

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Psychosomatic disorders are defined as disorders characterized by physiological changes that originate partially from emotional factors. Psychosomatic disorders can affect the oral cavity since the oral environment is related directly or symbolically to the major human instincts and passions and is charged with a high psychological potential [1]. Psychosomatic disorders may be due to several biochemical disorders involving neurotransmitters in the brain, incomplete connections with in the oral region and undefined complaints due to cognitive processes in higher centers of the brain [2].
A simple working type classification has already been proposed for the psychosomatic disorders of the oral cavity [3]. This article aims to discuss the psychosomatic disorders pertaining to dental practice with a revised working type classification. The simple working type classification includes pain related disorders, disorders related to altered oral sensation, disorders induced by neurotic habits, autoimmune disorders, and miscellaneous disorders.
Go to : 
PAIN RELATED DISORDERS
Pain related disorders include disorders of the orofacial region presenting with vague pain attributed to psychological stress [3]. This category includes myofascial pain dysfunction syndrome (MPDS), atypical facial pain, atypical odontogenic pain, and phantom pain.
1. Myofascial pain dysfunction syndrome (MPDS)
Myofascial pain dysfunction syndrome (MPDS) of the temporomandibular joint (TMJ) is a psychophysiological disorder that develops as a result of hyperactive muscles of mastication. In this syndrome, the changes in chronic masticatory muscle pain seem to be attributed to psychological stress [4]. In a preliminary study performed on patients with temporomandibular joint disorders, using Research Diagnostic Criteria (Axis II), it was found that more severe depressive and nonspecific physical symptoms were evident in patients with MPDS [5].
2. Atypical facial pain
Atypical facial pain is persistent idiopathic facial pain which lacks clear diagnostic criteria and standard treatment. Occlusal factors are less important and psychological and biochemical factors are recognized in its etiology [6]. Atypical facial pain may be related to apical fenestration and overfilling [7].
3. Atypical odontogenic pain
Atypical odontogenic pain is a chronic form of dental pain without signs of pathology. The pathophysiology has been proposed to be psychogenic, vascular, neuropathic, or idiopathic [8]. Dental surgeons are most likely to encounter these patients, and reaching a definitive diagnosis of atypical odontogenic pain can be a complex challenge [9].
4. Phantom pain
Phantom pain involves the sensation of pain in a part of the body that has been removed (most often associated with limb amputation). In the oral cavity, phantom tooth pain is usually associated with tooth extraction [10]. The theory and phenomenology of orofacial phantom pain in the oral cavity can be graded into phantom tooth pain, phantom bite syndrome, and intraoral stump pain [11]. Marbach described the term "phantom bite" as a patient's perception of an irregular bite when the clinician could identify no evidence of a discrepancy [12].
Go to :
DISORDERS RELATED TO ALTERED ORAL SENSATION
Disorders related to altered oral sensation are disorders in which the clinical presentation of the patient may be a persistent intraoral burning sensation [3]. This category includes burning mouth syndrome, idiopathic xerostomia, idiopathic dysgeusia, glossodynia, and glossopyrosis.
1. Burning mouth syndrome
Burning mouth syndrome (BMS) is a disorder presenting with an intraoral burning sensation for which no medical or dental cause can be found. Poor quality of life, depression, anxiety, and somatization are also often associated with this disorder. The available literature suggests that burning mouth syndrome is a multifactorial disorder associated with psychological components such as anxiety, depression, and cancerophobia [13]. The psychological aspects of burning mouth syndrome can be categorized into chronic somatoform dysfunction, chronic vegetative disorders, and chronic pain phenomenon [14].
2. Idiopathic xerostomia
Xerostomia is a common condition associated with quantitative and qualitative changes in saliva, which are generally referred to as salivary hypofunction (dry mouth). This can be caused by various systemic diseases such as Sjogren's syndrome, the anticholinergic effects of many medications, psychological conditions, and physiological changes [15]. Depressive symptoms are usually evident in individuals with idiopathic subjective dry mouth [16].
3. Idiopathic dysgeusia
Dysgeusia refers to persistent abnormal taste. It can also occur as a result of dry mouth, as adequate saliva is necessary for the function of taste, or it can be secondary to burning mouth syndrome in psychiatric patients [13]. Dysgeusia is a common oral side effect of cancer therapy (radiotherapy, chemotherapy, or combined modality therapy) and often impacts negatively on quality of life [17]. Unfortunately, the underlying causes are often not found, and the majority of patients are considered idiopathic dysgeusia cases [18].
5. Glossopyrosis
Glossopyrosis is a burning sensation of the tongue. It is usually associated with burning mouth syndrome. This condition may be the result of gastrointestinal, immunologic, neurologic, psychiatric, and dermatologic diseases. Lengthy periods of depression tend to be seen before the manifestation of the full clinical picture of glossopyrosis [21]. Lingual burning in patients with glossopyrosis is consistent with hyperalgesia, and neurogenic inflammation is observed in patients and animals with magnesium deficiency and in magnesium-deficient tissues [22].
Go to :
DISORDERS INDUCED BY NEUROTIC HABITS
Disorders induced by neurotic habits are disorders induced by parafunctional activity of the soft and hard tissues of the oral cavity [3]. This category includes dental and periodontal diseases caused by bruxism and biting of the oral mucosa (self-mutilation).
1. Dental and periodontal diseases caused by bruxism
Bruxism is the parafunctional clenching and grinding action between the upper and lower teeth. During this activity, extremely strong forces can be applied for periods of time exceeding those of functional mastication. These biomechanical loads create many dental problems, such as abfractions, hypersensitivity, periodontal distraction, and temporomandibular dysfunction [23]. The physiology and pathology of bruxism are unknown, although stress and anxiety are considered to be risk factors [24]. Behavioral problems and potential emotional problems have been found to be potential risk factors for bruxism in children [25].
2. Biting of oral mucosa (self-mutilation)
Self-mutilation due to biting of the oral mucosa originates as a result of chronic cheek, lip, or tongue biting [26]. These lesions are often observed in people who are under stress, and psychogenic background must be ruled out in individuals who exhibit this activity. This type of behavior may also be exhibited in cases in which people wish to obtain special attention from family members.
Go to :
AUTOIMMUNE DISORDERS
Autoimmune disorders are common dermatologic diseases with oral manifestations with psychological stress as an etiologic factor in the disease progression [3]. This category includes recurrent aphthous stomatitis, lichen planus, psoriasis, mucous membrane pemphigoid, and erythema multiforme.
1. Oral lichen planus (OLP)
Lichen planus is a common chronic immunologic inflammatory disease of the mucosa and skin presenting as interlacing white keratotic lines (Wickham's striae) typically located bilaterally on the buccal mucosa [27]. The exact etiology of OLP is unknown, but it is thought to arise due to immunologic disturbances (T-cell mediated and antigen-specific mechanisms). It is currently considered to be a disease that develops as a psychiatric problem due to depression, anxiety, and stress [28].
2. Recurrent aphthous stomatitis
Recurrent aphthous stomatitis (RAS) is the most common type of ulcerative disease of the oral mucosa. RAS can be a manifestation of a serious health condition, such as an autoimmune disorder, human immunodeficiency virus, infection, and hematologic or oncologic disorders [29]. Psychological stress may play a role in the manifestation of RAS and it may serve as a trigger or a modifying factor rather than being a cause of the disease [30].
3. Psoriasis
Psoriasis is a common dermatologic disorder that displays an association with stress or psychological distress [31]. There is a significant association between pustular psoriasis and an oral lesion, such as geographic tongue and fissured tongue [32]. Psoriasis may also manifest as inflammatory temporomandibular joint lesions and gingival and mucosal lesions.
4. Mucous membrane pemphigoid
Mucous membrane pemphigoid, a heterogeneous group of autoimmune blistering diseases, affects primarily the mucous membranes (oral and ocular mucosa) [33]. Diseases in this group have been noted to be associated with stress and depression as predisposing factors.
5. Erythema multiforme
Oral erythema multiforme (EM) can present with oral and lip ulcerations without manifesting target lesions on the skin [34]. This disease may occur secondary to herpetic infection. In herpes-associated EM, it is most likely that HSV-DNA fragments in the skin or mucosa precipitate the disease [35]. In this case, the role of stress is evident with deregulation of T-lymphocyte activity.
Go to :
MISCELLANEOUS DISORDERS
Miscellaneous disorders comprise an unclassified category in which the role of stress is important in the disease progression [3]. This category includes recurrent herpes labialis, necrotizing ulcerative gingivostomatitis, chronic periodontal diseases, and cancerophobia.
1. Recurrent herpes labialis
Recurrent herpes labialis is a mucocutaneous infection with herpes simplex virus type 1 (HSV-1) causing pain and blistering on the lips and perioral area (cold sores). Stress is an important precipitating factor in subjects with recurrent herpes labialis, involving modulations of T-lymphocyte function [36].
2. Necrotizing ulcerative gingivostomatitis
Necrotizing ulcerative gingivostomatitis (NUG) is a relatively uncommon disease characterized by gingival necrosis and ulceration, pain, and bleeding [37]. Emotional stress is one of the predisposing factors for NUG, and appears to play a role through induction of increased cortisol and catecholamine levels [38].
3. Chronic periodontal diseases
The literature has shown that stress and psychological factors are possible risk factors for periodontal disease [39,40]. Stress and depression may be associated with periodontal destruction through behavioral and physiologic mechanisms. Proper diagnosis and treatment of depression may be an important part of periodontal preventive maintenance.
4. Cancerophobia
Cancerophobia is the persistent fear in a patient's mind that he or she has contracted oral cancer. This has been observed to be associated with depression. Cancerophobia is often seen in association with burning mouth syndrome [13].
Go to :
PROPOSAL OF REVISED WORKING TYPE CLASSIFICATION FOR PSYCHOSOMATIC DISORDERS PERTAINING TO DENTAL PRACTICE
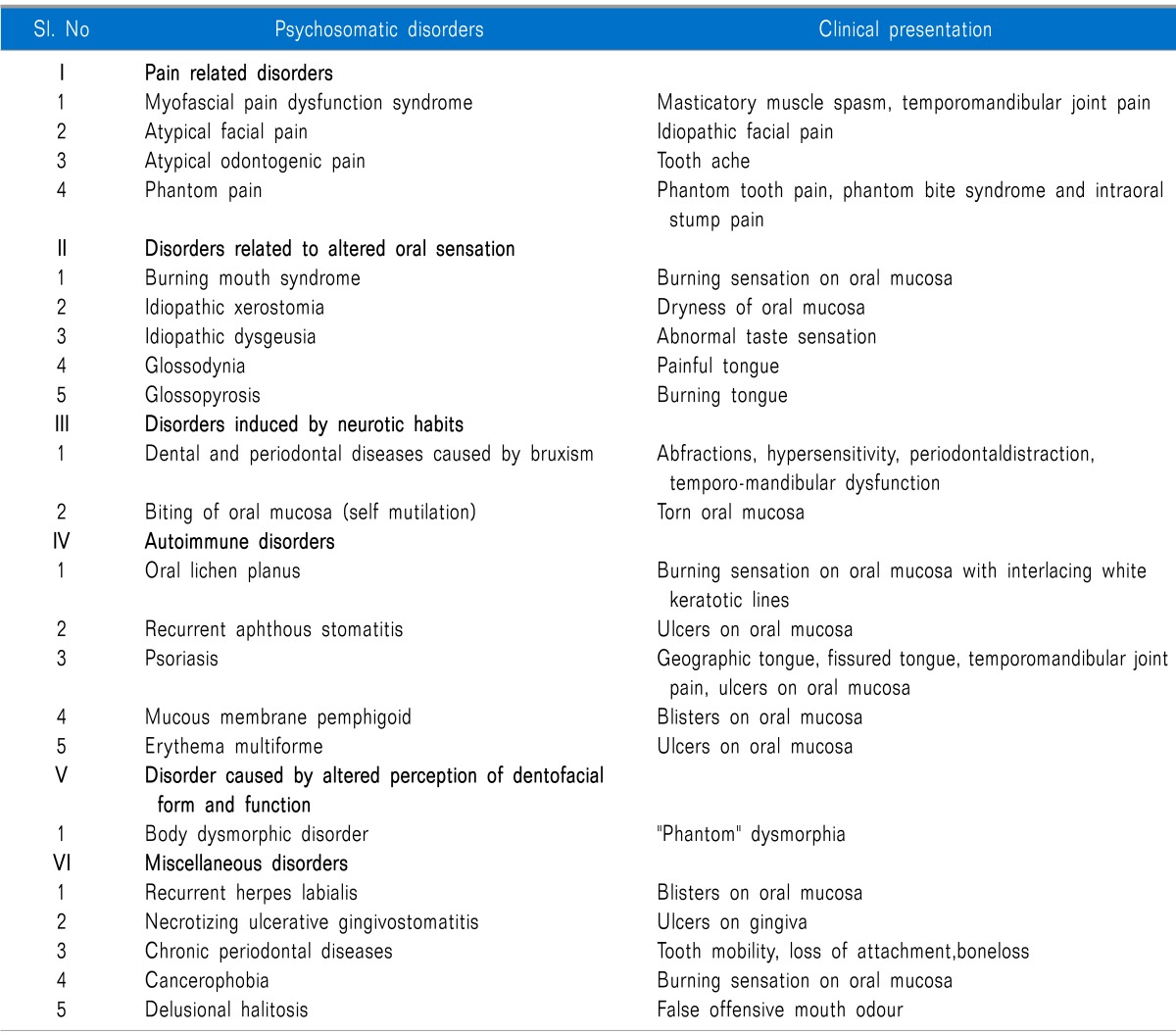
Future revisions and updates may be required with the further progress of time and knowledge. Body dysmorphic disorder (BDD) is a common psychological syndrome in dental practice which results in patients seeking treatment for an imagined defect in appearance [41]. Therefore, the author has added one more subset to the existing classification, i.e., V = Disorders caused by altered perception of dentofacial form and function, which include body dysmorphic disorder (BDD). After the inclusion of the subset (disorders caused by altered perception of dentofacial form and function), the terminology "psychosomatic disorders of the oral cavity" is modified to "psychosomatic disorders pertaining to dental practice". In the revised working type classification, miscellaneous disorders is shifted from V to VI with the addition of delusional halitosis under the miscellaneous disorders classification of psychosomatic disorders. A revised simple working type classification is proposed here for psychosomatic disorders pertaining to dental practice with their clinical presentation (Table 1).
Go to :
DISORDERS CAUSED BY ALTERED PERCEPTION OF DENTOFACIAL FORM AND FUNCTION
1. Body dysmorphic disorder (BDD)
Body dysmorphic disorder (BDD) is a psychological syndrome which results in patients seeking treatment for an imagined defect in their appearance [41]. Many patients present with a negative "feeling" about their exaggerated perception of a minimal dentofacial disorder of form and function or an also negative "phantom" dysmorphia. Aesthetic dental treatment for such patients is not beneficial and carries some potential risks [42].
Go to :
MISCELLANEOUS DISORDERS
Delusional halitosis
Halitosis or oral malodor or bad breath is a common concern for millions of people [43]. Delusional halitosis is a psychosomatic condition in which some individuals have the belief that they have an offensive mouth odor which neither the dental clinician nor any other clinician can perceive [44]. Delusional halitosis may be characterized as pseudo-halitosis or halitophobia, depending on the response to initial treatment.
Halitophobia is an olfactory reference syndrome and is a psychological condition that the dental surgeon is illequipped to treat alone. Delusional halitosis may present clinically as a spectrum ranging from an overvalued belief to a frank delusional disorder in which the individual can hardly be dissuaded from his or her belief of mouth odor; in other words the person will be presenting with false offensive mouth odor. Both Pseudo-halitosis and halitophobia patients must be referred to psychological specialists [45].
Go to :
CONCLUSION
To conclude, psychosomatic disorders pertaining to dental practice are presented here with a revised working type classification. In the revised working type classification, the terminology "psychosomatic disorders of the oral cavity" is modified to "psychosomatic disorders pertaining to dental practice". The psychosomatic etiology is already proposed for orofacial pain in dental practice [46]. Measures should be taken to incorporate this revised classification into the DSM-5 classification system and also to evaluate the validity of this classification.
Go to :
 XML Download
XML Download