

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Knee problems are the cause for which a large number of patients are referred to pain clinics. Due to its nature of complex movements, the knee is extremely sensitive to anatomic and functional derangements which can result from even small changes such as arthritis or injury to cartilage or ligaments [1]. Given that the knee has a complex structure, inflammation of one bursa can cause significant dysfunction, pain, and sometimes infection of the entire knee [2].
Although in most cases, the pes anserine bursa lies beneath the pes anserine tendon, which is the insertional tendon of the sartorius, gracilis, and semitendinosus muscles on the medial side of the tibia, it can have other anatomic positions as well. Due to the unique anatomic connections in the medial part of the knee, it is often hard to detect the anatomic structure which is the cause of a patient's pain by clinical examination [3]. Patients suffering from pes anserine bursitis experience pain in the medial part of the knee. Generally, it is difficult to diagnose pes anserine bursitis by physical examination. Use of common diagnostic modalities such as plain X-ray, MRI, and electromyography for the diagnosis of pes anserine bursitis is time-consuming, and injection into the bursa without image guidance is associated with considerable complications [4,5]. In recent years, the ultrasound technique has played a crucial role in increasing the accuracy and efficacy of neuraxial and peripheral nerve blockade as well as joint injection by both decreasing the rate of complications and improving our anatomic knowledge [6-8].
Therefore, this study was performed to evaluate sonographically the visibility and positions of the pes anserine bursa and its adjacent anatomic structures. In addition, the location of the saphenous nerve was also examined because it is in close vicinity to the pes anserine tendons of the medial part of the knee.
Go to : 
MATERIALS AND METHODS
After approval of the study protocol by the Institutional Review Board, 170 asymptomatic volunteers between 15 and 80 years of age and of ASA class I or II were enrolled in this study after providing informed consent. Exclusion criteria were: volunteer's withdrawal at any time after the submission of informed consent, congenital or acquired structural malformation, localized infection, knee pain, history of knee surgery, and any type of knee injury.
Following preparation, the volunteers were placed in the supine position with the knee bent at a 5 to 10 degree angle and ultrasound imaging was performed on the medial part of the knee. The sonography device was MicroMaxx (SonoSite, Inc., USA), and we used a linear array probe with 6-13 MHz frequency, with penetration depths of 2.5, 3.1, or 4 cm according to the volunteer's body mass index (BMI). The sonographic study was performed by an expert physician on both knees of the volunteers. For ultrasound visibility, we set criteria as follows: invisible (cannot detect), poor (detection of tendons and saphenous nerve), moderate (detection of tendons, pes anserine bursa, and saphenous nerve), and well (detection of tendons, pes anserine bursa, saphenous nerve, and medial collateral ligament). To prevent bias, all ultrasound examinations were performed by one pain physician while image evaluation was performed by another pain physician.
The gathered data were recorded by the first physician on previously composed sheets including demographic data such as age, weight, height, BMI, and gender, while anatomic indicators regarding the pes anserine bursa and the saphenous nerve were recorded by the second physician. The data were statistically analyzed using SPSS software version 18. The chi-square test was used for comparison of the frequency of the bursa position.
Go to :
RESULTS
The demographic data is shown in Table 1. No relationship was detected between BMI and sonographic visibility of the anatomic structures.
The position of the bursa in males was between the pes anserine tendons and the tibia in 67.1% of cases, between the medial collateral ligament and the pes anserine tendons in 21.2%, and between the pes anserine tendons in the right knee in 8.2%, and in some cases it was not visible. There were no significant differences between males and females in the position of the pes anserine bursa (Table 2).

Comparison of the location of the saphenous nerve between males and females showed that the nerve lies between the pes anserine tendons (intratendinous position) in 77.6% of male and female volunteers and outside the pes anserine tendons (extratendinous position) in 18.8% of males and 15.3% of females (P = 0.18), and in some cases it was not visible (Table 3). No differences between males and females were observed in the frequency of visibility of sonoanatomic structures including the pes anserine tendons, the pes anserine bursa, and the saphenous nerve (Table 4).


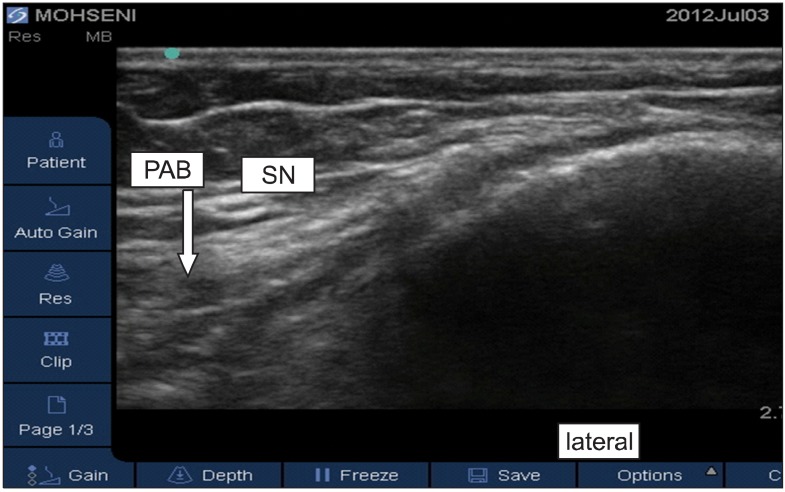
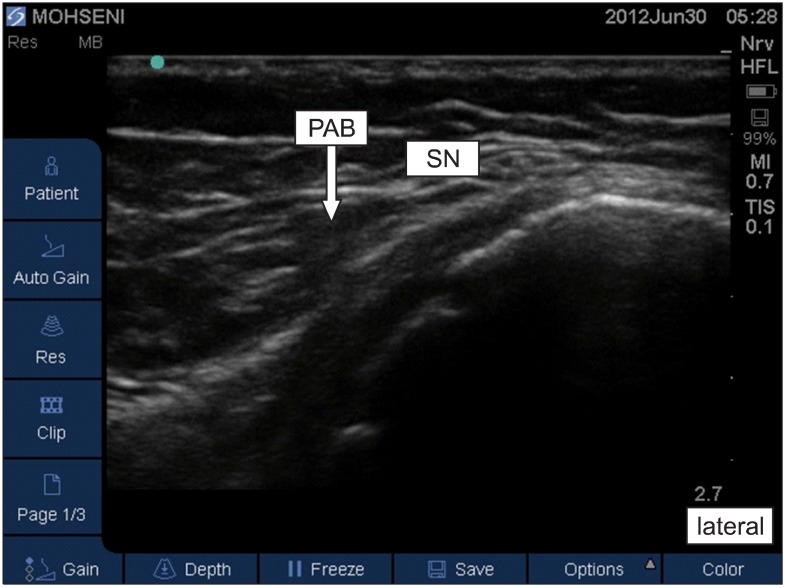
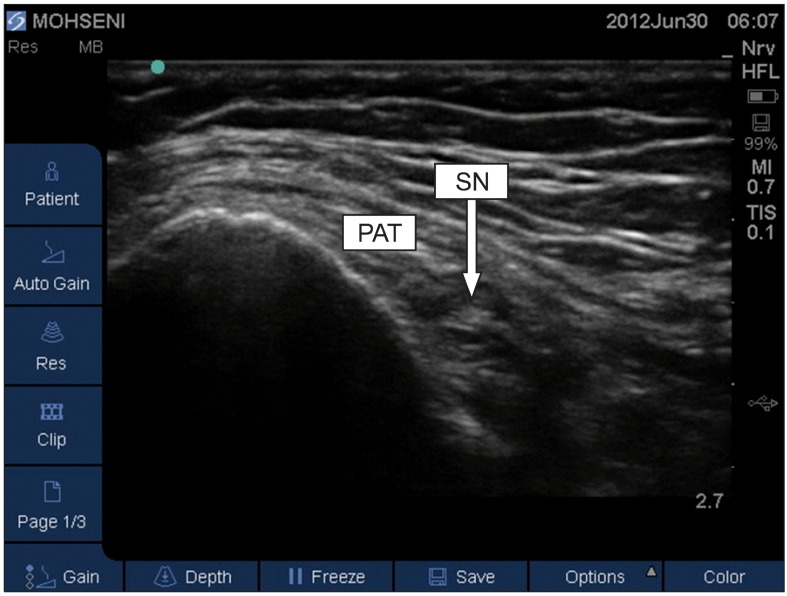
Out of 170 volunteers, one 40-year-old woman had pes anserine bursitis and felt moderate pain when the sonography probe was placed on the medial part of her left knee (Fig. 1). On examination of the knee of one 38-year-old man, thickening of the pes anserine tendon was observed. The subject gave a history of mild pain upon walking down slopes (Fig. 2). Other sonoanatomic variations are shown in Fig. 3-6.
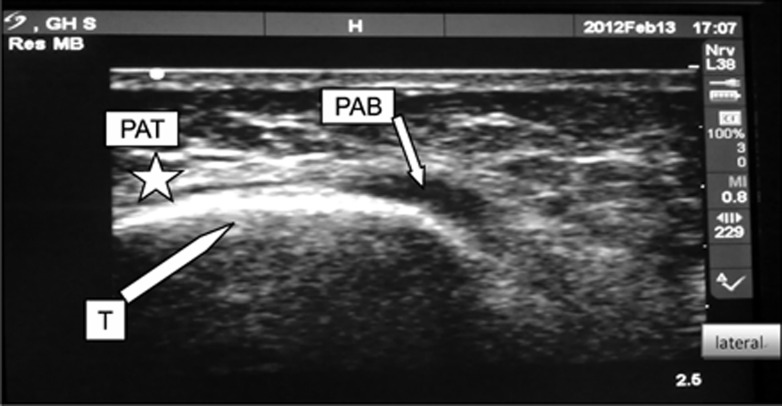 | Fig. 1Fluid filled pes anserine bursa (PAB) indicates the presence of bursitis. T: border of tibia, PAT: pes anserine tendons (asterisk).
|
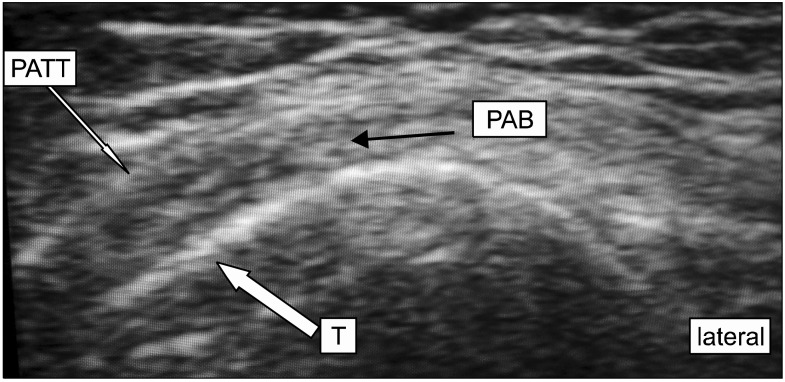 | Fig. 2Thickening of pes anserine tendons is shown. PATT: pes anserine tendon thickening, T: border of tibia, PAB: pes anserine bursa.
|

Go to :
DISCUSSION
In clinical practice, bursitis is one of the most common causes of knee pain [9]. Knee bursae including the pes anserine bursa are prone to injuries from both acute traumas and continuous micro traumas [10,11]. The pes anserine bursa has been described by most sources to lie beneath the pes anserine tendon, which is the insertional tendon of the sartorius, gracilis, and semitendinosus muscles on the medial side of the tibia, but it can lie between the pes anserine tendons and the medial collateral ligament of the knee [12].
Pain from inflammation of the pes anserine bursa worsens with passive internal rotation and active external rotation of the knee. Activity, especially external rotation and flexion of the knee, aggravates the pain [13]. Therefore, it can be mistaken for delicate pressure fractures, degenerative joint disease, meniscus injury, medial collateral ligament injury, non-specific medial meniscus cysts, paratibial cysts, semimembranosus bursitis, pes anserine tendonitis, and entrapment of the saphenous nerve [14]. Although magnetic resonance imaging is helpful in ruling out problems such as tumors and other injuries, it is not a cost-effective modality for diagnostic injection into the pes anserine bursa [15].
According to the study of Finnoff et al. [16], blind injection into the pes anserine bursa has a high failure rate. In that study, the accuracy of ultrasound for correct injection into the pes anserine bursa was 92% (correct injections 11 out of 12), while only 17% of injections performed without ultrasound guidance correctly entered the bursa (correct injections 2 out of 12). In addition, a case of pes anserine tendonitis diagnosed by sonography in a 45-year-old woman who presented to the emergency room with acute severe pain in the medial part of her knee was also reported [17].
In recent years, the ultrasound technique has played a crucial role in increasing the accuracy of peripheral nerve blockades, knee joint injections, and diagnosis of rheumatologic diseases [18-20]. Considering the prevalence of knee pain and the importance of diagnostic injections for pes anserine bursitis, as well as the results of this study, which demonstrated that demographic characteristics such as age, gender, and BMI do not influence the visibility of sonoanatomic structures, ultrasound can be considered an effective modality in diagnostic and therapeutic injection in the pes anserine bursa.
In the present study, although the pes anserine bursa lies in its usual position, which is between the tibia and the pes anserine tendons, in 67.1% of subjects, it is also found between the pes anserine tendons and the medial collateral ligament in 21.2%, and between the tendons of the sartorius, gracilis, and semitendinosus in 8.2%. This anatomic variation may lead to incorrect injections inside the tendon while attempting blind injection into the bursa. Information on the variation in location of the bursa and tendons is mandatory in performing injection therapy because correct injection into an inflamed bursa can help to reduce inflammation, but an inaccurate injection into a tendon may lead to tendon weakness and atrophy and higher risk of tendon rupture. On the other hand, entrapment of the saphenous nerve in the medial part of the knee is an important consideration in the differential diagnosis of pes anserine bursitis [21,22]. According to the results of this study, which reported the position of the saphenous nerve as intratendinous in 77.6% of cases and extratendinous in 18.8% of cases, we would assume that sonography can be used to find and block the saphenous nerve either for local surgical procedures or for treating nerve entrapment.
Finally, based on the results of this study, as a domestic survey on the target patients, and considering the evidence provided by previous studies reporting the accuracy of sonography in finding the position of the pes anserine bursa, ultrasonography can be used as a valuable and rapid method to assist in diagnostic and therapeutic procedures on the medial part of the knee. However, utilization of ultrasound for chronic pain interventions is still in its relatively early stages, and additional studies are required to further evaluate the efficacy and limitations of employing this modality [23].
Go to :
 XML Download
XML Download