

 PDF
PDF Citation
Citation Print
Print


FBSS is a condition in which symptoms do not change or worsen after surgery for a spinal abnormality, or the patient experiences difficulties in everyday life. For FBSS, no procedures can effectively control pain, and the pain becomes chronic. The pathogenesis of this syndrome has not been clearly elucidated; however, it is known to be from epidural adhesion, physical compression of peripheral nerves, and nerve root damage developing after spinal surgery [1].
Epiduroscopic laser discectomy and neural decompression is performed percutaneously, so it is advantageous that the epidural space can be visualized in 3 dimensions and in color with minimal invasiveness. Through this, the pathologic and normal anatomical structures can be differentiated, and drug therapy or detachment of the scar tissue can be performed on specific areas. ELND is known to be an effective procedure for intractable lumbar pain and radiating pain developing after lumbar surgery, as well as for herniation of the intervertebral disk, spinal stenosis, and internal disc disruption.
However, various complications can arise after the procedure such as epidural abscess, hematoma, nerve damage, increased cranial pressure, arachnoid cysts, and blindness. Rarely, cranial nerve palsy can occur from increased cranial pressure due to the normal saline used for perfusion. This possibility can increase further when dural puncture occurs accidentally while trying to go through the adhered band or scar tissue. From the cranial nerves, the trochlear nerve is the nerve with the lowest ratio of palsy, but when it happens on one or both sides, it causes vertical diplopia and blurred vision [2,3]. Hence, the authors are reporting a case of trochlear nerve palsy which occurred as a complication of ELND, together with a relevant literature review.
CASE REPORT
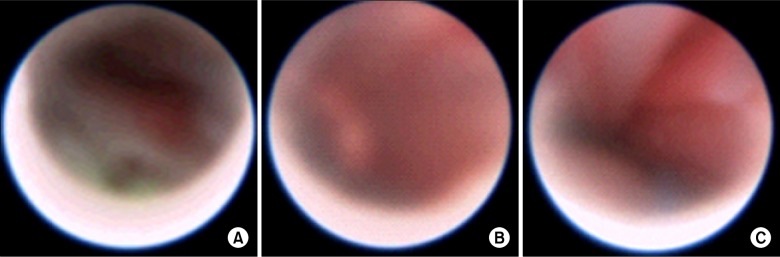
The patient was a 64-year-old female who had received spinal surgery (lumbar laminectomy L4-5) 25 years ago according to her past medical history. There were no abnormalities in her family and personal history. She complained of back pain occurring when standing up from a sitting position as the main symptom. In another hospital, drug administration, epidural block, and lumbar facet joint block were performed for the above symptom but there was no great effect. According to the physical exam, there were no abnormalities in the SLR test and FABER test, while spinal tenderness and paraspinal muscle tenderness were observed. There were no abnormalities found in the blood test, chest PA, and EKG performed before the procedure. In the epidurogram performed while hospitalized, there was suspicion of epidural adhesion and fibrosis in the operated area of the L4-5 so ELND was scheduled. The patient was put in a prone position and a pillow was placed under the pelvis to reduce lumbar lordosis and assist punctuation. The patient was changed to a reverse Trendelenburg position and the area surrounding the sacral cornu was draped with potadine solution and chlorhexidine solution. Midazolam 3 mg and fentanyl 50 ug were injected when performing local anesthesia for the caudal approach, and saturation was monitored while maintaining mild sedation. The video guided catheter was inserted in the caudal approach and contrast agent was used to check that it had entered the anterior epidural space. Using the endoscope as a guide, the catheter was inserted towards the L5-S1. Cold saline was used for irrigation to avoid vision obstruction from bleeding and foreign substances, and for adhesiolysis using hydraulic pressure. The patient complained of pain when the catheter was climbing towards the operated area (L4-5) through the anterior epidural space and when performing adhesiolysis so fentanyl was injected 50 ug at a time. In the L4-5 area, adhesiolysis was performed on the left side (holmium YAG laser was used after confirming the dural position) and while moving the catheter towards the right, an unintended dural puncture occurred. The amount of saline inserted in the intrathecal to secure a field of vision was 5 cc (Fig. 1). The procedure was completed immediately after confirming endoscopic entrance into the intrathecal, and the patient was cared for in the recovery room for 20 minutes before being transferred to the ward. The total amount of saline inserted including the epidural space was 120 cc, and the injection speed was 1 cc/sec. The total amount of fentanyl injected was 300 ug. The vital signs were normal in the recovery room, and there were no neurological symptoms such as headache. After moving to the ward, the patient complained of vertical diplopia and blurred vision, and through collaboration with ophthalmology, the patient was diagnosed with bilateral trochlear nerve palsy. There were no abnormalities such as bleeding observed on the brain MRI, and according to the f/u for 6 months after discharge, the blurred vision improved.
Go to : 
DISCUSSION
When the epidural space is expanded in the spinal canal, dural displacement occurs and the cerebrospinal fluid inside is pressurized. The subarachnoid space, including the cerebrospinal fluid, is liberally connected to all sections of the neuraxis. When performing ELND, saline is generally used to secure the field of vision from blood or foreign bodies and to open the epidural space. Due to this injection, the cerebrospinal fluid pressure of the spinal cord increases, and this also affects the pressure in the brain [4]. The increased cranial pressure is due to increased epidural pressure from the saline injection, and this pressurizes the dural sac and leads to a cephalad shift of the cerebrospinal fluid [5]. This change in cranial pressure is directly applied to the cranial nerves which can stretch or pressurize the cranial nerve, and this can lead to nerve damage [2]. The physiologic ICP range is known to be 5-10 mmHg [6]. According to Hilt et al. [5], when bupivacaine 10 ml is injected into the epidural space, the increase in cranial pressure starts a few seconds after starting the injection, and it continues to increase 35-45 seconds after stopping the injection. The maximum cranial pressure appeared to reach 63 mmHg, and it took 2-5 minutes to return to the baseline cranial pressure. Hilt et al. reported that the increase was greater when the initial cranial pressure was higher [5]. The epidural space is a "leaky reservoir" with characteristics of being collapsible, distensible and resisting inflow [7]. The degree of fluid leaking into the epidural space depends on how open the intervertebral foramen is [8]. In spinal stenosis patients with disc bulging in the spinal canal and a thickened ligament flavum, the resist inflow is increased [9]. The patient in this case had severe adhesion from surgery, and ligament flavum hypertrophy and disc protrusion were observed in the level above the operated area (Fig. 2). In a situation where leakage into the intervertebral foramen is obstructed due to adhesion and disc protrusion, and the spinal canal has been narrowed from spinal stenosis on the upper level, injection of saline can cause an excessive increase in the cranial pressure. Furthermore, there is a more direct effect when the fluid is directly added to the subarachnoid space due to the dural puncture [10]. Pressure can be directly affected by the injection rate and volume [11] so it is advised that the injection does not exceed 1ml per 1-2 seconds [4]. In addition, to prevent increased cranial pressure from stagnant saline, it is better to keep the injection site of the catheter open. Additionally, it is helpful to position the patient in the reverse Trendelenburg position.

Until now, there have been no case reports regarding the occurrence of trochlear nerve palsy after ELND. However, the etiological factor can be inferred from cranial nerve palsy cases caused by intracranial hypotension or hydrocephalus which occurs from changes in cerebrospinal fluid pressure. According to Zada et al. [12], cranial nerve palsy from intracranial hypotension occurs as abducens (6th) nerve palsy in 83% of cases, oculomotor (3rd) nerve palsy in 14%, and trochlear (4th) nerve palsy in 7% of the cases. Isolated trochlear nerve palsy, which does not include other nerves, is known to be extremely rare [13]. The clinical symptoms of trochlear nerve palsy can originate from peripheral and central lesions. A peripheral lesion is when nerve fascicles are damaged, and a central lesion occurs from damage to the trochlear nucleus. Depending on the time of occurrence, acute occurrence is due to trauma or disease, while chronic occurrence is possibly due to congenital reasons. The trochlear nerve has the longest intracranial distance (about 75 mm) from the cranial nerves so it is vulnerable to various traumas. The trochlear nerve nucleus is located at the pons level. The axon comes out of the nucleus and goes downward from the tegmentum to the pons and then, abruptly changes direction dorsalward and goes to the superior medullary velum. Here, the nerves intersect horizontally and continues in the opposite direction. For the case in this study, the palsy was caused by the increase in cerebrospinal fluid pressure pushing the brainstem to the back and pressing the superior medullary velum. Momentary stretching or compression of the nerves can also cause palsy.
Here, the authors report the occurrence of trochlear nerve palsy after ELND. In FBSS patients, the cerebrospinal fluid pressure can greatly increase so saline should be gradually and slowly injected. Considering that fentanyl 300 ug can cause excessive sedation which prevents the patient from noticing symptoms of increased internal pressure during the procedure, the patient should not be too sedated and there should be monitoring for symptoms from increased cranial pressure.
Go to :
 XML Download
XML Download