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Spinal stenosis is a common degenerative disease induced by nerve compression after narrowing of the spinal canal, lateral recess, or intervertebral foramen. In humans, spinal stenosis can compress the dorsal root ganglia (DRG), causing several symptoms, such as leg pain, motor and sensory impairment, and intermittent neurogenic claudication [1,2]. In animal models, chronic compression of the L4 and L5 DRG leads to ipsilateral cutaneous allodynia and hyperalgesia [3].
Although the pathophysiological mechanisms of spinal stenosis remain controversial, nerve root ischemia caused by mechanical compression is considered to be the most likely mechanism initiating inflammatory reactions with degenerative changes in DRG [4,5]. Prostaglandin E1 (PGE1) is a powerful vasodilator with antiplatelet and cytoprotective properties [6,7] that has been suggested to be a therapeutic agent for lumbar spinal stenosis. Several clinical studies have demonstrated that oral or intravenous administration of a PGE1 agonist can improve various symptoms of spinal stenosis [8,9,10].
A lipo-PGE1 agonist, a PGE1 derivative, is a lipogenated agent prepared by the dissolution of PGE1 in a lipid microsphere. It has been reported to efficiently accumulate in vascular lesions of nervous tissue after intravenous injection [11,12]. Meanwhile, a few studies suggested lipo-PGE1 prevent apoptotic cell death and inhibit neuronal degenerative change [13,14,15]. We focused on these characteristics of lipo-PGE1 and sought to administer it epidurally in a rat with foraminal stenosis. We evaluated the therapeutic effects of epidural lipo-PGE1 for improving and treating the neuropathic pain pattern of spinal stenosis in a rat foraminal stenosis model, and assessed the degree of microscopic changes in target DRG.
MATERIALS AND METHODS
1. Study materials
The experimental protocol was reviewed and approved by our institutional Animal Care and Use Committee (IACUC 06-036). The current study was conducted using 40 male Sprague-Dawley (SD) rats.
The rats were divided into three groups. In Group I, the epidural PGE1 group (EP) (n = 15), 0.15 µg/kg lipo-PGE1 (Eglandin®, Mitsubishi Tanabe Korea, South Korea) was infused once daily for 10 days from postoperative day 3 using an epidural catheter. In a recent study, we used 10 µg/ml, a 1 ml ampoule. The rats weighed 250-300 g at the time of injection; thus, we injected 0.037-0.045 µg on average. In Group II, the saline group (n = 15), the same volume of normal saline was infused using an epidural catheter. In Group III, the control group (n = 10), no drug was administered following establishment of the experimental model of spinal stenosis.
2. Establishment of spinal stenosis model
After induction with oxygen (3 L/min) and sevoflurane (3%), a longitudinal skin incision was made between L4 and L6. Then, the neural foramen between L5 and L6 on the left side was exposed. A stainless steel rod with an external diameter of 0.6-0.8 mm and a 4-mm length, was inserted into the intervertebral foramen at a 30° angle from the posterior central line and a 10° angle from the lateral parallel line, as suggested by Hue and Xing [3]. Following this, a stainless steel rod was placed on the L5 DRG to provide chronic DRG compression and foraminal stenosis.
An epidural catheter was prepared by making a knot 2.5 cm from the tip of a 17-cm microplastic catheter (PE-10; Natsume Co., Japan), as suggested previously [16,17]. The skin between T13 and L1 was incised at an approximate length of 3 cm. Then, the area adjacent to the supraspinous ligament was dissected using microsurgical scissors, and a small hole was made in the ligamentum flava. A catheter was inserted into the epidural space and was advanced caudally (approximately 2.5 cm) to the site between the L4 and L5 vertebral levels.
3. Behavioral observations
The daily feeding habits, sleeping, and behavioral patterns of the rats were monitored meticulously. If the rats showed severe excitatory symptoms, such as epilepsy, vocalization, or hyperrespiration, they were excluded from the study as having a hypersensitivity reaction. Behavioral observations were based on the assessment of motor function and the threshold response to mechanical stimuli. These evaluations were done preoperatively, on postoperative day 3, on drug administration days 1, 5, and 10, and weeks 1, 2, and 3 after final administration of the drugs (Fig. 1). All assessments were made by a single investigator who was blinded to the experimental procedure.
4. Assessment of motor function
The gait pattern was evaluated using the following motor grading system [18]:
Cases with Grade 2 or more were considered to have damage to the motor nerve.
5. Mechanical withdrawal threshold
The thresholds for mechanical stimuli were evaluated using eight von-Frey filaments (2.0-15.0 g) with an up-down method [19]. Thus, we assessed the avoidance response when the medial hind paw was stimulated by means of weighted von-Frey filaments (4.5 g). According to the methods of Dixon and Massey [20], stimuli were administered six times to calculate a 50% threshold for an avoidance response using an up-down regulation. A 50% response threshold was calculated using the following formula:
where Xf = size of filaments that were finally exerted (log units); κ = correction coefficient depending on the pattern of response; and δ = mean difference between the stimuli (here, δ = 0.224).
The percentile value of the difference in withdrawal latency in the lesions on the operated side (Mi), and the normal area on the contralateral side (Mc) was calculated using the formula (Mi - Mc)/Mc × 100. A positive percentile value (Mi > Mc) indicates hypoalgesia, and a negative percentile value (Mi < Mc) indicates hyperalgesia.
6. Microscopic assessment
For microscopic examination, all rats were sacrificed on day 3 after completion of the behavioral observations, which was the 24th day after final drug administration. Under general anesthesia using oxygen (3 L/min) and sevoflurane (2%), 200 mL of normal saline followed by 200-300 mL of 4% paraformaldehyde in a 0.1 M phosphate buffer was perfused transcardially into each rat. Once we extracted the vertebrae body around L5 with en-bloc technique, and then, the DRG, adjacent nerve roots, and spinal nerves at L5 where the stainless rod had been placed were carefully isolated. If inserted stainless steel rods that were not placed in the neural foramens are exempted from the test results.
The sampled tissue was treated with 10% w/v EDTA, and embedded in paraffin wax. Using standard tissue slide preparation methods, slides were prepared from 4-5 µm sections and stained with hematoxylin and eosin (H&E) and additionally Masson's trichome staining in case of fibrosis analysis. We examined and analyzed the histopathological findings, such as the degree of chromatolysis, chronic inflammation, and fibrosis, in light microscopic images. A microscopic assessment of the tissues was performed [21] by a single pathologist who was blinded to the test group.
The histopathological findings were classified as described subsequently:
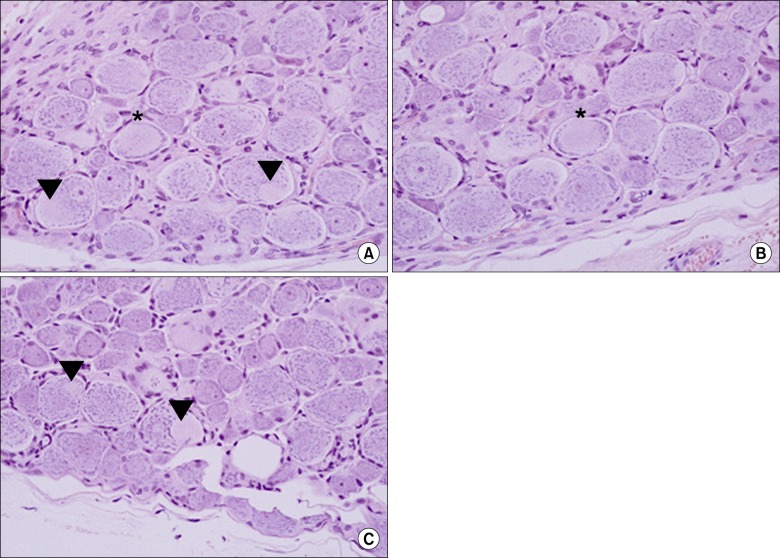
Chromatolysis was divided into central and segmental chromatolysis. Thus, total chromatolysis as the ratio relative to the total number of neurons was obtained (Fig. 2).
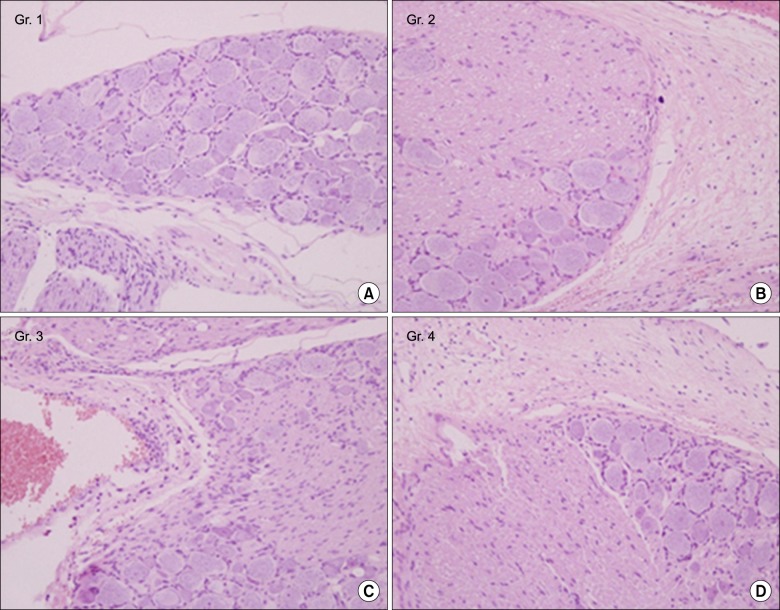
The histological degree of fibrosis was graded by the extent and intensity of collagen fibers detected by Masson's trichome staining, as shown in Fig. 3.
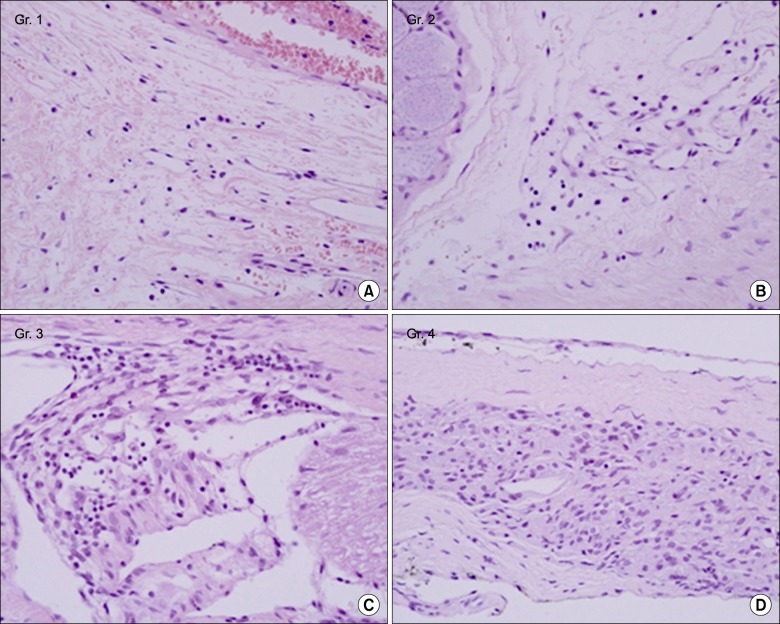
The histological grading system of inflammation was modified from that of Salafia et al. [22] (Fig. 4).
7. Statistical analysis
Based on the results obtained using the two types of behavioral observation, an intergroup comparison during the follow-up period was made using the Kruskal-Wallis test. If there was a significant difference, further statistical analysis was performed using the Mann-Whitney U-test with Bonferroni's correction for post hoc analyses. In cases in which a significant time-dependent change occurred within the same group, a repeated-measures analysis of variance (ANOVA) was performed. The light microscopic assessment of chromatolysis in slide samples was assessed using the Kruskal-Wallis test. The comparison of the degree of chronic inflammation and fibrosis was tested using Fisher's exact test. All measurements are expressed as mean ± standard deviation or standard error of the means (SEM) (%). Statistical significance was indicated by P < 0.05.
RESULTS
1. Assessment of motor function
Prior to surgery, all the rats showed normal gait. During the postoperative observational period, no rats showed motor paralysis. All the rats could ambulate normally within 1 h after surgery, and none had excitatory symptoms or hyperrespiration during the drug administration period.
2. Mechanical withdrawal threshold
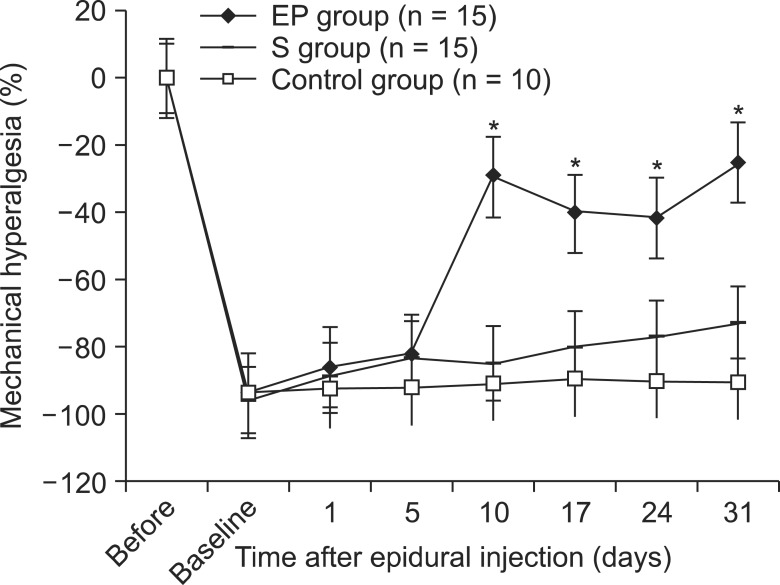
Fig. 5 shows the changes in mechanical hyperalgesia over time for each group. In all rats, the mechanical threshold decreased after surgery. The degree of hyperalgesia was not significantly different among the groups before drug administration to 5 days after the epidural injection (P > 0.05). The degree of mechanical hyperalgesia was -93.2 ± 1.4% (mean ± SEM) immediately before the administration of lipo-PGE1 in the EP group, and then gradually recovered to -29.0 ± 11.3% up to 10 days after epidural injection. In the EP group, significant differences in mechanical hyperalgesia between the control and saline groups existed (P < 0.05). Additionally, this was maintained, with a value ranging from -41.0 to -25.3%. In the saline and control groups, mechanical hyperalgesia was evident during the entire observational period.
3. Microscopic assessment
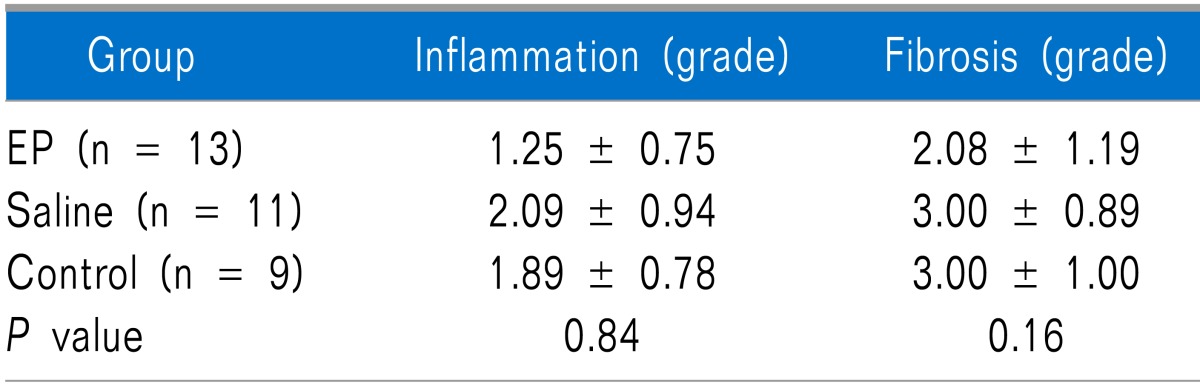
When dissecting peri L5- DRG area, all the stainless steel rods were placed at the initial place. Two slides in the EP group, four in the saline group, and one in the control group were excluded from microscopic evaluation because DRG were not seen in the slides. In the EP group, total chromatolytic findings were significantly lower than those in the other groups (P < 0.05) (Table 1). In the EP group, the degree of fibrosis and inflammation was slightly lower than that in the other groups; however, no statistically significant difference was observed (Table 2).
DISCUSSION
In this study, an epidurally administered lipo-PGE1 agonist was assessed with regard to relieving mechanical hyperalgesia in a rat spinal stenosis model. Hu and Xing [3] first suggested this spinal stenosis model in rats, which resulted in mechanical and thermal hyperalgesia at the injured hind paw. From this, they assumed that direct compression and secondary inflammation of DRG would play a role in generating the hyperexcitability of DRG and, in turn, hyperalgesia. Rydevik et al. [23] had previously reported that local compression of DRG induced intraneural edema and subsequent elevation of interstitial tissue fluid pressure, leading to a reduced blood flow, inducing an ischemic situation in DRG, and finally producing nerve root pain. Based on these previous studies, we adopted this model. We reproduced mechanical hyperalgesia in the injured hind paw and inflammation of injured DRG. From the experimental studies, three days in rat's age is approximately equivalent to 3 months of human life [24]. We assumed, therefore, evaluation and drug administration at 3 rd day after the launch was efficient time interval to induce chronic degeneration and neuropathic response. Then, we injected a lipo-PGE1 agonist epidurally to assess recovery from hyperalgesia in the rat model. In this study, mechanical hyperalgesia was induced after surgery and began to recover over 5 days of the epidural administration of the lipo-PGE1 agonist. We could not confirm the exact timing from when the recovery was revealed, between the 5th day and 10th day. On the other hand, in the saline and control groups, mechanical hyperalgesia was maintained during the entire period. These findings indicate that mechanical hyperalgesia did not simply decrease in a time-dependent manner.
Various animal experiments have demonstrated the efficacy of PGE1 in spinal stenosis [12,25]. In one of the latest studies, Shirasaka et al. [26] found that a PGE1 derivative dilated arteries and improved blood flow in nerve roots without blood stasis in veins. They assumed that this effect was derived by mediation of the Procyclin (IP) receptor and that it was associated with cyclic guanosine monophosphate (GMP). In clinical studies, intravenously administered lipo-PGE1 has been reported to be effective for the treatment of intermittent neurogenic claudication, ambulatory function, and numbness of the lower extremities in more than 77% of patients with spinal stenosis [9]. Myeloscopic findings showed that the blood vessels on the surface of the subarachnoid membrane were dilated following administration of a lipo-PGE1 agonist in patients with spinal stenosis.
We also performed an animal study by administering the lipo-PGE1 agonist intravenously in the same spinal stenosis model [27]. As a result, the intravenous lipo-PGE1 agonist improved mechanical hyperalgesia. Comparing that result with recent data, there was almost a similar effect on induced mechanical hyperalgesia as well as less chromatolysis. Based on the many reports on intravenous administration of a lipo-PGE1 agonist, we inferred that this effect resulted from an increase in blood flow to the injured nerve lesion.
Nevertheless, no reports are available on epidurally administered lipo-PGE1. Theoretically, at least, an epidural approach would seem to be beneficial, as opposed to other administration routes, because the major target of the drug is the spinal cord. First, smaller amounts of epidural agents could have similar effects to larger amounts of intravenous drugs and cause fewer systemic side effects [28]. Second, the risk of developing neurotoxicity after intrathecal drug administration is assumed to decrease with epidural drug administration. An epidural approach may be considered clinically uncomfortable and difficult. Nevertheless, for pain clinicians, an epidural approach may be a relatively easy and useful way of treating patients with chronic low back pain. Also Epidural injection might be hazardous. The recent incident related with contaminated steroid injection in the United States would be an example of this [29]. On the other hand, it impetuses researchers to develop a different medication other than steroids. For these reasons, our study, which is the first reported trial of a lipo-PGE1 agonist administered into the epidural space, would seem to be useful.
Chromatolysis is accompanied by an increase in ribonucleic acid (RNA) and protein synthesis. Apparently, the chromatolytic reaction to axotomy represents a shift of protein synthesis from that destined for export to protein required for "domestic" use in regeneration. Although the chromatolytic process may be a straightforward reaction to cell injury, it may also be a reaction to the loss of contact with a target organ. In this way, neurons return to a state more similar to their condition during development, and the accompanying cytological changes are consistent with this [30]. Central chromatolysis signifies the loss or dispersion of Nissl bodies, starting around the nucleus and extending peripherally. This is the classical neuronal response to axotomy and also occurs after some toxic injuries to neurons [31]. In contrast, peripheral chromatolysis is thought to be much less common; however, it has been reported after axotomy or ischemia in certain species. Segmental chromatolysis may represent partial compression of the axon or segmental loss of axonal contact with target organs, whereas central chromatolysis follows complete axotomy. In our study, segmental chromatolysis could have been induced by a local toxic injury, such as persistent ischemia by the stainless steel rod compression, and chromatolysis was markedly decreased in the EP group. We suggest that epidural administration of lipo-PGE1 increased segmental blood flow into the DRG and protected the neuron from chromatolysis and subsequent cell death.
In addition to the vasodilatory properties of PGE1, many experimental studies have demonstrated that PGE1 analogs regulate inflammatory cytokines and immune functions [7], reduce trauma-induced rat spinal cord injury by inhibiting neutrophil activation [32], and block apoptotic cell death in the dorsal horn induced by sciatic nerve occlusion [13]. We also microscopically examined the degree of inflammation and fibrosis around the DRG. However, no significant difference was observed in inflammation or fibrosis around the injured DRG among the groups. These results suggest that the lipo-PGE1 agonist might have no strong effect on reducing inflammation in the injured DRG; rather than by inhibiting inflammation, it might work by another mechanism. As reviewed previously, a large body of evidence indicates that lipo-PGE1 acts as a vasodilator and increases blood flow around injured neurons.
In our study, we did not use an epiduroscope with a video camera or a laser Doppler flow meter and were unable to conclude that the positive effect of the epidurally administered lipo-PGE1 agonist definitely resulted from an increased blood flow to the injured DRG and nerve root. Another limitation of this study is that we did not accurately calculate the conversion ratio between intravenous and epidural administration. Sekikawa [12] examined blood flow and oxygen pressure in lumbosacral nerve roots with various intravenous doses and concluded that 0.15 µg.kg-1 significantly increased blood flow and oxygen pressure to nerve roots under a dural tube compression condition. Therefore, we used a dose of 0.15 µg.kg-1 lipo-PGE1 similar to the intravenous injection.
Clinically, steroid injections into the epidural space are frequently performed in patients with spinal stenosis or postspinal surgery pain syndrome. Although no strong recommendations with evidence levels of Level II-1 to II-2 are available [33], some restrictions on lumbar epidural steroid injection exist, such as limited availability or frequent recurrence of pain. In this study, we demonstrated the effectiveness of a lipo-PGE1 agonist and its epidural administration in a rat foraminal stenosis model. If anti-inflammatory agents and lipo-PGE1 are administered together epidurally, there would a great advantage in drug delivery, both by the anti-inflammatory effect and increasing blood flow to the nerve root to inhibit inflammation. Although further experiments on the safety and appropriate doses of lipo-PGE1 and formal clinical trials are obviously needed, we suggest that epidurally administered lipo-PGE1 may be a useful therapeutic candidate in patients with spinal stenosis.


 XML Download
XML Download