

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Clinically, various antidepressants and anticonvulsants have been used for the management of neuropathic pain [1,2]. Among antidepressants, tricyclic antidepressants (TCAs) have been used most commonly, but its anticholinergic, antihistaminergic, and cardiovascular effects limit their usage [2]. Therefore, newly developed antidepressants, such as selective serotonin reuptake inhibitor (SSRI) and serotonin norepinephrine reuptake inhibitors (SNRI), have been tried to reduce such side effects.
Milnacipran is known as a balanced SNRI with minimal side effects and broad safety margin [3,4]. Intrathecally-administered milnacipran shows an antiallodynic effect in animal models [3,5-8]. The action site of milnacipran may be the spinal cord [3]. By administration of milnacipran directly to spinal cord, its dosage can be significantly lowered compared to oral or parenteral route, which could decrease side effects and increase the effectiveness of the drug [9]. However, there is no animal study on the neurotoxicity of neuraxial milnacipran. Although oral milnacipran has been used safely in clinical settings [4], its safety should be substantiated by preliminary animal studies for the intrathecal or epidural administration in clinical settings [10,11]. The aim of this study was to evaluate the neurotoxicity of epidural milnacipran in rats.
Go to : 
MATERIALS AND METHODS
The experimental protocol was approved by Institutional Animal Care and Use Committee of Seoul National University Hospital. Sixty-nine male Sprague-Dawley rats with mean body weight of 180.0 ± 23.8 g were used. The rats were acclimated to the housing facility (2-3 rats/cage, 12-h light/dark cycle) for 1 week. Food and water were provided ad libitum.
Rats were anesthetized by placing in a closed box containing 3% sevoflurane in oxygen (3 L/min) with spontaneous ventilation. After three minutes and confirmation of conscious loss, anesthesia was maintained with 2-3% sevoflurane in oxygen via a self-manufactured mask. The rats were placed in a prone position. After sterile dressing, epidural catheterization was performed as previously described with some modifications [12-16]. A 2-3 cm midline skin incision was made around the L6 level and the spinous process of the L6 was removed. Using fine microscissors, a small epidural puncture was made at the center of the ligament flavum just below the base of the lamina of the L5 and a PE-10 catheter (Natsume, Japan) was inserted and advanced approximately 3 cm (measured on the surface before the catheter insertion) cranially. The catheter tip was placed at the L1 level [12,17]. The knot was tied with 3-0 Vicryl™ to fix the catheter firmly in place.
The rats were excluded if blood or cerebrospinal fluid was aspirated thorough the cathter. To confirm the correct position, 0.15 ml of 2% lidocaine was injected through the catheter and then the tip was sealed with a flame. After the complete recovery from anesthesia, a correct epidural catheter placement was defined as a condition in which the rats showed paralysis of the hind limbs while forelimbs showed normal motor functions. If the test solution extravasated through the sutured skin and the rats did not show paralysis of the hind limbs, those cases were excluded. If the test solution were injected intrathecally or intravasculary, sudden respiratory arrest or cardiac arrest would have been observed; such cases were also excluded. After confirmation of correct epidural catheter placement, we observed gait, spinal deformity, and behavioral abnormalities for 3 days. Rats that showed abnormalities during the observation period were excluded from this study.
At first, sixty nine rats were included. However, sixty male Sprague-Dawley rats, weighing 146-297 g, were successfully prepared for this study and divided randomly and equally into three groups. Under general anesthesia (as previously described), 3 mg (0.3 ml, 100 mg of milnacipran was dissolved in 10 ml of normal saline) of preservative free milnacipran (Bukwang Pharm. co., Ltd., Seoul, Korea) was injected over one minute via an epidural catheter in group M. In groups A and S, the same volume of 40% alcohol and 0.9% normal saline were injected, respectively. After recovery, rats were housed individually under a 12-h light/dark cycle.
Behavioral observation tests were performed to evaluate for acute toxicity at 1 and 3 days after the injection and chronic toxicity at 7 and 21 days. An examiner unaware of the study protocols evaluated the rats for motor and sensory deficits with the toe-pinch test and motor function evaluation (gait and hind foot deformity). Toe-pinch test was used to evaluate withdrawal reflex for nociception [14,18,19]. After deep pinching the hind foot sole with forceps for 6 seconds, an examiner observed the avoidance response. Stimuli were applied 3 times with 5-minute-interval on both soles. When the avoidance responses were observed in all periods, it was rated as normal and if not, as abnormal with a possible insult of sensory function, motor function, or both [18,19]. Through the examination of the posture and the gait, we can evaluate the proprioception, motor, sensory and autonomic function. If there is a lesion in the general proprioceptive system, rat shows sensory ataxic gait. Motor function was assessed using a previously devised scoring system with some modifications [14,20]. The grading was as follows: grade 1 = normal gait with no evidence of motor paresis; grade 2 = normal gait with slight hind paw deformity, such as plantar flexion of toes; grade 3 = slight gait disturbance with motor weakness and/or an inverted hind paw; and grade 4 = a prominent limping gait with a dropped hind paw. The rats with a motor disturbance of grade 2 or above were considered to have a motor deficit.
The spinal cord was harvested in 5 rats from each group on the 1st, 3rd, 7th and 21st days after the injection for histopathological evaluation of neural injury. Rats were sacrificed under general anesthesia, by intracardiac perfusion of 4% paraformaldehyde in 0.1 M phosphate buffer. 1 cm length of spinal cord, caudal and cranial to the catheter tip, was harvested and fixed with 10% neutral formalin solution. The spinal cord was then embedded in paraffin, cut into sections at a thickness of 4-5 µm, mounted, and stained with hematoxylin and eosin [21]. Microscopic analysis was focused on 4 aspects: vacuolation of dorsal funiculus, chromatolysis of motor neuron in ventral horn, neuritis, meningeal inflammation [13,14,22-24]. Vacuolation of dorsal funiculus was graded as follows: grade 0 = none, grade I = observed in less than 10% area of dorsal funiculus, grade II = observed in 10-50% area, and grade III = observed in more than 50% area [17]. In cases of chromatolysis of motor neuron, neuritis and meningeal inflammation, the existence was examined. One blinded pathologist examined all histological specimens.
Data are expressed as mean ± SD. Inter- and intra-group comparisons of body weights were analyzed using a RM-ANOVA followed by Duncan's method. Motor and sensory deficits, motor function and histopathological results were analyzed using Chi-square test between the groups if the cells whose expected frequency is less than 5 do not exceed 25% of cases. If they do exceed 25% of cases, Fisher's exact test was used between the groups. The level of statistical significance was set at P < 0.05.
Go to :
RESULTS
At first, sixty nine rats were included, but data were acquired from only sixty rats in the end. The reasons for exclusion of nine rats were as follows: Four rats were sacrificed soon after the injection of lidocaine due to arrest. Three rats in group A died before the end of the experiment. And, in two rats, pathological specimens have been lost.
In all groups, significant weight gain was observed during the study period (P < 0.001). However, rats in group A showed more slow weight gain than groups S and M from the 7th day (P < 0.05).
All rats in groups S and M responded normally to the toe-pinch test and showed normal motor function at each observation point. However, all rats in group A showed abnormal response to the toe-pinch test from the first day (P < 0.001, Table 1), and showed hind-paw deformity and a gait disturbance from the first day except two rats (P < 0.001, Table 2).
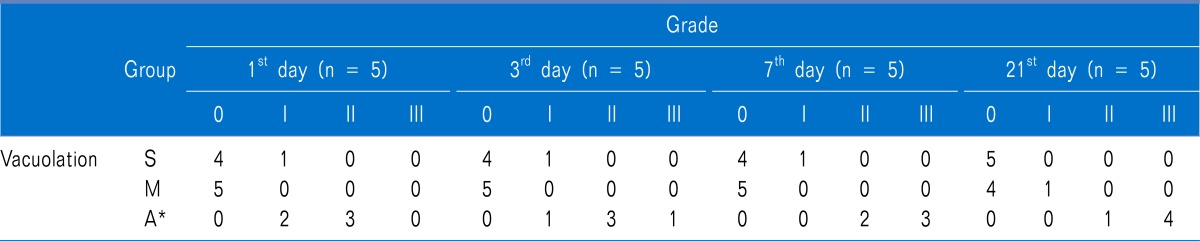
Table 1
Vacuolation in the Dorsal Funiculus of the Spinal Cord Under Microscopic Examination after Epidural Injection of Drugs
Values are expressed as number of positive rats out of the total. Group S: epidural injection of 0.3 ml of normal saline, Group M: epidural injection of 3 mg/0.3 ml of milnacipran, Group A: epidural injection of 0.3 ml of 40% alcohol. The grade of the vacuolation was assessed with a four-point scale; 0: no vacuolation, I: <10% area, II: 10-50% area, III: >50% area of the dorsal funiculus vacuolated. *P < 0.01 vs. groups S and M.
![]()
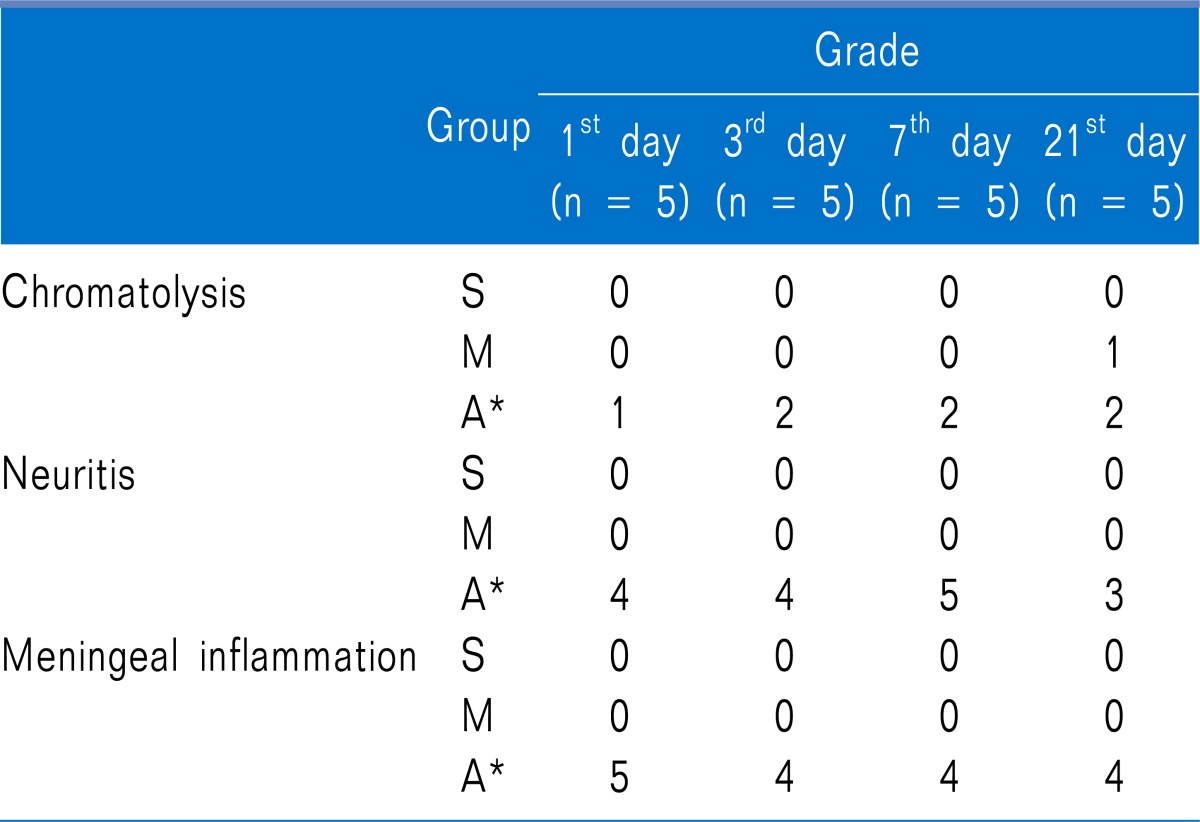
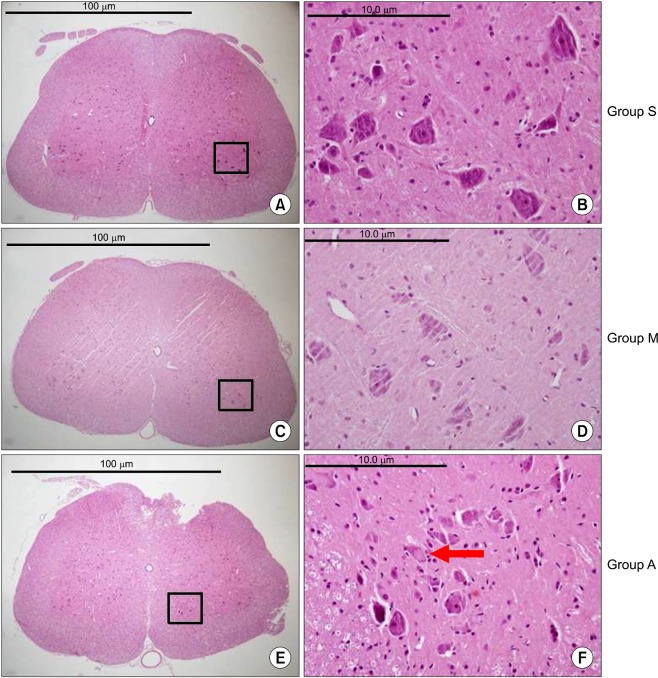
No statistically-significant lesions were observed through hematoxylin and eosin staining in group S or M at any time in the experimental period (P < 0.01, Fig. 1-4). However, in group A, specimens obtained at 1, 3, 7, and 21 days showed various neuropathies, such as vacuolation of the dorsal funiculus, chromatolysis of motor neuron, neuritis or meningeal inflammation (P < 0.01, Fig. 1-4).
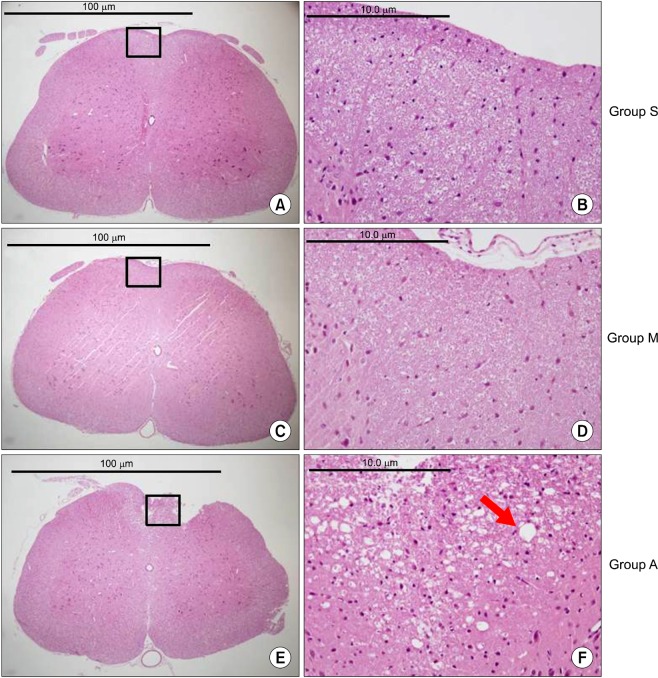 | Fig. 1Characteristic light microscopic appearances of vacuolation in the dorsal funiculus stained with hematoxylin and eosin from groups S (A, B), M (C, D) and A (E, F). Groups S and M show no vacuolation but, group A show severe (grade III) vacuolation in dorsal funiculus (indicated with red arrow). A, C, E: original magnification ×40. B, D, F: original magnification ×400.
|
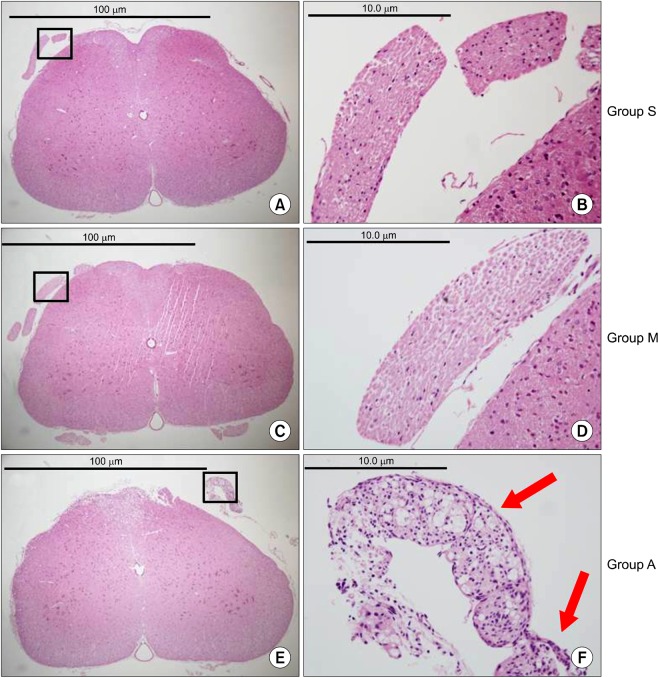
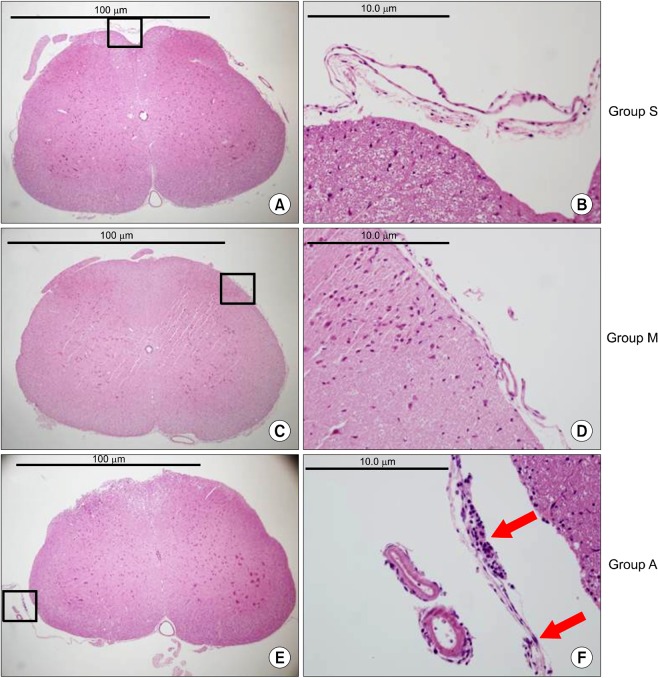 | Fig. 4Characteristic light microscopic findings of meningeal inflammation stained with hematoxylin and eosin from groups S (A, B), M (C, D) and A (E, F). In groups S and M, the meninges are thin and show no infiltration of inflammatory cells. However, in group A, the meninges are thickened and show heavy infiltration of inflammatory cells such as neutrophils (indicated with red arrow). A, C, E: original magnification ×40. B, D, F: original magnification ×400.
|
Go to :
DISCUSSION
The neurotoxicity of epidurally-administered milnacipran was investigated and our results showed that epidurally-administered milnacipran has no neurotoxic effects in rats.
Milnacipran reduced allodynia and hyperalgesia in chronic neuropathic pain model of a mice [6], but not in a nociceptive one [7]. Intrathecal administration of milnacipran had an anti-allodynic effect with the reduction of neuropathic pain, but not with any other routes of administration [3,5,8]. There has been a lot of evidence that milnacipran was more effective by direct spinal administration. Therefore, it postulated that both serotonin and norepinephrine reuptake inhibition must take place in the spinal cord for the antiallodynic effect of milnacipran [3]. If the medication's main effector site were spinal cord, direct neuraxial administration into the epidural or intrathecal space would be better than other routes. However, if there is any possibility of neurotoxicity with direct contact to the nerve, milnacipran cannot be administered by spinal route. In this study, epidural administration is used than intrathecal one. The reasons are like that; First, in this study, 2% lidocaine 0.15 ml was used for catheter confirmation but it can cause respiratory arrest if intrathecally. Second, there is a risk of inadvertent cord or nerve injury during intrathecal catheter placement [25,26].
Although the drugs are already commercially available for systemic administration and has been used safely, the toxic responses must be reconsidered when the administration route is changed [10,27]. The "minimal evidence guidelines required to support the use of drugs for intrathecal pain therapy" states that the preclinical evaluation about the physicochemical properties and animal studies is essential and must precede clinical (human) studies. The animal studies should provide information on the mechanism of action, site of action, pharmacokinetics, toxicity and efficacy. Moreover, the animal toxicology studies should include a maximum dosage and concentration [27].
Important factors in determining the drug dose used for the epidural neurotoxicity study are the concentration and volume. The drug concentration is the important contributor to the epidural neurotoxicity and the knowledge of the supramaximal concentration that does not induce neurotoxicity will set a safety criterion for the effective dose. Drugs were administered via a fine catheter into the epidural space (0.61 mm in external diameter). So, the study must be instituted with the recommended solubility to exclude the possibility of catheter occlusion by the solutes not dissolved completely. It is known that the solubility of milnacipran is 19 mg in 1 ml of saline, so the maximal dose of milnacipran that can be delivered epidurally is 5.7 mg in 0.3 ml of saline. In this study, we administered 3 mg of preservative free milnacipran in 0.3 ml of saline into epidural space. This 3 mg in 180 g-rat is equivalent to 17 mg/kg of epidural dose. The Food and Drug Administration has suggested that the extrapolation of animal dose to human dose is correctly performed only through normalization to body surface area. To convert the dose used in rats to one based on surface area for humans, multiply 17 mg/kg (epidural dose of the Rats) by the Km factor of 6 for a rat and then divided by the Km factor of 37 for a human [28]. Therefore, it is approximately equivalent to an epidural 196 mg in 70 kg-man. Considering that the required dose for the epidural route is about 1/10-1/30 of the dose for oral administration [29], the 3 mg of epidural milnacipran in rat may be equivalent to an oral administration of about 1,960-5,880 mg for a human adult. In addition, considering the fact that the maximal recommended dose per os for milnacipran is 200 mg in human adults [4], the maximal epidural dose calculated is 6.7-20 mg. A study by Mochizucki administered maximal 120 mg/kg of milnacipran per os with the neuropathic rat model; this 120 mg/kg of oral milnacipran is equivalent to 4-12 mg/kg epidural dose [6]. We believed this 3 mg of epidural milnacipran was sufficient for the evaluation of neurotoxicity in the rat because it was approximately 9.8-25.2 fold greater than clinically used doses in human adult and 1,700 times greater than previously reported maximal intrathecal dose of 1.0 µg/kg [8], and the Dura mater of small animals has greater diffusibility than that of the human [29,30]. Because no epidural neurotoxicity was seen in this study with a highly concentrated and supramaximal dose of epidural milnacipran, it can be speculated that there will be no epidural neurotoxicity within above-mentioned concentration and dose of epidural milnacipran in the clinical management of neuropathic pain.
Next, to consider is the volume of the drug. Choi et al. showed that 0.3 ml spreads to more than 10 segments of spinal column [14]. If the catheter tip were placed at the L1 level, the spread of milnacipran might range from the T9 cranially to L6 caudally. It would be sufficient to observe the sensorimotor changes of the hind foot.
We obtained the spinal cord at L1 level as a histopathological specimen because at that level the spinal cord would be exposed to the highest concentration of the drug for a longer time than any other levels. Additionally, neurotoxicity should be assessed by examining sensory, motor, and behavioral changes. The symptoms and signs of neuronal damage might exist even in the absence of histological changes [31] and vice versa [32]. Therefore, both the behavioral and the histopathological studies are crucial. In this study, all rats in group A exhibited reduced activity and appetite, poor weight gain, and acute and chronic neurotoxicity findings upon histopathological examination, all of which could be considered as sequela of alcohol-induced neurotoxicity [33-35]. But, all rats in group M and S, showed no sensorimotor deficits and did not show statistically-significant abnormal histopathological findings during the study. Although statistically insignificant, three specimens in group S showed grade I vacuolation at day 1, 3, 7 and one specimen in group M at day 21. The exact mechanisms are not clear, but the infection from the external source, the irritation of contaminant or the physical damage during the catheterization might be responsible factors for the abnormal findings rather than the epidurally-administered drug itself [25,26].
We used an alcohol as a positive control because it destroys all neuronal components such as axon, glial cell and myelin sheath [36,37]. Considering the fact that usually 33% alcohol is used clinically for neurolysis and the study by Lee [17] that 30% alcohol did not cause any abnormal behaviors, we used 40% alcohol in this study.
In conclusion, epidurally-administered milnacipran in rats did not cause sensory, motor, behavioral, and histopathological changes that suggest neurotoxicity. This results implicates that milnacipran could be administered directly via the epidural route in a clinical setting. However, similar studies in larger species are required to obtain reliable safety data on the epidural application of milnacipran before use in clinical settings.
Go to :
 XML Download
XML Download