

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The analgesic nefopam (NFP) is one of the drugs for which the mechanism-of-action target is unknown but can be predicted [1]. It was known as fenazocine and developed in the 1960s, and is widely used in European countries as a non-opioid, non-steroidal, centrally acting analgesic drug that belongs to the benzoxazocine chemical class [2,3,4,5]. It has been used most commonly to treat acute postoperative pain; therefore, most studies on NFP were focused on its analgesic potency compared to those of opioids or non-steroidal anti-inflammatory drugs (NSAIDs).
However, we know that its mechanisms of analgesic action are similar to those of triple receptor (serotonin, norepinephrine, and dopamine) reuptake inhibitors and anticonvulsants [1]. Thus, NFP can be beneficial to treat neuropathic pain in addition its effect on nociceptive pain based on these analgesic mechanisms of action.
In this paper, we will discuss several aspects of NFP, including the brief history and analgesic mechanisms of action, its clinical application and the adverse reactions (ADRs), and future directions for research.
Go to : 
BRIEF HISTORY OF NEFOPAM
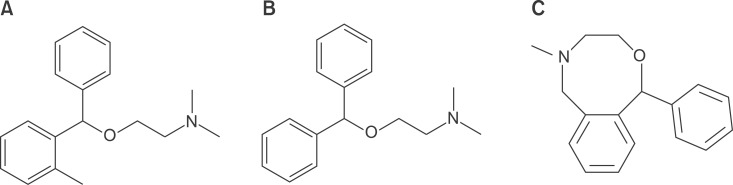
Nefopam, previously called fenazoxine, is a benzoxazocine derivative structurally related to orphenadrine and diphenhydramine (Fig. 1) [4]. The systemic name is 5-methyl-1-phenyl-1, 3, 4, 6-tetrahydro-2, 5-benzoxazocine, and the chemical formula is C17H19NO.
The only paper related to fenazocine we found available was "Studies on the peripheral pharmacology of fenazocine, a potential antidepressant drug" written by Bassett et al. [6] in 1969. The paper reported the drug inhibits the uptake of catecholamines in a manner similar to that of desmethylimipramine.
The name fenazocine was changed to nefopam in the early 1970s. Starting at this time, the paradigm of most studies about this newly renamed drug had shifted from a muscle relaxant [7,8] or an antidepressant [8,9] to an analgesic [10,11,12,13,14]. However, most of the studies have ignored NFP's role as an analgesic.
On the other hand, the use of NFP in the prophylaxis and treatment of shivering has been studied since early 1990s [15,16]. Its effect on shivering, defined as the body's physiologic response to cold exposure and preserve heat by peripheral vasoconstriction, has been compared with various drugs, such as meperidine, tramadol, clonidine, and ketamine. Clinically, shivering is noticeable as involuntary and uncoordinated skeletal muscle contractions that increase metabolic activity generating heat and elevating the core body temperature [17].
Intravenous infusion of NFP has been used to treat severe hiccups as a synaptosomal neurotransmitter reuptake inhibitor, a muscle relaxant, and an activator of the descending pain-modulating pathways in the case of non-responders with chlorpromazine and lidocaine since 2000. Hiccups, brief bursts of intense inspiratory activity involving the diaphragm and inspiratory intercostal muscles, with reciprocal inhibition of the expiratory intercostal muscles, might result from structural or functional disturbances of the medulla or of the afferent or efferent nerves to the respiratory muscles [18,19,20].
Go to :
ANALGESIC MECHANISM
1. Animal model of nociceptive pain
Nociceptive tests in animals can be divided into groups based on the responses to electrical, thermal, mechanical, or chemical stimuli [21]. In contrast, animal models of neuropathic pain can be divided into peripheral nerve injury models, central pain models, and drug- or disease-induced neuropathy models [22].
There are 2 phases in the formalin test: the first phase is a direct effect of formalin on the nociceptors, lasting for the initial 5 minutes, while the second phase is caused by inflammation of the affected area, starting from 20 to 30 minutes after injection. NSAIDs and steroids inhibit only the inflammatory second phase, while acetylsalicylic acid and acetaminophen are antinociceptive in both phases. The latter 2 drugs have some actions independent of their inhibition of prostaglandin synthesis and effects on non-inflammatory pain. NFP, a centrally acting analgesic, like opioids is antinociceptive in both phases. NFP also reduces the noxiously evoked spinal c-Fos protein expression in the early phase of nociceptive processes [23,24,25].
Using plate and plantar tests to demonstrate a withdrawal reflex mediated supraspinally and antinociceptive activity, NFP showed potent property to reduce thermal hypersensitivity after acute postoperative pain in rats [26].
Moreover, when injected before a surgical plantar incision, NFP reduced the exaggerated postoperative pain induced by perioperative fentanyl treatment and prevented the development of long-term pain hypersensitivity. Further, preoperative NFP administration also improved morphine analgesic efficacy in the context of fentanyl-induced postoperative hyperalgesia. Tissue damage associated with surgery often produces peripheral and central sensitization that may outlast the stimuli, leading to exaggerated postoperative pain. Paradoxically, the use of opioid analgesia, which is essential for surgical pain management, may induce pain sensitization leading to enhanced postoperative pain and an increased risk of developing chronic pain [27].
2. Postoperative pain in patients
A meta-analysis for randomized, placebo-controlled trials of NFP for the prevention of postoperative pain in human patients showed 3 main findings. Firstly, NFP, when used in adults undergoing surgery, has a morphine-sparing effect in the postoperative period. Secondly, it decreases pain intensity. Lastly, it increases the risk of tachycardia and sweating. In conclusion, NFP is used with opioids and NSAIDs as a multimodal approach for postoperative analgesia [4,28,29]. Moreover, it does not have any effects on respiratory and hemostatic functions, but is devoid of antipyretic properties [30]. The centrally-acting antinociceptive effect of NFP may be explained by its activation of triple monoamines descending inhibitory pathways and its antihyperalgesic activity by modulation of glutamatergic transmission [31].
3. NFP for neuropathic pain
To summarize the studies related to the basic mechanisms for the treatment of neuropathic pain from the early development as fenazocine to current NFP, the dual analgesic mechanisms of action, namely, a) descending pain modulation by triple neurotransmitter reuptake inhibition similar to antidepressants, and b) inhibition of long-term potentiation mediated by NMDA from the inhibition of calcium influx like gabapentinoid anticonvulsants or blockage of voltage-sensitive sodium channels like carbamazepine, enable NFP to be used as a therapeutic agent to treat neuropathic pain.
1) NFP for neuropathic pain: an antidepressant property
The classic tricyclic antidepressants have been used for the treatment of neuropathic pain due to the following 6 basic mechanisms: (1) blockage of norepinephrine, serotonin, or dopamine reuptake, (2) blockage of sodium channels, (3) antagonism of NMDA glutamate receptors, (4) sympathetic blockage, (5) effects on the visceral mechanosensitive afferent nerve fibers, and (6) effects on mood [32].
Experimentally confirmed primary binding profile for NFP have recently been proven to be serotonin receptor 2A transporter (1,685 nM), serotonin receptor 2B transporter (330 nM), serotonin receptor 2C transporter (56 nM), other serotonin transporters (29 nM), dopamine transporter (531 nM), and norepinephrine transporter (33 nM) (Table 1, Fig. 2) [1,33].
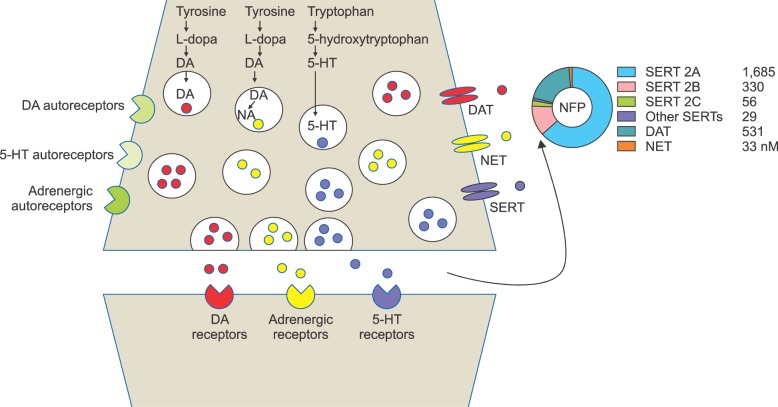 | Fig. 2Schematic presentation of dopamine (DA), noradrenalin (NA), and 5-hydroxytryptamine (5-HT) synaptic terminals drawn in the same neuron. In human body, they are actually located in the different neurons and locations: (1) The dopamine transporter (DAT) expression is dominant in the cell bodies of the substantia nigra and ventral tegmental area: (2) The noradrenalin transporter (NET) expression is abundant in the locus coeruleus and other brain stem nuclei; (3) The 5-HT transporter (SERT) expression is frequently found in the median and dorsal raphe nuclei. They are also found peripherally, especially in the dorsal root ganglia related to descending inhibition of pain. Monoamine transporters are localized to presynaptic sites, where they are crucial for the termination of monoamine transmission and the maintenance of presynaptic monoamine storage. Nefopam (NFP) has an ability of these 3 receptors reuptake inhibition (Modified from Torres GE, Gainetdinov RR, Caron MG. Plasma membrane monoamine transporters: structure, regulation and function. Nat Rev Neurosci 2003; 4: 13-25.).
|

2) NFP for neuropathic pain: an anticonvulsant property
NFP can inhibit calcium influx, intracellular formation of cGMP, and NMDA receptor-dependent neurotoxicity following the activation of voltage-sensitive calcium channels in vitro. Its presynaptic action reduces the excessive release of endogenous glutamate involved in neurological and neuropsychiatric disorders. Contrastingly, in some reports, nefopam blocks voltage-sensitive sodium channels and modulates glutamatergic transmission [34,35,36,37,38,39,40]. It has not yet been proven that the anticonvulsant activity of NFP originates from either the calcium, sodium, or both channels; however, NFP has a definite property as an anti-convulsant (Fig. 3).
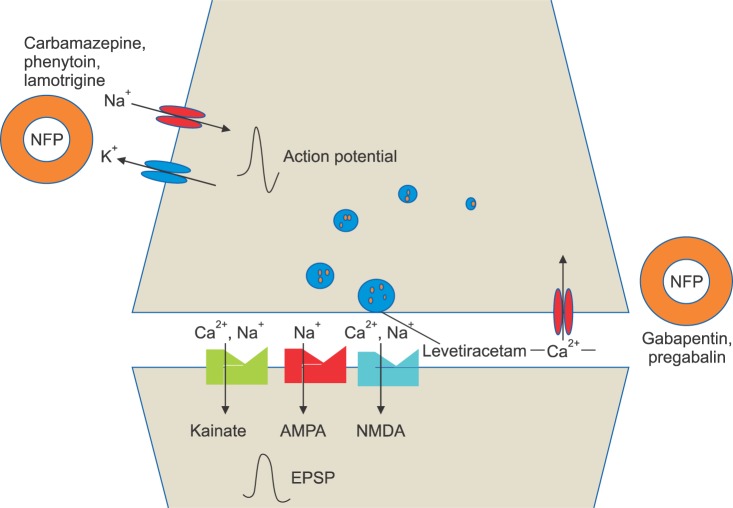 | Fig. 3Model synapse illustrating interaction of Na+ channel blocking anticonvulsants with voltage-activated Na+ channels and putative sites of action of newer anticonvulsants (gabapentin, pregabalin, and levetiracetam) that may more directly interact with release machinery. Gabapentin and pregabalin bind to α2-δ, which may inhibit voltage-activated Ca2+ entry through high voltage-activated Ca2+ channels or affect the way in which Ca2+ channels interact with vesicular release. Levetiracetam may also affect release by binding to synaptic vesicles protein SV2A. In contrast, action potentials are mediated by voltage-activated Na+ and K+ channels; Na+ channel blocking anticonvulsants suppress epileptiform action potential firing, which leads to inhibited release. Smaller yellow circles represent glutamate within synaptic vesicles (larger blue circles) and free in the synaptic cleft. Glutamate acts on ionotropic receptors of the NMDA, AMPA and kainate types to generate an excitatory postsynaptic potential (EPSP) in the postsynaptic neuron. Nefopam (NFP) shows an activity of the inhibition of long-term potentiation mediated by NMDA from the inhibition of calcium influx like gabapentinoid anticonvulsants or blockade of voltage-sensitive sodium channels like carbamazepine (Modified by Löscher W, Schmidt D. New Horizons in the development of antiepileptic drugs: Innovative strategies. Epilepsy Res 2006; 69: 183-272.).
|
Go to :
THREE POTENT NEUROTRANSMITTERS IN THE HUMAN BODY
The 3 potent neurotransmitters (serotonin, norepinephrine, and dopamine) have their own functions: (1) serotonin relates to cognitive impulse control and relaxation, obsession and compulsion, and memory; (2) norepinephrine relates to alertness, concentration, socialization, and energy; (3) dopamine relates to pleasure, pain avoidance, sense of inner and outer reality, reward, and motivation (Fig. 4) [41].
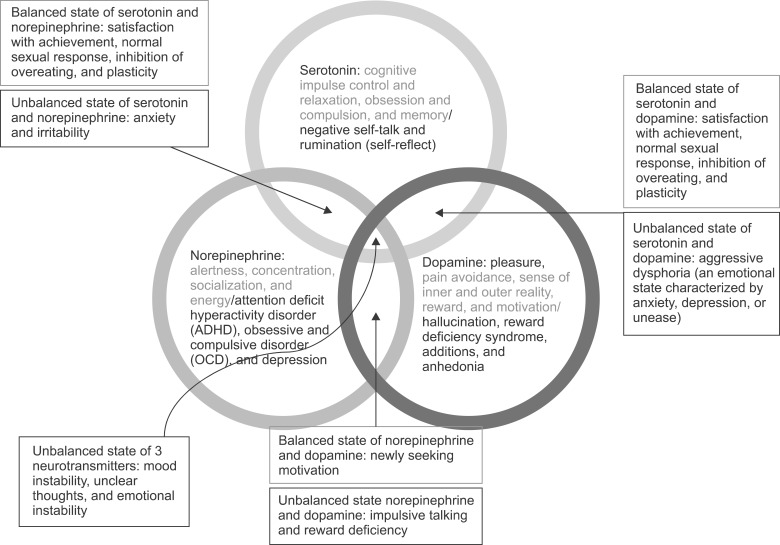
A well-balanced state of serotonin and norepinephrine leads to active socialization and normal sleep and appetite. A well-balanced state of serotonin and dopamine leads to satisfaction with achievement, normal sexual response, inhibition of overeating, and plasticity. A well-balanced state of norepinephrine and dopamine leads to newly seeking motivation.
An imbalance of these 3 neurotransmitters can lead to mood instability, unclear thoughts, and emotional instability. Imbalance of serotonin causes negative self-talk and rumination (self-reflect). An imbalance of norepinephrine can cause attention deficit hyperactivity disorder (ADHD), obsessive and compulsive disorder (OCD), and depression. An imbalance of dopamine can cause hallucination, reward deficiency syndrome, additions, and anhedonia (inability to experience pleasure).
An unbalanced state of serotonin and norepinephrine can lead to anxiety and irritability. An unbalanced state of serotonin and dopamine can lead to aggressive dysphoria (an emotional state characterized by anxiety, depression, or unease). An unbalanced state of norepinephrine and dopamine can lead to impulsive talking and reward deficiency.
1. Serotonin receptors
There are 7 families of serotonin (5-hydroxytryptamine, 5-HT) receptors. Most of the receptors are a group of G protein-coupled receptors (GPCRs), however the 5-HT3 receptor is a ligand-gated ion channel (LGIC), found in the central and peripheral nerve systems. The serotonin receptors modulate the release of many neurotransmitters, including glutamate, GABA, dopamine, epinephrine/norepinephrine, and acetylcholine, as well as many hormones, including oxytocin, prolactin, vasopressin, cortisol, corticotropin, and substance P, among others. The serotonin receptors influence various biological and neurological processes such as aggression, anxiety, appetite, cognition, learning, memory, mood, nausea, sleep, and thermoregulation. The serotonin receptors are the target of a variety of pharmaceutical and illicit drugs, including many antidepressants, antipsychotics, anorectics, antiemetics, gastroprokinetic agents, antimigraine agents, hallucinogens, and entactogens [42,43,44,45].
2. Adrenergic receptors
The adrenergic receptors (or adrenoreceptors), a class of metabotropic G protein-coupled receptors that are targets of the catecholamines, especially norepinephrine (noradrenaline) and epinephrine (adrenaline). There are two main groups of adrenergic receptors, α and β, with several subtypes [46].
3. Dopamine receptors
Dopamine receptors are a class of metabotropic GPCRs that are prominent in the vertebrate central nervous system (CNS). Dopamine receptors are implicated in many neurological processes, including motivation, pleasure, cognition, memory, learning, and fine motor control, as well as modulation of neuroendocrine signaling. Abnormal dopamine receptor signaling and dopaminergic nerve function is implicated in several neuropsychiatric disorders. Thus, dopamine receptors are common neurologic drug targets; antipsychotics are often dopamine receptor antagonists while psychostimulants are typically indirect agonists of dopamine receptors. There are at least five subtypes of dopamine receptors, D1, D2, D3, D4, and D5. The D1 and D5 receptors are members of the D1-like family of dopamine receptors, whereas the D2, D3 and D4 receptors are members of the D2-like family. There is also some evidence that suggests the existence of possible D6 and D7 dopamine receptors, but such receptors have not been conclusively identified [47].
Therefore, a balance between descending controls, both excitatory and inhibitory, can be altered in various pain states. There is good evidence for a prominent α2-adrenoceptor-mediated inhibitory system as well as 5-HT3 (and likely also 5-HT2) serotonin receptor-mediated excitatory controls originating from brainstem and midbrain areas [45].
Go to :
NEUROPATHIC PAIN SCALES
Neuropathic pain is defined as pain arising as a direct consequence of a lesion or disease of the peripheral or central nervous system affecting the somatosensory system. There are several pain scales for assessment of neuropathic pain [48]. NFP is considered to be a drug for the treatment of neuropathic pain based upon its analgesic mechanism; therefore, future studies related to NFP should be performed with an assessment of neuropathic pain scale. Therefore, it is recommended, for the patients who have neuropathic pain and are NFP recipients, to check the "The neuropathic pain symptom inventory", such as a) the neuropathic pain scale (NPS), b) the neuropathic pain symptom inventory (NPSI), c) the Leeds assessment of neuropathic symptoms and signs (LANSS), d) the Neuropathic pain questionnaire (NPQ), and Douleur neuropathique 4 (DN4).
Go to :
CLINICAL APPLICATION and ADVERSE REACTIONS
1. Clinical application
Administration of nefopam should be administrated as a single dose of 20 mg intravenously at a slow rate for 15-20 min or with continuous infusion of 60-120 mg/d due to known adverse effects, such as nausea, cold sweating, dizziness, tachycardia, or drowsiness. The usual dose of oral administration is three to six times totaling 90-180 mg/d. However, it might have a ceiling effect as a previous study revealed that additional doses up to 90 mg did not result in greater pain relief [27,29].
NFP is a potent analgesic compound administered as a racemic mixture. Previous in vitro and in vivo studies with NFP enantiomers have shown that (+) NFP is substantially more potent than (-) NFP. There are no significant differences in area under the concentration curve (AUC), the maximum concentration (Cmax), or half-life between enantiomers following intravenous administration. Based on these findings, there is currently no compelling rationale to justify administering or monitoring individual enantiomers [49].
2. Adverse reactions
From the analysis of the French Pharmacovigilance system, the most frequent ADRs included 'expected' ADRs such as sweating, nausea, tachycardia, malaise or vomiting and 61 'unexpected' ADRs. No overdose was reported; 26 ADRs (23%) were considered as 'serious'. Most of the ADRs were 'unexpected' included neuropsychiatric (hallucinations, convulsions) or cutaneous (pruritus, erythema, urticaria). Six cases of anaphylactic ADRs (two angioedema and four anaphylactic shocks) were reported, all occurring shortly after use of nefopam during the post-operative period. Physicians should be aware of the possible occurrence of some serious ADRs when using nefopam especially when the drug is used in special medical conditions such as post-operative periods [50].
If NFP is given in single doses of 20 mg slowly over 15-20 min or with continuous infusion of 60-120 mg/d, complaints of the ADRs and the need to stop the administration are rare. It is also rare to observe ADRs with the usual dose of oral administration with three to six times per day totaling 90-180 mg with a titration. Similarly the same level of attention should be given towards ADRs when antidepressants and anticonvulsants are administrated due to their potential ADRs.
Go to :
CONCLUSIONS
The recently discovered dual analgesic mechanisms of action enable NFP to treat chronic neuropathic pain by modulating the descending pain pathway via triple neurotransmitter reuptake inhibition (similar to antidepressants) and the inhibition of long-term potentiation mediated by NMDA (from the inhibition of calcium influx like gabapentinoid anticonvulsants and/or blockade of voltage-sensitive sodium channels like carbamazepine).
In the setting of acute postoperative pain, we think that is can be helpful to use it for surgical insults that result in developing neuropathic pain. In such setting, as part of multimodal approach, NFP may be suitable for the application as intravenous patient controlled analgesia using its different class analgesics, such as opioids and NSAIDs. However, studies have to be done to investigate this property. It is also helpful to treat hiccups and to prevent postoperative shivering.
During the titration of oral administration for neuropathic pain, there are only a few parenteral medications for breakthrough pain (BTP) currently. Neither NSAIDs nor opioids provide substantial relief of intractable BTP. Intravenous nefopam could be an effective parenteral agent for BTP during the titration of oral medication for neuropathic pain in a hospital setting. Further, it can be easily converted from parenteral to enteral routing before patients are discharged from the hospital.
Moreover, NFP may be helpful to the patients who have already reached maximal doses of anticonvulsants and antidepressants, or who cannot escalate the dosage of these drugs due to hepatic or renal problem or their ADRs. Again, all the above possible applications must be studied to collect evidence before NFP is routinely used in a clinical setting.
Go to :
 XML Download
XML Download