

 PDF
PDF Citation
Citation Print
Print


Myofascial pain syndrome is a common disease. The main treatment includes injection therapy at the trigger point and medication in which an analgesic anti-inflammatory agent and muscle relaxant are administrated together. Trigger point injection (TPI) is widely applied since it is effective in most cases and easily performed on outpatients. However, the duration of pain relief may, in some cases, be short. Hence, many patients return to the clinic as outpatients when the analgesic effect diminishes. TPI may be used many times, but repetitive TPI may be rejected because of its cost and the fact that it relies on a needle injection. Some patients consider TPI as a temporary treatment method. Therefore, we report on a myofascial pain syndrome case where direct pulsed radiofrequency treatment was applied to the trapezius muscle on which TPI had been sufficiently effective but of short duration. Moreover, the analgesic effect of the pulsed RF treatment was maintained for a considerable duration.
CASE REPORT
A 47-year old female patient visited our clinic with the main complaint of neck pain that had become severe over the past year. The medical history showed that the patient was undergoing psychiatric treatment for depression and had been diagnosed with ossification of the posterior longitudinal ligament (OPLL) for neck pain that had continued for 15 years. One year before visiting our clinic, she had undergone an operation in a neurosurgery clinic. The symptom did not significantly improve after the surgery and the pain continued. Thus, she underwent continuous rehabilitation therapy and physical therapy under the diagnosis of failed back surgery syndrome.
When the patient came to the clinic, she complained of tearing pain concentrated in the neck and both nuchal regions. This pain became more severe when the patient was doing more than the usual household chores. The visual analogue scale (VAS) score of the pain was as high as 8 and was accompanied by sleep disorders. The physical examination showed pain during neck flexion and extension as well as direct tenderness at both trapezius muscles and the levator scapular muscle.
A simple C-spine X-ray test and a laboratory test found no explanation for the pain. TPI was then performed, under the assumption that the myofasical pain syndrome originated in the trapezius and the surrounding muscles. Medication for failed back surgery syndrome was suggested, but the patient rejected it since the previously used analgesic anti-inflammatory agent had had no effect on her and she was taking an antidepressant and other drugs. Hence, as an outpatient,a small dose (12.5 µg/hr) of fentanyl patch (Durogesic D-trans®, JanssenPharmaceutica N.V, Tumhoutseweg, Belgium), which is a narcotic analgesic, was given, and TPI was performed on the trapezius muscle.
When the patient returned as an outpatient after the treatment, the patient stated that the VAS score had decreased from 8 to 4-5 for 2-3 days following the TPI but later returned to previous levels. The patient did not show any side effects from the fentanyl patch. TPI was repeated three times, but the pattern of improvement for 2-3 days and exacerbation, thereafter, continued. Treatment methods such as botulinum toxin injection were considered but pulsed RF treatment to the trapezius muscle was performed first due to its lower cost and the fact that it could be used in outpatient treatment.
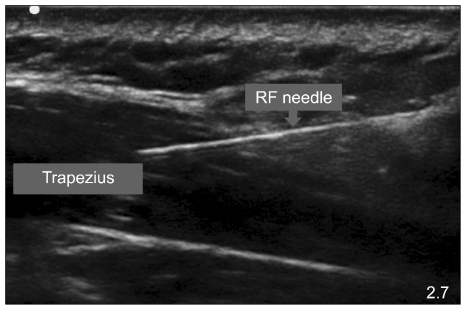
Following betadine disinfection in the prone position, the accurate trigger point was located by means of an additional physical examination. Then, skin wheal infiltration was performed with local anesthetics. To verify the accurate needle position, 10 cm-RF needles (22 gauge, straight, 5 mm active-tip) were inserted into both trapezius muscles under ultrasound (S-nerve, Sonosite®, Bothell, WA, USA) guidance. Following sensory stimulation performed at 50 Hz with a potential less than 1V, pulsed RF (PMG230, Baylis medical company Inc, Montreal, Quebec, Canada) treatment was performed two times for each muscle (120 s, 20 ms, 2 Hz, 42℃, impedance below 400 ohms) (Fig. 1).
When the patient returned as an outpatient one week after the pulsed RF treatment, the pain at both nuchal regions was much relieved as reflected in the VAS score of 1-2. This pain relief was continuously maintained. Thus, we decided to use only the fentanyl patch. Since the VAS score has been in the range of 2-3 for about two months after the pulsed RF treatment, TPI is no longer performed.
DISCUSSION
RF thermocoagulation is a method of pain treatment that has been used for more than 30 years. The basic principle is to prevent nociceptive input using the thermocoagulation of nerve tissues. Recently, another hypothesis suggested that the pain analgesic effect of RF thermocoagulation is not only caused by tissue destruction but also by the strong magnetic field that is formed around the treated region [1]. Pulsed RF treatment, which is used as an alternative to nerve destruction, employs the same frequency as RF thermocoagulation. However, the difference is that pulsed RF uses a high voltage energy burst for 20 msec to reduce nerve destruction compared to RF thermocoagulation uses heat that causes nerve destruction by increasing tissue temperature. Thus, pulsed RF treatment has been used in the treatment of dorsal root ganglion, medial branch, or peripheral nerves. However, it has been rarely used to treat myofascial pain [1].
Myofascial pain is a common pain syndrome. However, long-term treatment of this pain is difficult [2]. Traditional treatment includes using local anesthetics (including steroids) injection at trigger points, dry needling, physical therapy, and behavior modification. However, the duration of pain relief is often less than a few days or weeks. Thus, although various methods have been suggested for prolonged analgesia, none has been found to perform significantly better than another [2].
Pulsed RF treatment was performed at muscles trigger points to produce prolonged analgesia. Significant analgesia was obtained for three months after the patient received pulsed RF treatment at both trapezius regions. There is no explanation exists as to why pulsed RF treatment has a longer pain relief effect. In case of TPI or dry needling, analgesic effects are brought by a complex mechanism of a stimulus to cutaneous Aδ nerve fiber by needling, a stimulus to C-fiber by local anesthetics injection, and an alteration of around the trigger point various chemical environments (cytokine, substance P, etc.,) which induces pain [2]. Pulsed RF is known to be involved in the expression of the c-fos gene at lamina I and II in the dorsal horn at the neurobiological level [3,4]. The c-fos gene expression encourages the formation of preprodinorphin, which is the second RNA messenger. This results in an increased production of endorphin that modulates analgesic action [5]. Thus, the change in the gene expression caused by pulsed RF may reflect an inherent change in the dorsal horn, which may cause a prolonged analgesic effect [6]. Additionally, the strong magnetic field formed during pulsed RF treatment might reduce the transmembrane potential of the micro-nerves (Aδ fiber or C-fiber) in or around the muscle, which might have also affected the neuronal environment and thereby influenced the analgesic effect and duration by means of the thermal field effect in tissue [7]. Further studies need to be conducted to compare the analgesic effect and duration of TPI and pulsed RF treatment to the muscles in the same regions.
In conclusion, pulsed RF treatment has the advantage of not destroying neurons and producing less pain. It can also give a longer analgesic effect than conventional treatment methods when applied to myofasical pain. Pulsed RF treatment is cost-effective in view of its use in repeated outpatient visits. More prospective randomized controlled trial studies are necessary to compare its effectiveness with TPI treatment.
 XML Download
XML Download